Just How Far Will the FDA Go To Protect A Bad Drug?
What the tragic lessons of the SSRI antidepressants can teach us about the COVID-19 vaccines

Story at a Glance:
•The SSRI antidepressants are some of the most harmful medications on the market, but also some of the most profitable.
•Since their discovery, a deluge of data has shown that they are incredibly unsafe, and as one whistleblower testified, overt bribery was needed for the first SSRI, Prozac, to be approved.
•While the FDA initially tried to stop Prozac, once Bush came to power (as his family was in bed with Prozac’s manufacturer), the FDA reversed course.
•Since that time, the FDA has gone to extremely lengths to cover up the harms of antidepressants. Much of what the FDA did with the SSRIs was identical to what it’s done with the COVID vaccines and I believe learning what happened in the past is highly instructive for understanding what the FDA is doing now and how to stop it.
Every now and then, a highly profitable pharmaceutical will come along that everyone also knows is quite dangerous. Remarkably, rather than this stopping the product, it will often be pushed to market and the profits it generates will be used to ensure any objections to its safety get ignored and blown to the wayside.
One of my goals with this Substack has hence been to review the scandalous history of some of the most dangerous pharmaceuticals on the market. This was done both to help those being harmed by them (e.g., consider the story of the statins and the story of the NSAIDs) and to illustrate that the horrendous malfeasance we’ve observed from the FDA throughout COVID-19 is in fact has been it’s standard operating procedure.
For example, I recently covered the story of Merck’s Vioxx, an unsafe and unneeded painkiller which was kept on the market until outside investigators proved it was causing heart attacks and strokes (estimated to have killed 120,000 people by the time Vioxx was withdrawn), something Merck was fully aware of from the start. Vioxx resulted in a wave of lawsuits which cost Merck billions of dollars but never resulted in criminal charges against any of the executives responsible for those deaths (rather they got bonuses).
Immediately after the Vioxx lawsuits, Merck brought the HPV vaccine Gardasil to market, fully aware that it had minimal value to those vaccinated (in fact it increased the risk of cancer by 44.6% in those who already had the target HPV-16 or 18 infection—something which like COVID-19 is never tested for prior to vaccination). More importantly, Gardasil had an extraordinarily high rate of adverse reactions.
Note: in its trial, over 50% of the girls were observed to have developed “new medical conditions,” 2.3% of which Merck admitted were autoimmune in nature (although the actual figure was likely much higher).
Once Gardasil hit the market, the CDC and FDA were deluged with a wave of injuries being reported to them. However, rather than listen to these warnings, they doubled down on their claim the vaccine was “safe and effective,” did everything they could to bury those injuries, and ardently worked with Merck to sell the vaccine to as many people as possible.
However, as bad as those stories are, I believe what happened with the Selective Serotonin Reuptake Inhibitor (SSRI) antidepressants is even worse. Since the SSRI saga provides the clearest case study I know of into the gross malfeasance of the FDA, this article will review it in the hope we can better understand the agency’s behavior with the COVID vaccines and just how far it will go to protect the pharmaceutical industry.
Note: Psychiatric medications are one of the most profitable drug franchises, making approximately 40 billion dollars a year—a figure that is expected to significantly increase in the years to come.
The Harms of SSRIs
When integrative physicians are asked to name what they consider to be the five most dangerous mass prescribed drugs in America, SSRIs (and SNRIs) almost always end up on the list, something I believe is due to their mechanism of action (and adverse event profile) having many overlaps with an illegal stimulant like cocaine.
