We Now Know How The Government Lied About the COVID Vaccines
For more than 250 years, the same playbook has been used to prop up toxic vaccines. At long last, we have a chance to end it.

Story at a Glance:
Since the dawn of vaccination, authorities have habitually doubled down on unsafe and ineffective vaccines, regardless of the pushback they received or the evidence against them.
Sustaining this has required increasingly brazen methods to censor and conceal the deluge of “extremely rare” injuries caused by an ever-expanding vaccination schedule.
Senator Ron Johnson, who has worked tirelessly to expose this coverup, recently held a Senate hearing aptly titled: “Unmasked: How Biden Health Officials Purposely Turned a Blind Eye Toward COVID-19 Vaccine Safety Signals.”
Faced with a tsunami of vaccine injuries too large for anyone to ignore, the FDA and CDC searched for a way to statistically dismiss it, eventually settling on effectively comparing Moderna’s injury rate to Pfizer’s and declaring the vaccines “safe” because there was no major difference between the two.
When a senior FDA analyst pointed out this obvious flaw and suggested comparing them to less toxic vaccines instead, documents show the entire FDA turned against her to suppress her findings. As a result, dozens of conditions we have all seen the COVID vaccines cause were never officially linked to them—despite the data clearly showing they were.
The unprecedented damage caused by the COVID-19 vaccines has created a historic loss of trust in the parties who covered it up, giving us a once-in-a-lifetime opportunity to force them to start telling the truth and end an immunization experiment that has profoundly damaged the health of our society.
I have long believed in a “law of equilibrium” which posits that most things are cyclical and will eventually be brought back into balance. Mechanistically, this frequently results from existing phenomena being the result of competing forces reaching a balance point (e.g., you don't fall through the floor because the ground pushes up on you just as hard as gravity pulls you down) and because nature’s design utilizes feedback loops to maintain balance.
This process is commonly referred to as “negative feedback,” where anything that shifts a system away from its center (e.g., its “set point”) triggers a response that counteracts that change (e.g., a thermostat kicks on the heat when the temperature drops too low, or turns on the AC when it climbs too high). Biology in turn, has many layers of these negative feedback loops (where one thing counteracts another which counteracts another etc.) which collectively are able to keep the immensely complex orchestra of life functioning.
Conversely, “positive feedback loops” also exist, where a shift from baseline triggers a further shift from baseline (e.g., forest fires spreading, fruit ripening, the blood clotting cascade, the hormonal surge triggering ovulation, or childbirth contractions) but these are far rarer and ultimately still “turn off” because they rapidly consume a self-limiting resource.
Due to the cyclical nature of history, I have noticed the same vaccine fiascos repeat again and again, but each time, are forgotten, and hence able to repeat again. Briefly, the process is typically as follows:
•A new (dubious) vaccine is introduced and marketed with immense fanfare despite the existing evidence showing it does not deserve that fanfare.
•Once the vaccine hits the population, a significant number of vaccine failures and injuries inevitably occur.
•Once this happens, health authorities (and healthcare workers) respond by exaggerating the benefits, moving the goal posts from what was originally promised, and sweeping all the injuries under the rug.
•This produces increasing pushback from the public and resistance towards vaccinating.
•As time goes on, rather than acknowledge the shortcomings of the vaccine, the failures of the vaccine begin being increasingly blamed not enough people vaccinating (e.g., to reach “herd immunity”). As such, more and more aggressive mandates are instituted which create stronger and stronger public resistance against the program.
I named this the “vaccine positive feedback loop” because if things were functioning normally, the injuries and failures of the vaccine would trigger a negative feedback response that would cause the vaccine program to be pulled back—but instead a rather curious and unnatural thing occurs—the devotion to them increases. This I believe cuts to the core of why “vaccines are a religion” and why vaccine proponents will always double down on what they are doing rather than admit fault.
Recognizing that this is a recurring cycle, my focus hence has been on exposing the cycle, as I feel it is only through the knowledge of what our society is actually trapped in that it will be possible to free ourselves from it.
Note: a major reason I've focused on umbrella therapies like DMSO is that their mechanisms of action are in many ways the inverse of what vaccines do, which provides a concrete way to understand why so many different vaccines can cause such a wide range of neurological and autoimmune injuries. This for example was why my recent article on DMSO treating “incurable” neurological injuries had to be so detailed, but now that that has been done, a much shorter version which references the more extensive summary can be published (and will be).