In the first and second parts of this series, I attempted to detail those harms which included:
•Causing violent psychotic behavior which frequently led to suicide, and less frequently to homicide.
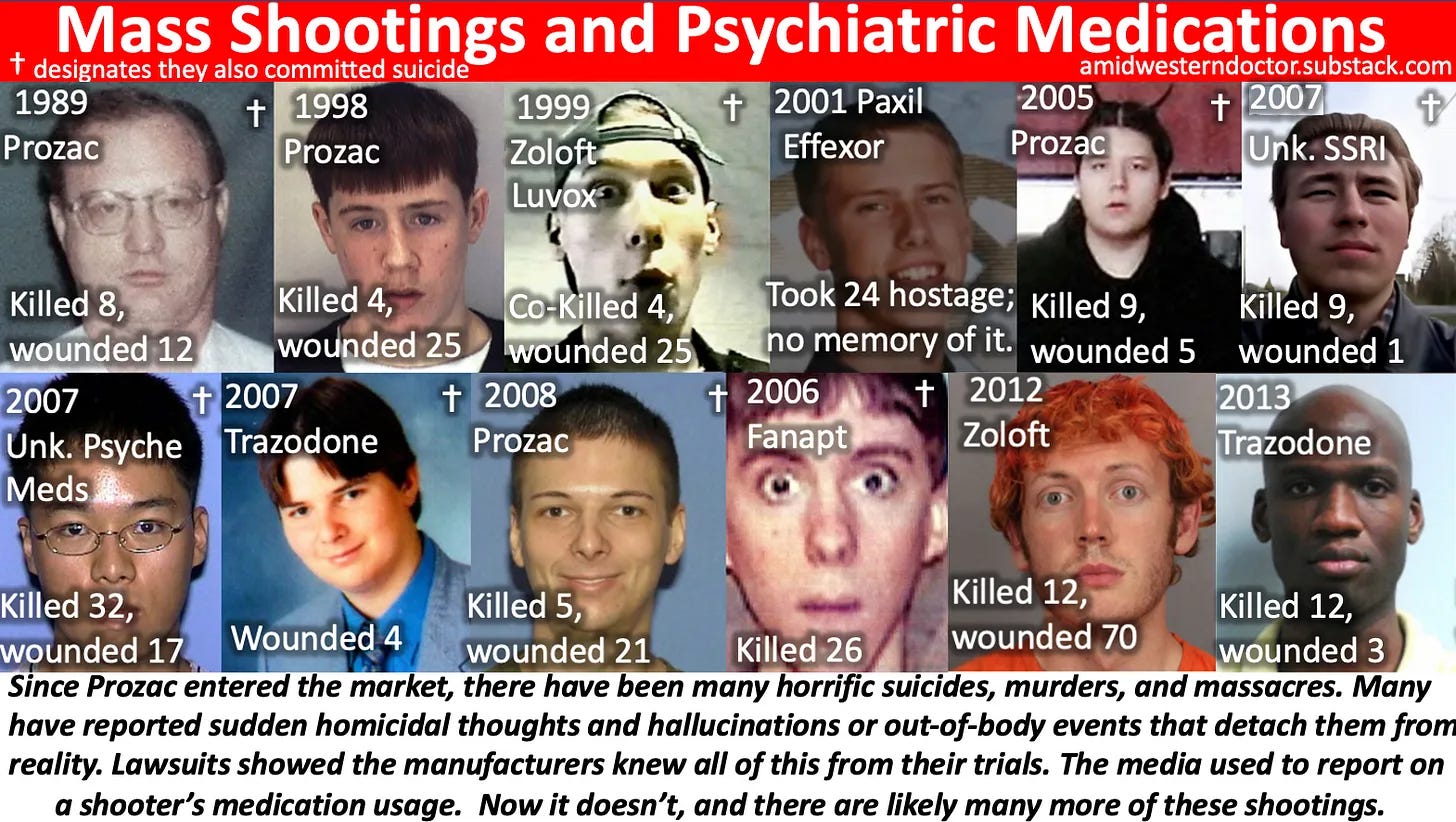
To illustrate: a peer-reviewed Swedish study looked at information on over 850,000 patients prescribed SSRIs within a national database and compared the rates of violent crimes committed by these individuals when they were and were not taking an SSRI over a 3 year period. This study found that SSRIs increased the rate of violent crimes committed by 43% in those between the ages of 15 and 24 receiving the drugs.
Note: I initially focused on psychotic SSRI violence because it is a common but undiscussed thread in mass shootings (and other grisly murders which shocked their community). However, I believe the SSRI suicides (as they are far more common) are an even bigger issue. Consider for instance that one study found 10% of mentally healthy volunteers on an SSRI became suicidal, while a much larger survey of SSRI users found 39% had experienced suicidal ideation while on the drugs. Additionally, as the previously mentioned Swedish study shows, SSRIs have been repeatedly shown to significantly increase the incidence of hostile (but not yet psychotic) behavior.
•Causing 7.7% of the users each year to develop bipolar disorder (ultimately affecting between 20-40% of SSRI users). For many, bipolar disorder is a permanently debilitating disorder which significantly impacts one’s quality of life.
•Causing over half of the users to no longer feel like themselves and in many cases as though they were losing their own minds.
•Emotionally anesthetizing 60% of the users. This numbness frequently results in individuals losing the will to leave a toxic relationship or work situation (often for years if not decades), to stop emotionally reacting to things you should react to (e.g., someone being mean to you or violating your boundaries), and to no longer experience the joy or vibrancy of life.
•Causing sexual dysfunction in the majority of the users (59% in this study, 62% in this study) which is often extremely impactful to the patient’s life (e.g., 40% in this study found the side effect intolerable).
Note: keep in mind that sexual dysfunction is one of the fastest ways to make someone depressed.
•Increasing the risk of life threatening birth defects by 2-6 times (e.g., taking a single SSRI increases the likelihood of the newborn having a septal defects from 0.5% to 0.9%, while taking two increases it to 2.1%).
•Causing severe withdrawal symptoms (e.g., frequent electrical zaps through the brain) in 56% of those who discontinue the drugs, with most (46% of discontinuers) experiencing severe withdrawals. Very few people appreciate just how difficult it can be to get off an SSRI (even after only a brief course of the drugs), or that there is absolutely no support within the conventional medical field for patients wishing to get off the drugs. This is particularly tragic because many of the SSRI suicides and murders are preceded by someone having their SSRI dose changed (e.g., increased, decreased or changed to a different medication).
Note: Since I was repeatedly asked to do so, I attempted to put together my suggestions on how to withdraw from SSRIs, and I must emphasize it is truly unfair just how addictive these drugs can be.
Sadly in addition to those common side effects, patients also experience a variety of debilitating side effects from the SSRIs such as palpitations, anxiety, and insomnia. Worse still, it is fairly feasible to identify who will have a good or bad response to SSRIs (e.g., from their genetics) but physicians are never taught how to do this as it would understandably reduce SSRI sales if they were only given to those who will benefit from them.