Reducing “Vaccine Hesitancy”
One of the most depressing facets of the “vaccine positive feedback loop” is how consistently both doctors and government officials will sweep vaccine injuries under the rug to maintain public confidence in the vaccine, with the earliest example I’ve found being one that Suzanne Humphries unearthed:
Mr. Henry May, writing to the Birmingham Medical Review, in January, 1874 reported that deaths as a result of vaccination were often not reported because of an allegiance to the practice. Often a vaccinated person was recorded as having died from another condition such as chicken pox or erroneously listed as unvaccinated.
Polio Coverups
When producing the original (Salk) polio vaccine, manufacturers faced a delicate balance: the live poliovirus had to be fully inactivated with formaldehyde to ensure safety, but excessive inactivation could damage key viral antigens and weaken the immune response. This required a series of careful steps to strike an appropriate balance and during the clinical trials, three different parties (Salk, the US government and the manufacturers) tested the vaccines for safety.
Once the vaccine was approved, changes were made to the vaccine to increase potency (a preservative was removed), inactivation protocols became much more lax (increasing potency), and testing was delegated to manufacturers (despite large deviations from Salk’s inactivation protocols)—all of which was essentially done to meet the large demand for the polio vaccine as the trial approach was not feasible to implement at scale.
As a result, on April 12th (based on the recent clinical trials), was declared “safe, effective, and potent,” and licensed the same day. The next day, widespread vaccinations began, and around April 24th polio began being reported in recipients, ultimately causing 40,000 recipients to develop non-paralytic polio, 200 to develop paralytic polio and 10 to die.
To solve this public relations nightmare (which given previous assurances greatly shook public confidence in vaccines), the US government chose to blame it on faulty manufacturing from one of the five producers (who recalled their vaccines) but stand behind the other four. However, to quote Turtles All the Way Down (and Paul Offit):
Alexander Langmuir, the CDC’s chief epidemiologist, and Dr. Neil Nathanson, who at the time headed the CDC’s polio surveillance unit. The two conducted a follow-up investigation into the Cutter Incident and discovered that Wyeth’s vaccine had also caused several cases of paralysis. Following their report, the company silently recalled the allegedly “hot lot” from the market. No one other than senior US health officials ever saw that report.
“It was never released to the media,” Offit writes, “never shown to polio researchers, never shown to the National Foundation, never shown to polio vaccine advisers, never distributed to health care professionals, never published in medical journals, and never made available to defense attorneys in subsequent lawsuits against Cutter Laboratories. As a result, only a handful of people knew about the problem with Wyeth’s vaccine.”
Years later, Nathanson said he thought the report had been buried due to officials’ wish to maintain public confidence in the Salk vaccine: “As long as the problem was with one manufacturer [i.e., Cutter] and a couple of lots of vaccine, it would be viewed as an aberration due to sloppy manufacturing or testing procedures and not an intrinsic problem. Once it was extended to a second manufacturer, it would be seen as intrinsic to the product.” In this scenario, Offit further clarifies, ”people would be afraid to use any polio vaccine.”
Likewise, after a panel was convened to investigate the disaster:
Perhaps the most disturbing element of the entire program, has been the disparity between the risks that were known to be involved and the repeated assurances of safety.—Paul Meier, professor of epidemiology at the Johns Hopkins University School of Public Health
The National Foundation, in a memo sent to doctors, also stated emphatically that the [polio] vaccine was completely safe and that the risk of ensuing paralysis was “zero”.
The best way to push forward a new program is to decide on what you think the best decision is and not question it thereafter, and further, not to raise questions before the public or expose the public to open discussion of the issue.—Paul Meier (sarcastically) speaking at an expert panel on the polio vaccine.
Finally, in 1984, amid tort litigation raising technical questions about whether the original 1961–1962 clinical trial lots met the monkey neurovirulence test standards, the FDA loosened the clinical trial requirements for licensure so that any remaining regulatory doubts about the vaccine’s safety would not undermine the immunization program. Their announcement, in turn, was quite explicit:

Leaked transcripts have also revealed this mentality. For example, in a private June 2000 meeting, the CDC, WHO and vaccine manufactures discussed Verstraeten’s CDC analysis showing mercury in vaccines had a dose-dependent association with neurodevelopmental disorders. Expressing concern the study had ever been done, the WHO’s representative stated “My mandate as I sit here in this group is to make sure at the end of the day that 100,000,000 are immunized… and that will have to be with thimerosal containing vaccines unless a miracle occurs,” urging the group to present findings to the ACIP in a way that would not get “exposed to the traps which are out there in public relations.” Another warned that “the medical legal findings in the study, causal or not, are horrendous,” while the meeting’s own chairman, Dr. Dick Johnston, admitted, “I do not want my grandson to get a thimerosal-containing vaccine until we know better what is going on.” The study was stamped “DO NOT COPY OR RELEASE” on every page, and over the next three years the data was reworked until the significant associations largely disappeared in the version published in Pediatrics in 2003—by which time Verstraeten had left the CDC for GlaxoSmithKline.