Note: similarly much (but not all) of the harm which occurs from vaccines (especially in children) could be avoided if doctors were taught to recognize the initial adverse reactions children experience and pause giving those children additional vaccines. Likewise, if the vaccines were spaced out (rather than all being given together during the critical developmental period of a child) or the most dangerous ones (e.g., Gardasil or COVID-19) were taken off the market, the harm also would significantly decrease
However none of that has been done since it would be equivalent to an admission vaccines are not “100% safe and effective” and hence significantly reduce vaccine sales. Consider for instance that the government was actually mandated by the 1986 National Childhood Vaccine Injury Act (which gave legal immunity to the vaccine manufacturers) to study the safety of the existing vaccines so that safer ones could be developed, but it has nonetheless refused to do so ever since.
Regulatory Failure
When you read through the previous section, the first thing that should catch your attention is how just high the percentage of adverse reactions were (e.g., many affected approximately half of those taking the drugs). This in turn highlights just how badly the FDA can fail to do its job and “detect” patently obvious side effects which were seen throughout each SSRI’s clinical trials and then throughout America once the drugs entered the market.
To explain this, I put forth the argument that a drug’s approval is not based on its risks versus its benefits, but rather its risks, its benefits, and its potential profitability (e.g., consider how large the potential antidepressant market is)
This for example is why fairly safe and effective treatments (e.g., hydroxychloroquine or ivermectin) were relentlessly attacked as unsafe and ineffective by the American medical establishment. Similarly, it’s why incredibly dangerous and unsafe ones that were also incredibly profitable were pushed on America throughout the pandemic despite widespread public opposition to their adoption and study after study showing the official pandemic policy was causing more harm than good.
Likewise, because people are creatures of habit, you can be relatively assured that if something was used in the past which “worked,” you will see it done again and again. My familiarity in turn with the dirty deeds by used by the pharmaceutical industry with their worst products (e.g., the SSRIs or Gardasil) in turn made me immediately spot those same tactics being used to doctor the COVID vaccine trials, trick the public into buying them, and cover up the deluge of evidence they were harming people.
As you review the SSRI saga, it is important to remember that much of this was only discovered through lawsuits against the manufacturers and Congressional investigations (as the industry has successfully argued their raw data is proprietary information and hence cannot be disclosed to the public—which in turn requires us to “trust” their presentation of it).
Since that time, the pharmaceutical industry has gained much greater control over both the media and government and has legally been granted almost complete immunity from being sued for an unsafe and ineffective vaccine so similar documents are highly unlikely to be revealed through the discovery process.
Note: In an 1989 lawsuit which followed a man shooting eight people dead, wounding another 12 and killed himself one month after he started fluoxetine, Lilly “won” a jury verdict and claimed it was “proven in a court of law ... that Prozac is safe and effective.” The trial judge however forced Lilly to admit that it had made a secret settlement with the plaintiffs during the trial and, outraged, the judge changed the verdict in Lilly’s favor to one of “dismissed as settled with prejudice.”
As part of this deal, Lilly illegally regained the incriminating documents it had been forced to disclose, preventing them from being used in other in other lawsuits. Sadly, in addition to burying incriminating documents within the courts, both the FDA and the EMA (Europe’s FDA) have repeatedly managed to “lose” documents in their possession which incriminated the SSRIs.
Doctoring Trials
While we hold randomized controlled trials in high regard, in truth there are a variety of ways they can be doctored to arrive at the results the sponsor wants, regardless of how ineffective or unsafe they are. For example, the public was told over and over that the COVID vaccines were safe, effective, and would end the pandemic despite:
•The Pfizer trial showing that at best you needed to vaccine 119 people to prevent a single minor case of COVID (e.g., a sore throat plus a positive test), 2711 to prevent a major case of COVID (major being undefined), well over 21,720 to prevent a single death and that the vaccine’s ability to prevent transmission had never been tested.
Note: once the vaccine hit the market, COVID rapidly evolved resistance to the vaccine, so in real life the actual figures were even worse.
•That many of the Pfizer trial participants experienced symptomatic reactions from the vaccine which were as bad or worse than a COVID infection (e.g., 59% experienced fatigue after Pfizer's vaccine, whereas around 10-15% experience fatigue after a typical influenza vaccine).
•The Pfizer trial 6 month report showing that more people died (and were injured) who got the drug than who got the placebo.
•Numerous whistleblowers coming forward and testifying they suffered a severe reaction to the COVID-19 vaccine which never made it into the final trial report, one of whom directly notified the senior management at the FDA over what was occurring and another, who (being a lawyer) filed a formal governmental inquiry against the lead author of Pfizer’s vaccine trial.
•A manager of a Pfizer trial site providing documented evidence to the FDA that their site was flagrantly violating established research protocols (e.g., not having the trial be blinded, failing to test those who received the vaccine and developed COVID like symptoms for COVID and underreporting vaccine injuries) .
Note: the FDA refusing to listen to reports of serious issues with its drug (and in turn denying they even existed) is likewise nothing new (e.g., I recently provided footage of them doing it the 1980s with the now withdrawn DTwP vaccine). Similar, consider Kim Witczak’s experience:
As the head of FDA division Dr Bob Temple and Dr Tom Laughren told us in a private meeting with them, David Healy and another family, my husband was just an “anecdote“ because it didn’t happen in a double blinded placebo controlled trial [even though lawsuits later showed it did]. I kept telling them to go investigate how my husband went from not sleeping (reason for prescription) to head outside body looking in to hanging in 5 weeks with no depression or history of depression or mental health issues. It was first glimpse that FDA has no desire to investigate and also learned the same people responsible for approving drugs were also responsible for monitoring safety. Obviously, it is out of control with covid vaccines
Given all the serious issues which had been detected in their trial, let’s review how Pfizer described their vaccine in their much heralded December 2020 NEJM paper:
The safety profile of BNT162b2 was characterized by short-term, mild-to-moderate pain at the injection site, fatigue, and headache. The incidence of serious adverse events was low and was similar in the vaccine and placebo groups.