Note: it should come as no surprise that despite decades of attempts to access this study's underlying database, the CDC has blocked every single one, leaving us to having to trust that their in-house analyses always correctly determined safety.
Likewise, Gavin Debecker’s Forbidden Facts, was written to expose leaked transcripts from the IOM’s closed Immunization Safety Review Committee meetings—which were tasked with definitively evaluating vaccine safety but instead prioritized downplaying risks to avoid eroding public confidence and triggering vaccine hesitancy. Committee members repeatedly framed their approach around protecting vaccination uptake. For example, Dr. Michael Kaback stated, “The more negative that presentation is, the less likely people are to use vaccination… We are kind of caught in a trap.” Dr. Bennett Shaywitz warned that any “waffling” could lead parents to opt for single vaccines [which are safer but less profitable], noting “everybody knows that that is going to reduce the vaccinating of children.” Dr. Steven Goodman emphasized they had to be “very, very careful” about quantifying side effects, lest it be seen as an “ideologic bias” harming public trust. This mindset shaped their wording and conclusions toward reassurance rather than full scientific transparency.
Looking into the present, as doubts about vaccines have continued to increase, the messaging on every platform has shifted to the urgent need to “reduce vaccine hesitancy” by censoring any information about serious adverse effects of vaccination. Given that Peter Marks (the FDA bureaucrat who was essentially in charge of the COVID vaccines and stonewalled all investigations into their harms) frequently publicly spoke out against vaccine misinformation and the dangerous vaccine hesitancy it caused, I suspected the longstanding tradition to bury vaccine injuries to preserve public trust in vaccination was alive and well throughout COVID-19. To quote the recent Senate investigations:
Records that the Subcommittee has obtained to date [5/21/25] offer a simple, yet troubling, answer to these questions: Biden administration officials knew in early 2021 that the mRNA COVID-19 injections could result in adverse health events and they downplayed the risks [e.g., myocarditis] to avoid alarming the public and create vaccine hesitancy. As a result, they violated what should be the inviolable principle of informed consent [and mandated the vaccine for virtually every American].
By May 2021, senior officials in the FDA’s CBER (the unit responsible for COVID-19 vaccine safety surveillance), drafted an email to Dr. Szarfman [who was providing evidence of serious vaccine harm], directing Dr. Szarfman to “hold off on creating and sending data mining reports and analyses.” Dr. Peter Marks, a staunch supporter of the COVID19 vaccines who at the time led CBER [and had told Szarfman to cease and desist in her activities], eventually warned [Dr. Szarfman’s boss] that Dr. Szarfman’s data mining could “create erroneous conflicts that feed in to anti-vaccination rhetoric.
Exposing the Coverup
Senator Johnson has spent more than four years working around the clock, regardless of the pushback he receives, to expose the COVID cartel and help those injured by its greed. In doing so, he has, for the first time, provided conclusive evidence that authorities habitually lie about vaccines, which I believe is necessary to finally break the toxic cycle we are trapped within.
Recently he held a hearing to present what his Senate investigative team had unearthed, a few parts of which I’d like to highlight. First, in his opening statement, he concisely lays out conclusive proof that the FDA and CDC compulsively covered up COVID vaccine injuries, while also demonstrating why anyone with basic common sense could tell a massive coverup was underway.
Note: the report Johnson references can be read here.
That opening statement alone was sufficient to make the hearing’s intended point. However, I chose to watch the rest, in large part because I was curious how Senator Blumenthal (the lead voice defending the pharmaceutical industry at each of these hearings) would attempt to defend the indefensible.
His response was, on one hand, somewhat disappointing: at Johnson’s previous hearing, Blumenthal had briefly displayed genuine surprise at and interest in the plight of the vaccine injured, which was entirely absent this time. On the other hand, it was reassuring, as despite his zeal to defend the industry, all he could muster were a few arbitrary denials of Johnson’s findings and emotionally manipulative tangents bearing no relation to the actual evidence, demonstrating that against Johnson’s case, his position was indeed indefensible.
Note: I felt Blumenthal’s most memorable line was “The majority’s report cherry picks, emails, and misconstrues an internal debate between scientists who were actively looking for ways to detect side effect to support a predetermined and flawed thesis that COVID nineteen vaccines have done more harm than good. That’s not the scientific method to have a preconceived result and then frame the evidence to fit the outcome.” This is because the second sentence perfectly characterizes all the science conducted throughout COVID-19 that rationalized ways to prove the vaccines were safe and effective despite immense evidence to the contrary.
To further support his position, Blumenthal summoned a witness (representative of his political base), who testified to the trauma of nearly dying from COVID and then recovering from long COVID—which, while tragic (and likely preventable with non-standard COVID therapies), was again, entirely irrelevant to whether authorities covered up vaccine injuries.
As she detailed her journey and desperate desire to just be heard, I could not help but notice every single thing she described was identical to what the COVID vaccine injured routinely experience, who unlike her, have been gaslighted and forgotten by the medical system and often do not recover. Senator Johnson also immediately picked up on this too, and politely suggested she collaborate with the (far more common) victims of COVID vaccine injuries.
Note: every medication, policy or decision has a trade off between risks and benefits. Propaganda preys upon people’s inability to accurately compute this from limited data by emphasizing one side of the equation and downplaying the other (which for example is why many people who follow mainstream media sincerely believe “long COVID” is a much larger issue than COVID vaccine injuries). Likewise, in this hearing, vaccine proponents repeatedly used the often repeated line “vaccines save lives,” which while true, is immensely deceptive because it omits that in many cases vaccines also kill more people than they save or injure far more than they save.
Other facets of the hearing which jumped out to me included:
1. After vaccine proponents (once again) attempted to whitewash all criticisms of the vaccine by highlighting how incredibly well the COVID response was done in spite of the challenges faced at the time, one Senator pointing out that we need to stop repeating that fable and it is only by acknowledging that serious mistakes were also made that we can avoid making them again in the future (particularly because of how damaging they were to our children).
2. Repeatedly highlighting (as the earlier quotes show) that the senior FDA analyst who demonstrated vaccine harms were being covered up, Dr. Szarfman, was ostracized by her peers and shut down by her superiors. This in turn is very similar to the experience of Andrew Mosholder (a child psychiatrist and FDA safety officer) who in 2003 correctly determined data showed Paxil caused suicidality in children, after which his superiors blocked him from releasing the report (and then a year later, once it was leaked, focused on catching the leaker rather than acting on its findings).
3. There were numerous attempts to dodge FOIA requests which included the FDA simply stopping (potentially incriminating) internal data releases of COVID-19 vaccine adverse event data like Szarfman’s.
4. One witness highlighting that all the vaccine adverse reporting was designed to only report adverse events “no one cared about” such as injection soreness or a fever rather than serious and life changing adverse events people had.
5. Szarfman’s analysis showing 45 conditions were strongly linked to the COVID vaccines (with an upper and lower bound for their increased frequency). Assuming I interpreted the chart shown in the hearing correctly, when put in descending order by the lower bound (which makes a stronger case for causality), the conditions most conclusively linked to the COVID vaccines are as follows:
Strongest link: Product administered to patient of inappropriate age (Moderna), Acute myocardial infarction (Pfizer), Brain natriuretic peptide increased (Pfizer), Asymptomatic COVID-19 (Pfizer), Electrocardiogram ST segment elevation (Moderna), Blood pressure systolic (Pfizer), COVID-19 pneumonia, Acute myocardial infarction
Strong link: Brain natriuretic peptide increased, Ischaemic stroke, Drainage, Dementia, Pneumonia aspiration, Cardiac telemetry normal (which indicates it was being frequently checked due to heart concerns), Paraesthesia ear, Magnetic resonance imaging heart (which is done to evaluate for myocarditis)
Moderate link: Blood pressure systolic (all vaccines), Embolic stroke, Basal ganglia stroke, Cardiac assistance device user, Cardiac telemetry abnormal, Ejection fraction, Sinus rhythm, Hypertensive emergency
Weaker but Notable: Bell’s palsy, Sudden cardiac death, Pulmonary infarction, Bradykinesia, Cerebral artery occlusion, Diastolic dysfunction, Aortic stenosis, May-Thurner syndrome, Acute left ventricular failure, SARS-CoV-1 test, Cardiac failure chronic, Agonal rhythm, Cholecystitis acute, Product substitution, COVID-19 immunisation, Cardiac telemetry abnormal, AST/ALT ratio abnormal, Diaphragmatic spasm, Mastoid disorder, Percutaneous coronary intervention, Aortic aneurysm rupture, Thalamic infarction
That chart, in turn, was quite notable to me, as most of the conditions on it I’d previously concluded were probably linked to the COVID vaccines as I’d seen people develop them shortly after vaccination, and in many cases, would never have otherwise expected them to. That, in turn, highlights a recurring theme with the COVID vaccines—the harms were frequent enough that people like me with extremely limited datasets could accurately detect the signals of harm from the vaccines—so it’s hard to conceive they were “too rare” for health authorities who had access to infinitely larger pools of data to identify.