A two-dose regimen of BNT162b2 conferred 95% protection against Covid-19 in persons 16 years of age or older. Safety over a median of 2 months was similar to that of other viral vaccines.
At the time this paper was released, it was greeted with an almost religious jubilation by the medical field, and before long I realized it was an exercise in futility to explain to many of my colleagues why the trial’s conclusion was not at all supported by the data within it. As you all know, that jubilation quickly spread through the country and before long gave rise to the highly unethical vaccination mandates.
However, despite a litany of evidence emerging which showed that Pfizer’s paper had serious shortcomings which should not have passed peer review (e.g., documented fraud by the lead author) NEJM has not issued a retraction or correction. This is identical to what NEJM did with its pivotal Gardasil paper, and what NEJM did with its Vioxx paper until a wave a lawsuits mounted against Vioxx (at which point NEJM issued a “statement of concern”).
Sadly, we were warned in 2004 by NEJM’s editor-in-chief that the medical journals (e.g., the NEJM) are corrupt and cannot be trusted. Had she been listened to, there might have been a bit more skepticism towards Pfizer’s NEJM trial.
Note: for those interested, some of the best resources I’ve come across for the tricks drug companies commonly use to create the illusion a bad drug is “safe and effective” are Doctoring Data (by Malcolm Kendrick), Deadly Medicines and Organized Crime (by Peter Gøtzche), The Truth About Drug Companies (by Marcia Angel) and Bad Pharma (Ben Goldacre). Of these doctors, Goldacre is the most orthodox one, so I find his book on pharmaceutical corruption, while not as good as the previous, is often more effective for persuading more skeptical parties.
The SSRI Trials
The less concrete a pharmaceutical’s benefit is (e.g., preventing minor flu like symptoms occurring in parallel to selectively applied [and almost always positive] COVID-19 PCR tests), the easier it is to alter the trials parameters to create the illusion that a minor change is actually a big deal (e.g., Pfizer’s 0.8% reduction in the likelihood of having a minor case of COVID).
Since “depression” is a highly subjective metric, a variety of methods were concocted to create the illusion the drugs “helped,” improve depression. This for example was done by using scales which “quantified” the effects of the drugs for anxiety and depression rather than something which directly correlated to either. To illustrate, in a meta-analysis conducted by GSK, suicide-related events occurred more often (3.86 times) on Paxil than on placebo in children and adolescents, whereas suicide items on rating scales the trials used like Hamilton’s didn’t show this difference. Likewise, a meta-analysis carried out by the FDA in children and adolescents found suicide items on depression scales “showed” SSRIs decreased the risk of suicide by 8% whereas raw company data showed the risk was increased by 95%.
Note: The subjectivity of what constitutes depression has resulted in a significant discrepancy between the benefits psychiatrists perceive from their medications, and what their patients experience. This 1982 study of the effect of blood pressure medications for instance excellently illustrates the tendency of doctors to overestimate the benefits of their drugs:
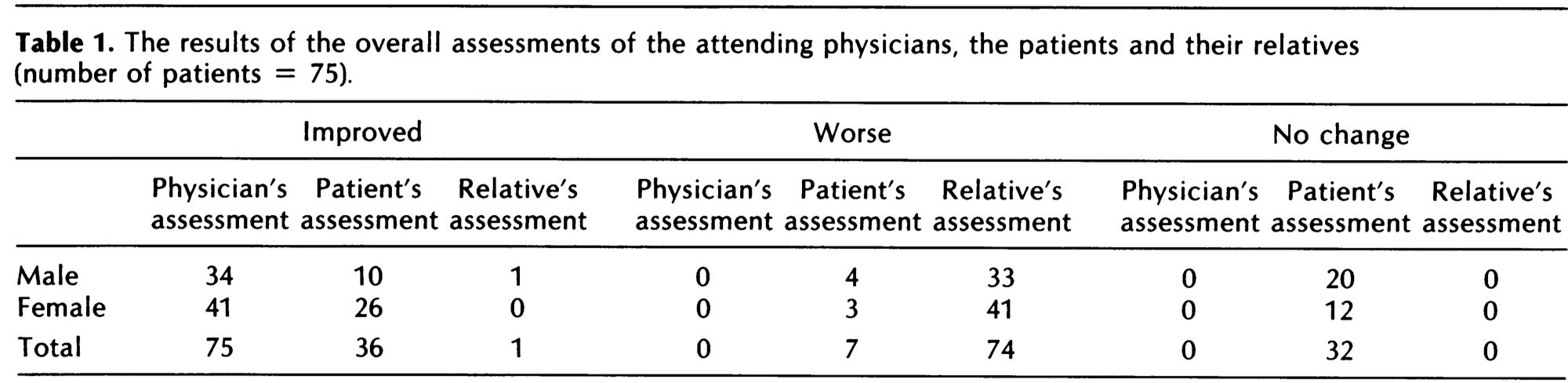
Likewise in the SSRI trials, it has frequently been observed that psychiatrists tend to document a much greater improvement for their patients than what the patients themselves reported. For example in 8 trials, which included 1576 children and adolescents, trial site psychiatrists reported an overall improvement (effect size 0.25), whereas the patients themselves did not (effect size 0.05), results which were also found in a Cochrane review of newer antidepressants in children and adolescents (effect sizes of 0.29 vs. 0.06). Given that “mental health” is entirely in the mind of the patient, it is insidious that psychiatrists can be the arbiters of the benefits of these drugs, and we routinely see countless cases where psychiatrists exercise their power to forcefully medicate patients.