6. Much in the same way the early polio vaccines had major issues when their production was scaled up for the general population, the COVID vaccines did as well (because they switched from duplicating the mRNA with PCR to having bacteria mass synthesize it—resulting in dangerous synthetic bacterial DNA contaminating the vaccines). At this hearing, I learned there was supposed to be a comparison study between Pfizer’s old and new production methods of the vaccine (which like many other “required” tests was magically never done), and that later Pfizer’s vaccine (the dilutant) was changed again without being tested.
Finally, a few of the participants were quite blunt about how egregious this all was. Here for instance, Senator Hawley points out that the entire COVID vaccine affair was an unconscionable money grab the government pushed along while “All of the public health problems get offloaded onto other people, namely the American people…All of the costs get borne by the patients” (after which Johnson highlights how the government, from the start, also abandoned the vaccine injured).
Or to quote one witness, who after highlighting that the emergency use authorizations for the COVID vaccines was contingent upon extremely robust safety monitoring of them in the marketplace stated:
This isn’t a blind spot. The FDA was completely blind to adverse events, and the CDC wasn’t even looking. There was a savior in the ranks of the FDA who correctly identified the problem, appropriately worked with the inventor of EB data mining to create a solution, communicated the fix to everyone who would listen. The problem is no one listened. Luck was not on our side.
The CDC failed to look. The FDA failed to fix a broken system that the CDC touted as the gold standard. The HHS failed to protect us, especially after our freedom of choice was assaulted by the president threatening us all with our patience is wearing thin. FOIA evasion was well practiced and discovered, obviously, not through a FOIA. Simply put, during the largest pharmaceutical rollout in human history, pharmacovigilance did not exist.
That is the betrayal of our time, so vast that we cannot even count its casualties.
Masking Illness
One of my foundational beliefs has been that humanity has experienced a massive decline in vitality over the last 250 years as:
•Many of my mentors reports that from the start of their careers to the end, patients became sicker and less responsive to the therapies which had previously worked on them.
•In many cases, they found both colleagues and their own mentors shared these observations, and in a few cases, confirmed their mentors had received a similar response from the people who trained them.
•Corroborating this, I found numerous medical texts, beginning in the early 1800s which showed new degenerative diseases had begun emerging and detailed examples of treatments being used with a much higher degree of efficacy than when I observe in the present.
•Many data sets show chronic illness has continually increased as time has moved forward.
One of the insidious things about this decline is that since it is never talked about (rather medical training just focuses on the “dark ages of infectious disease vaccines miraculously vanquished”), it is very hard for medical practitioners to recognize this larger trend has occurred. As such, each new generation of medical practitioners becomes habituated to the current baseline of illness, and unless they live at a time when there is a massive and permanent spike in illness, rarely are cognizant of what has occurred.
Because of this, we’ve put a lot of thought into what is actually causing this massive decline in human vitality, have identified roughly 10 key agents, and believe one of the most impactful ones is widespread vaccination (e.g., the permanent spikes in illness typically coincide with the introduction of particularly dangerous vaccines, beginning with the original smallpox ones and most recently with the COVID-19 vaccines).
Doctoring Data
Over the years, I’ve heard many different definitions of intelligence, one of which is one’s aptitude for manipulating logical symbols towards a desired outcome. In turn, many facets of human society ultimately boil down to competing parties trying to rearrange what’s there to their advantage (e.g., rhetoric is essentially the skill of how you do that with your words to control people).
One of the particularly unfortunate things about science is that while it began as a tool those interested in seeking truth relied upon to further that goal, once this started producing results and social capital, the unscrupulous members of society seized upon science to promote their own agendas and no longer prioritized accuracy.
Because of this, a lot of “science,” much like rhetoric, is simply an exercise in rearranging the data obtained (or how the data is obtained) until it can be put into a configuration which credibly supports your message. As such, being able to interpret the scientific literature has become somewhat of an art, as you need a complex toolset to separate fact from fabricated fiction.
Vaccine Masking
Vaccines have a dose-dependent toxicity, so as you take more of them, you are more likely to develop chronic neurological or autoimmune diseases. Since the vaccine industry, like many others, is continually growth focused (and has very unique protections from the Federal government), there has been a continual trend to give people more and more vaccines.
This has reciprocally led to a sustained increase in chronic illness (sometimes beginning immediately following vaccination) which has become harder and harder to cover up as it gets increasingly frequent. To address this, the vaccine industry has used increasingly aggressive methods to censor those injuries, so people do not connect them to vaccinations, and for those who nonetheless do, they will be widely ridiculed by those around them. This for example is why:
•Medical journals used to publish severe vaccine injury case reports (many of which are summarized here) but now never will.
•Television stations used to regularly air programs on individuals having their lives ruined by vaccines (56 of which I compiled here), but now never do due to Clinton-era regulatory changes allowing pharmaceutical advertising to buy out the media (which RFK is presently trying to reverse).
•So much work has gone into making it socially acceptable to demonize anyone who questions vaccines and hence end any question on the subject.
•Tech platforms (until recently) aggressively censored content critical of vaccination.
Likewise, a variety of absurd epistemological frameworks have been erected to sanctify the notion vaccines are completely safe and cannot harm you.
Aaron Siri, for example, in his book about the religion of vaccines (Vaccines Amen) highlighted that all of vaccine science is predicated on the notion that vaccines are completely safe and effective, so any evidence, regardless of how weak it is that supports this is viewed as true, while any evidence which refutes it, regardless of how robust it is, is typically disregarded.
This in turn, has allowed a rather remarkable standard to be accepted within vaccine clinical trials where rather than vaccines being tested against placebos, they are tested against other vaccines, and only deemed to be dangerous if their rate of harm is significantly higher than the other vaccine. Because of this, it is possible to “chain” vaccine studies together, where increasingly toxic vaccines are deemed “safe” (as they are only somewhat more harmful than the one that immediately preceded them and the newer vaccine was tested against).
Note: the justification for this experimental design is that “vaccines are so safe and effective and lifesaving that it is unethical to deny children in trials vaccines, so rather than placebo, they should get the previous “safe” vaccine.” Beyond that being absurd (as it’s far more unethical to inject every child with an untested vaccine), in many cases, the vaccine “placebo” is a completely different vaccine (which entirely defeats the logic of that argument).
One of the most insidious things about this framework is that it effectively hides the continual increase in chronic illness, as it occurs in tandem with increasing vaccine side effects being viewed as “normal” and not elevated from baseline (whereas they clearly are were the vaccines to be compared to an actual placebo).
Note: as you might expect, most of the basic studies necessary to determine vaccine safety, especially multiple at a time, have never been done because they are “unethical.” Conversely, when the studies that can be done are nonetheless done (retrospective or observational), they all show vaccines cause a massive increase in illness (typically a 2.5 to 9 fold increase), but are always dismissed for not having placebos (which can never “ethically” be done).
Interestingly, a very similar safeguard is put into Federal vaccine safety monitoring.
Specifically, the CDC uses the Proportional Reporting Ratio (PRR) to help identify potential safety signals in VAERS data (which only exists because a law forced the government to have a public reporting system available). The PRR compares the proportion of a specific adverse event reported for a given vaccine against the proportion of that same event reported across all other vaccines in the database to determine if that side effect is disproportionately higher in the vaccine in question. The FDA likewise utilizes a similar disproportionality analysis which uses additional statistical measures that reject certain links the PRR would establish.
While this approach can detect fairly unique side effects linked to a specific vaccine, it has major blind spots:
Due to the top half of the formula, it struggles to flag individual side effects for vaccines that cause a high overall rate of adverse events. If nearly every side effect is elevated for that vaccine, no single one stands out proportionally compared to the vaccine’s own other reported events.
Due to the bottom half of the formula, it cannot easily detect side effects that occur across many different vaccines (e.g., certain neurological, autoimmune, or cardiac events), because those events are also elevated in the comparator group, making the vaccine in question look less unusual.