Beyond the fact that many of the common SSRI side effects mentioned previously (e.g., sexual dysfunction) would make one “depressed,” in my eyes, one of the best proofs of the absurdity of the SSRIs was that high rate of people who voluntarily stopped taking SSRIs (e.g., between 44%-56% of those in surveys of thousands of patients on SSRIs, and likewise similar results were observed in the clinical trials). Given that so many patients, against the advice of their doctor were willing to stop using the pills that were supposed to make them feel “good,” this suggests the pills failed to accomplish their goal (i.e., instead it made them feel bad).
Note: likewise, a survey of 500 patients found 81.5% were unsure if their anti-depressants were necessary.
Conversely, the industry effectively concealed the wide range of side effects which came up in the trials through the following methods:
•They intentionally harmed the placebo group so that the “drug” group would look better in comparison. This was accomplished by recruiting people into the trials who were already on SSRIs, and then withdrawing those in the placebo from their drugs causing them to enter devastating withdrawals (the side effects of which were detailed in the previous article).
Note: Sadly this abhorrent tactic is not unique to the SSRIs. For example, with Gardasil, those in the placebo group were given the most toxic component of the vaccine (its extremely potent aluminum adjuvant), which resulted in similar amounts of severe injuries (e.g., the autoimmune disorders) developing in the “placebo” group, which in turn was used to argue Gardasil’s side effects were unrelated to the vaccine.
•They gave the patients who suffered “activating” side effects (e.g., aggression, bipolar disorder, violent behavior, or anxiety) from the drugs benzodiazepines to “treat” those side effects (which of course were not disclosed in the trials since the patients did not display those behaviors when the trial concluded).
Note: by one estimate 84% of the SSRI trials used benzodiazepines as part of their protocol.
•They used scales to evaluate adverse effects of the drugs which did not register the common side effects of the drugs, which in turn led to many not being detected.
Note: this is similar to how Merck chose to label the deluge of Gardasil injuries as “new medical conditions” and how many who participated in the COVID-19 vaccine trials were not given a way to report their injury, even when they repeatedly tried to do so (hence leading to there being “no data” the injury could occur). Likewise, in the system the CDC made to monitor adverse reactions to the COVID-19 vaccine, participants were not given the option to enter many of the more severe COVID-19 vaccine side effects.
•They recruited the healthiest members of society (e.g., those less likely to commit suicide) to the trials, and in three-quarters of the SSRI trials they had an initial 1-2 week period where those who had a bad reaction to the drug could be detected and excluded from continuing in the trial. Conversely, many of those who receive SSRIs in real life already have a mental illness, and those who have a bad reaction to the SSRI are almost never withdrawn from it by the prescribing doctor (rather the dose is often raised).
Note: this is a longstanding issue in clinical trials (e.g., we rarely test drugs on the elderly—who are typically the most likely to suffer adverse reactions to them, but once the drugs go to the market, those are the groups they are most frequently pushed upon). In the COVID-19 vaccine trials, in addition to relatively few of the elderly being tested (who in turn were frequently found to have the highest rate of death from the COVID-19 vaccines), those with pre-existing autoimmune disorders were also not tested. This was unfortunate because one of the most common severe side effects of the COVID-19 vaccines was an exacerbation of a pre-existing autoimmune disorder (which happens to between 1 in 3 to 1 in 5 of those patients)—something many suspected would be a problem with the vaccine due to its design, but something that conveniently was never assessed prior to it being given to humans.
•Individuals were carefully monitored throughout the trials to ensure they do not miss a dose (to avoid a withdrawal) and often taken out of the trial before severe side effects could emerge, something which again does not occur in real life. Likewise, they received an attentive circle of social support (which is very helpful for mental illness but again often does not occur in real life).
•They often failed to publicly report severe adverse events (a commonly used excuse is that the investigators decided the events were “unrelated” to the drug). For example, in a pivotal Paxil study, after three subjects were removed from the trial because they attempted suicide, the lead author failed to report this and instead stated that they were terminated from the study because of “non-compliance.”
Note: that author also received hundreds of thousands of dollars from the pharmaceutical industry each year which he failed to disclose (along with his department receiving $50 million in “research” funding). Additionally, a social worker found evidence he outright fabricated some of the adolescents who were allegedly enrolled in that trial (as he was paid $25,000 for each child he “recruited”). Despite all of this, he has received no significant repercussions for his actions.
Likewise, a 1985 in-house analysis of placebo-controlled trials for Prozac found 12 suicide attempts on Prozac versus one each on a placebo and a tricyclic antidepressant, but after the blind was broken, six of the suicide attempts were “removed” from the dataset. Similarly, the FDA’s expert on safety matters, David Graham, noted that fewer than 10-20% of fatal effects were reported for Prozac, but the data nevertheless showed relatively more suicidality among patients on Prozac than among those on tricyclic antidepressants or placebo. Sadly, all of these warning were ignored by the FDA leadership.
Similarly, consider the early 2000s trials where Lilly unsuccessfully tried to promote the use of Cymbalta for urinary incontinence. In these, it was discovered that there had been had 41 deaths and 13 suicides in the trial participants Lilly concealed from the public, including a notorious 2004 case where a healthy 19-year-old student who had joined the trial to help pay her college tuition hanged herself in a laboratory run by Lilly. It was then discovered the FDA had no record of her suicide or that of at least 4 other test subjects and refused to release the data (e.g. deaths it had received) under the logic it would be “commercially unfair” to Lilly if it did so.
One of the best proofs SSRI deaths are deliberately removed from trials came from a 2005 meta-analysis conducted by independent researchers of the published trials. It included 87,650 patients and all ages and found 2.28 times the suicide attempts on drug than on placebo and that many suicide attempts were missing from the trials (e.g., some of the investigators who were queried responded that there were suicide attempts they had not reported in their trials, while others shared that they didn’t even look for them).
Note: SSRI suicides are almost always attributed to “pre-existing” depression, which is then used to argue that those suicides actually meant that more SSRIs rather than fewer SSRIs should be given out. Yet, in a detailed review on the subject of depression and suicide, only 26% of those who commit suicide had been diagnosed with depression before the suicide. This is analogous to many COVID vaccine injuries being blamed on catching the virus itself (e.g., many injuries are attributed to long COVID).
Sadly, one of the most common causes of vaccine death is the individual developing a fatal case of COVID-19 (this has been shown within the VAERS data and I personally know of many cases where this happened). Likewise, I know of multiple cases where an individual had an asymptomatic or minor infection at the time of vaccination that then rapidly became severe or fatal. Sadly, rather than consider the vaccine’s culpability, these cases are used to argue the individual needed to have been vaccinated earlier, much in the same way SSRI suicides are attributed to insufficient “treatment” of those patients.
•When the side effects were reported, much like the previously mentioned “non-compliance” those effects (with the FDA’s consent) were reclassified to innocuous and misleading terms (which were often only learned after lawsuits forced the disclosure of those trials). For example:
—Suicides were typically coded as “overdoses.”
—Suicidal ideation or attempted suicide was coded as “depression” or “emotional lability.”
—Akathisia (the violent restlessness where one feels as though they want to jump out of their skin and which typically proceeds murder or suicide) was coded as “nervousness,” “agitation” or “agitated depression.”
—Abnormal thoughts (one of the most common SSRI side effects) was coded as “abnormal dreams.”
— Other attempted (and frequently completed) suicides that were preceded by hallucinations were simply coded as “miscellaneous effects” (not unlike what happened with Gardasil’s most concerning injuries). Remarkably, as shown within Lilly’s own memos, even their own researchers (in Germany) were uncomfortable doing this and only did so because they Lilly’s management ordered them to.
Note: Many of the trial participants testified that they suffered a severe injury from the COVID-19 vaccines which did not make it into the final report despite their best attempts to do so (e.g., providing the medical documentation showing that they did indeed have the condition or petitioning the FDA for it to be awknowledged). Maddie De Garay for example is permanently disabled (she can no longer walk alongside a variety of other debilitating symptoms) and her reaction was coded as “functional abdominal pain,” Olivia developed a malignant and unusual cancer which was coded as “moderate lymphadenopathy” (swollen lymph nodes), and Augusto Roulex almost died from a pericardial effusion, which was coded by the lead authors of Pfizer’s NEJM trial as COVID-19 (despite Augusto testing negative for COVID-19).
•The SSRI trials observed those receiving the drug for a relatively short period, making it impossible for many of the later onset side effects to be detected, (particularly the devastating SSRI withdrawals). This is similar to how after receiving an EUA, Pfizer and Moderna abruptly ended their placebo groups under the argument “it was unethical to withhold the life saving vaccination,” which in turn made there no longer be a control group which could prove the litany of chronic side effects following vaccination were indeed due to the vaccine. Sadly, this absence of evidence is often treated by the courts as there being “no evidence” those harms exist.
Note: as you might have guessed, the patients in those placebo groups were monitored for a much longer period than the SSRI recipients, which led to many more adverse events (e.g., suicide) being documented for the placebo group. For example, Pfizer produced a meta-analysis claiming Zoloft reduced the risk of suicide by 48%, but once an additional 29 days (of recorded data) was taken into account, their SSRI instead increased the risk of suicide by 47%.
•Many of the trials which yielded concerning data (even with every possible attempt being made to spin them in a positive direction) were simply never published (and in many cases not disclosed to regulators). For example, in 2004, a researcher used a comprehensive summary of internal reports of GSK’s trials (made available on the internet as a result of litigation) and found that Paxil increased suicidal tendencies by 177% (likewise numerous cases of self-injury, suicidal ideation and suicide attempts never made it into the public reports of GSK’s trials).
In one of the most memorable examples, after Pfizer got an antidepressant (Reboxetine) approved in Europe (but not the USA), a German institute asked Pfizer for all of their studies on it—which Pfizer repeatedly refused to do until the institute said Reboxetine would not be eligible for insurance reimbursement unless the institute had the data to see if it worked. Pfizer immediately complied, and the institute in turn concluded the drug was unsafe and ineffective. Sadly Europe’s FDA doubled down on their approval and simply unjustly attacked the institute for its conclusion.
Putting Lipstick on a Pig
In short, much of the clinical trial industry has evolved into finding elaborate ways to put “lipstick on a pig,” which in my opinion is largely a result of the mass media, medical academics, the medical journals, and the drug regulators being unwilling to call this behavior out and demand the trials be conducted in an accurate manner that will actually predict how the products will perform once they enter the market.