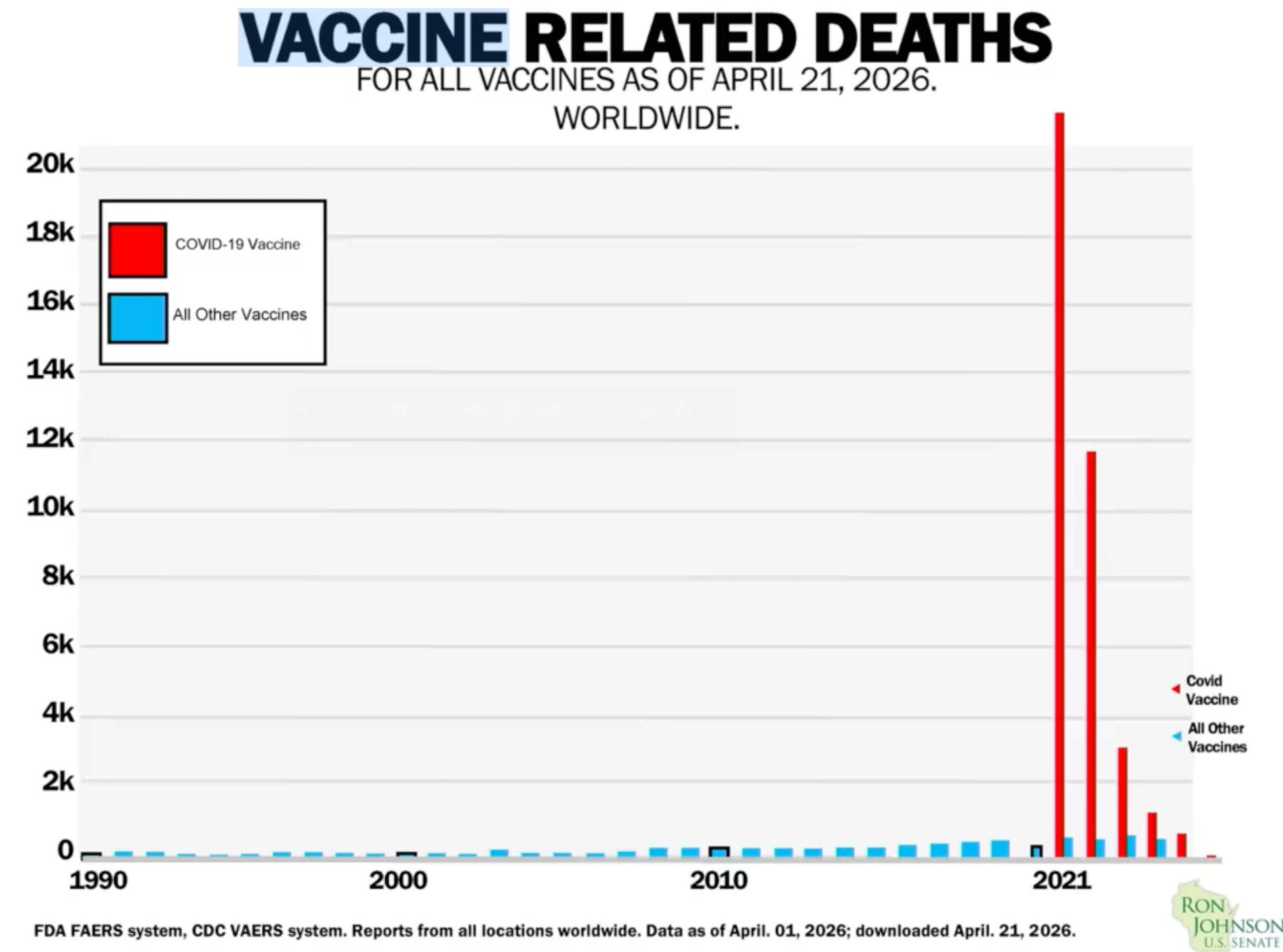
Additionally (due to the bottom half) when two or more similar vaccines enter the market at the same time and both have much higher adverse event rates than older vaccines, the PRR becomes heavily masked as the “all other vaccines” baseline gets flooded by reports from the other new vaccine(s), so neither one stands out as disproportionate.
When I learned about the PRR, I immediately noticed how well-engineered it was to conceal the ever increasing harm from vaccination, as harm would always be assessed against a previous (already increased baseline) and increases large enough to trigger a signal were hard enough to reach they would rarely if ever happen. More remarkably, this system also provided the magic solution for an incredibly toxic vaccine being released onto the market, provided there were at least two different ones released simultaneously.
As it happened, seven weeks after the first COVID-19 vaccines received Emergency Use Authorization, and as VAERS began receiving a surge of adverse event reports, the CDC issued its VAERS Standard Operating Procedures for COVID-19. In that document, the agency formally designated the Proportional Reporting Ratio (PRR) as one of its primary tools for routine safety signal detection, stating it would perform PRR data mining on a weekly basis or as needed (something I am almost certain was done as it was the only way to hide the massive signal of vaccine injury).
Note: despite this, the CDC eventually stopped doing even this to (while making numerous false statements on what it had done) and ultimately deferred to the analysis to the FDA’s “more robust system.”
The net result of this approach hence was that things like this “were not signals” because they were being compared to other massively elevated baselines.
Szarfman in turn came up with a fairly obvious solution to this problem: rather than compare an mRNA vaccine to all other vaccines plus the other mRNA vaccine, you don’t include the other mRNA vaccine in the comparison (red vs. blue rather than red vs red plus blue). However, despite being incredibly obvious, since that revealed critical issues with the COVID vaccine the existing approach masked, it hence was not acceptable (and we only even learned about it thanks to Johnson’s lengthy investigation).
One in a Million
Since vaccine injuries are frequent and unavoidable, the medical industry’s solution has been to reframe them as “very rare” so people are not alarmed by injuries they run into, and at some point settled on the phrase “that injury is one in a million”(which may have originated from the smallpox vaccine’s encephalitis rate — somewhere between 7 and 1,444 per million vaccinated), alongside assurances robust support is in place for the one in a million who are injured.
Because of that, a schizophrenic dichotomy exists with vaccine injuries where:
1. Common but relatively inconsequential ones are publicized (e.g., injection site pain or being ill for a few days), after which concerns about them are dismissed by highlighting the inconsequential nature of the injury.
2. The severe and life altering ones which affect large numbers of people are relentlessly denied.
3. The extraordinarily rare ones which are unique to specific vaccines are emphasized, and in some cases results in the vaccine being pulled if an alternative is available (e.g., this happened with one rotavirus vaccine).
This hence makes it possible to create the illusion of robust vaccine safety, as people will assume that if regulators are strict enough to go after extraordinarily rare things, they will definitely go after common things (further reinforced by the focus on inconsequential reactions). That, I believe is also why:
•The system used in VAERS to detect injuries (PRR) can only detect unique and rare injuries, whereas the common injuries everyone cares about seen across vaccination (category 2) are essentially never are flagged by it.
•Monitoring systems like V-safe which were designed to detect category 2 injuries were discarded by the FDA and CDC once they realized it was detecting large numbers of category 2 injuries.
•The NIH was initially very interested in providing support to individuals like Brianne Dressen who received severe neurological injuries from the vaccines (and even provided a costly treatment that somewhat worked), but once they realized her injury wasn’t “rare,” pivoted to ghosting her and blocking the publication of the research studies she participated in (as a very rare side effect they could treat would increase confidence in vaccination, whereas acknowledging a common one would decrease confidence and exceed their budget to treat every instance of).
•The FDA made a big deal of temporarily pausing the J&J vaccine due to a few cases of a very rare blood clot (cerebral venous sinuses thrombosis), while ignoring the far more common clotting risk of the mRNA vaccines.

Conclusion
Over the eons, many have concluded one of the greatest mistakes humans make is believing they can hijack and dominate natural processes rather than recognize their influence over them will be temporary at best and create significant strain in the process (e.g., most pharmaceutical drugs work by artificially shifting the enzymatic baselines within the body, something that commonly provokes resistance to the drugs and increasing side effects as the body deviates further and further from its baseline).
However, a major reason why I believe in the “law of equilibrium” is because in instances where it appears to not be being followed (e.g., during a positive feedback loop, or when expected negative feedback fails to materialize) on a broader scale it still is and the expected changes still occur.
Because of this, in instances where it appears people have been able to successfully suppress a natural equilibrium, a broader feedback loop will eventually take over. For example, in the case of vaccines, for 250 years, we have seen a continually escalating cycle of more and more powerful methods being used to push vaccines upon an increasingly resistant public (which has been incredibly depressing to witness as I’ve lost count of how many people I know whose lives were ruined by vaccines and then gaslit by everyone around them as the majority of people could not conceive these injuries could ever occur in the first place).
However, while propaganda has an incredible ability to sweep things under the rug, it has limits, and because of just how many people were injured by the COVID vaccines (e.g., polls consistently show 12-20% of those vaccinated were injured; often seriously), it has become impossible to cover up (e.g., 49–55% now believe the vaccines caused significant unexplained deaths). Furthermore, a much broader loss of trust has occurred in vaccines, the medical system, and health authorities that dwarfs anything else in the history of medicine (all of which I detailed here). Consider for example how scathing Hawley’s language was towards the pharmaceutical industry; we never heard statements like these before and they are only being said (before the midterms) because a large portion of the electorate supports them. The tide, at long last, appears to be turning—not because the truth changed, but because it finally became too large to hide.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.
"Vaccine hesitancy" is such a BS term. "Vaccine NOPE" would be the correct term. Because once you are jabbed with anything you can't change your mind. Speaking just for myself, there is literally no one who could convince me to get jabbed for anything now. Why would I trust anyone on that? Can't be undone. As much as I admire all the doctors who are saying nope, I would not get jabbed, now, for anything on their say so. That chicken has flown the coop. Probably has the flu.
Nice to see Sen. Johnson taking action again. Let’s hope more comes of it this time.