Note: in a recent article, I attempted to illustrate the systemic web of corruption which led to this.
One of the saddest things about this fraud is that doctors are trained to believe all drug side effects (especially from those their specialty regularly prescribes) are “anecdotal” unless there is scientific proof those side effects are real. Yet simultaneously, relatively few of them realize that the “peer-reviewed” articles they rely upon for that proof always censors pharmaceutical side effects. This in turn gives rise to the sad phenomenon of medical gaslighting (which for example we saw throughout the COVID-19 vaccine program).
Note: One of the best books I have found about psychiatry’s gaslighting is the aptly named Deadly Psychiatry and Organized Denial. That book was one of the primary sources for this series. According to it, some of the most common forms of psychiatric gaslighting include the suicides “just being [inconsequential] anecdotes,” the trials not showing a statistically significant increase in suicide (rather they only showed an increase of suicidal behavior), and that SSRIs protect agains suicide because they treat the undiagnosed depression that frequently causes suicide. Sadly, this is not that different from the logic vaccine fanatics use to justify more and more boosters despite the fact they are the primary ones still getting COVID.
John Virapen
It is exceedingly rare for a pharmaceutical executive to speak out against their industry (as doing so will permanently blacklist them from being hired again). In turn, the only ones I know of (besides an executive I’ve privately corresponded with) are Peter Rost and John Virapen, both of whom found themselves in very unique circumstances which enabled and compelled them to speak out against their industry and disclose the sociopathic behavior they observed within it.
Note: Rost’s story, along with similar accounts from the other Pfizer whistleblowers can be found in this article and this article.
One of the pharmaceutical executives directly involved in obtaining the approval for the original SSRI antidepressant, Prozac, developed a great deal of guilt for what he was complicit in once a large number of SSRI-linked deaths occurred. In turn, after he was unjustly fired, John Virapen chose to speak out.
Virapen chronicled those events in “Side Effects: Death—Confessions of a Pharma Insider.” These included outrageous acts of bribery to get his drugs approved, and photographing physicians with prostitutes provided by Eli Lilly so that they could be blackmailed into prescribing Lilly’s drugs. For those interested, this is a brief talk that Virapen gave about his experiences. I greatly appreciate the fact he used candid language rather than the euphemisms almost everyone else does:
At the start of the saga, Lilly’s senior management knew Prozac was garbage and wanted to shelve the drug, but since Lilly in dire financial straits they decided to go all in on the approval of Prozac in the hope it could save the company. Prozac, in turn, had initially been proposed as a treatment for weight loss (as this side effect of Prozac had been observed in treatment subjects). However, Lilly ultimately concluded (as explained above) it would be much easier to create the illusion Prozac treated “depression” and then get a post-marketing approval for the treatment of weight loss.
As Prozac took off, it became clear that depression was a much better market, and the obesity aspect was forgotten. Lilly then used a common industry tactic and worked tirelessly to expand the definition of depression so that everyone could become eligible for the drug and aggressively marketed this need for happiness to the public, before long, transforming depression from a rare to a common one.
Unfortunately, while the marketing machine had no difficulties creating a demand for Prozac, the initial clinical trial data made it abundantly clear that the first SSRI, Prozac, was dangerous and ineffective. Lilly settled on the strategy of obtaining regulatory approval in Sweden, and using this approval as a precedent to obtain approval in other countries. Virapen was assigned to this task and told by his superiors that if he failed, his career was over. Virapen, unfortunately, discovered that whenever he provided Lilly’s clinical trial data to experts, they laughed and had trouble believing he was actually seeking regulatory approval as Prozac’s trial data was just that bad.
Sweden (following their regulatory procedures) elected to allow an outside independent expert to make the final determination on whether Prozac should be approved or not. The identity of this expert witness was concealed, but Virapen was able to determine that it was Anders Forsman, a forensic psychiatrist and member of the legal council on the Swedish National Board of Health. After meeting with Virapen, Forsman proposed an untraceable bribe. Then, upon receiving payment, wrote a glowing letter in support of Prozac, fully reversing his previous position (he had ridiculed it just two weeks before) and guided Virapen through re-writing the trial to conceal the 5 attempted (4 of which were successful) SSRI suicides in it.
Forsman’s “expert” opinion resulted in Prozac being partially approved and formally priced for reimbursement in Sweden, which was then used as a precedent to market it around the world at that same lucrative price.
Note: After leaving Lilly, Virapen tried to have Forsman prosecuted for bribery. Despite the chairman for the Institute against Bribery submitting a report to the Department of Justice affirming bribery had indeed occurred, Forsman (who repeatedly lied throughout the process) was not prosecuted because he was not an official employee of the agency. Forsman in turn was allowed to continue his professional career and was employed by the state long after the investigation ended.
Virapen noted that during this time, German drug regulators who had clearly and unambiguously stated that Prozac was “totally unsuitable for the treatment of depression” suddenly reversed their position, leading Virapen to suspect that similar under-the-table activity must have occurred in Germany. David Healey, a doctor and director of the North Wales School of psychological medicine, likewise concluded that the German approval was due to “unorthodox lobbying methods exercised on independent members of the regulatory authorities.”
Note: A key reason why the German regulators initially refused to approve Prozac was because the specific criteria used for determining an improvement in depression was highly subjective and the benefit was only being reported by the trial psychiatrists but not the participants themselves.
Not long after saving Eli Lilly, Virapen was fired. Virapen believes he was fired because he was a man of color in an otherwise Caucasian company (he was told this by his supervisor). Peter Gøtzsche, a leading expert in pharmaceutical research fraud, on the other hand, attributed this to typical organized crime tactics where Lilly sought to conceal their illegal activity by firing Virapen and his two assistants (as immediately after their abrupt termination, none of them were permitted to access their offices, and thus could not obtain any of the files that proved that they had bribed Forsman).
In short, given how horrendous the data supporting their safety and efficacy was, you must be wondering how the SSRIs made it through the regulatory approval process.
George H.W. Bush
There is a lot of dark history to the Bush family. The Bush dynasty was founded by Prescott Bush, who built his family fortune by collaborating with the Nazis directly against the wishes of the U.S. government (The Guardian, for example, confirms it here). His son, George H.W. Bush had the unique accomplishment of being the only CIA chief to later become president, and during his brief tenure there was responsible for numerous crimes against humanity in South America. After leaving the CIA once Carter became president, Bush (senior) served as a board member for Eli Lilly. He then joined the Reagan Administration as Vice President, where he helped to push through the catastrophic decision for the FDA to approve aspartame for consumer use (aspartame was so dangerous even the FDA did not want to approve it).
After succeeding Ronald Reagan as President, Bush chose Dan Quayle as his Vice President:
In Talking Back to Prozac (1994), I pointed out that Prozac was approved under the first Bush administration and that George Bush had been a member of the board of directors of Eli Lilly, the manufacturer of Prozac. I also pointed out that Vice President Dan Quayle was from Indiana, the home state and international headquarters for Eli Lilly. At the time the FDA was approving Prozac, Quayle employed former Eli Lilly personnel on his own staff, and Quayle had considerable leverage over the FDA as the chair of a special committee that was investigating its operations. I questioned whether the FDA might have rejected Prozac and that the entire SSRI onslaught might never have gotten started if the president and vice president of the United States had not been so closely affiliated with Eli Lilly.
Bush’s son, President George W. Bush likewise followed in his father’s footsteps and appointed Eli Lilly executives to senior positions within his administration. In fact, he even inserted a provision into the Patriot Act to exempt vaccine manufacturers, including Eli Lilly, from liability for thimerosal (Mercury) within vaccinations.
In short, Bush profoundly changed the FDA’s regulatory conduct. Consider this example shared by John Virapen that occurred a few years before Bush became president. In 1980, Eli Lilly applied for the approval of benoxaprofen, and aggressively promoted this new blockbuster medication. Not long after being approved, in 1982, benoxaprofen was taken off the market after being linked to a small number of deaths, and Eli Lilly underwent a lengthy investigation conducted by the Justice Department, where it was concluded that Lilly intentionally covered up the deaths caused by their drug. Benoxaprofen is banned, but nothing remotely similar has been done for the SSRIs.
SSRIs and the FDA
The FDA’s treatment of the SSRIs is one of the only instances I know of, where, like the COVID vaccines, the agency has not only ignored, but actively tried to conceal a horrific number of adverse events for a pharmaceutical despite receiving widespread protest from the public. This was most likely heavily influenced by the Bush Administration being in bed with Eli Lilly. As such, it is insightful to see how this has played out over decades, as we ponder how the FDA will handle the COVID vaccines and what we need to do to address this mess.
First, consider the FDA’s behavior when Bush was not yet the president:
Initially, the FDA was skeptical and noted serious flaws in Lilly’s trials. An FDA officer wrote in 1984 that patients who didn’t do well after two weeks had their blinding broken, and if they were on placebo, they were switched to fluoxetine (resulting in six weeks of fluoxetine being compared to two weeks on placebo). An FDA review also discovered that 25% of the patients had taken an additional drug, and when the FDA in 1985 removed patients on other drugs from Lilly’s trials, there was no significant effect of fluoxetine. By adding benzodiazepines, Lilly broke the rules for its trials but didn’t inform the FDA, and when the FDA later learned about it, the agency permitted it and thereby broke its own rules. The public and the doctors were never informed about this ruse.
Prozac was ultimately approved in December 1987, at which point 3 of the 4 studies that this approval was based upon used benzodiazepines to conceal the agitating or psychotic syndromes created by the SSRI drugs.
Note: a good case can be made that many of the benefits attributed to SSRIs actually were due to the benzodiazepines that were used concurrently with them.
Once Prozac entered the market in 1988, adverse event reports began to accumulate, and by 1991, Prozac had one of the highest rates of adverse events ever reported to FAERS (similar to VAERS but for other pharmaceutical injuries). As there was less regulatory capture at the time, these red flags were sufficient to convene a Congressional hearing on the SSRIs (whereas today, except for one held a month ago by Congresswoman Marjorie Taylor Greene, this still has not happened for the COVID-19 vaccines).
Note: In the first nine years, the FDA received 39,000 adverse event reports, far more than for any other drug. In those, there were thousands of suicides (e.g., by 1999 over 2000 Prozac suicides had been reported), horrendous crimes, hostility, psychoses, confusion, abnormal thinking, convulsions, amnesia and sexual dysfunction.
A 1991 FDA hearing was convened where many witnesses told stories about out-of-character suicides and homicides. The advisory committee members, many of whom had financial ties to pharmaceutical companies producing SSRIs, ignored those reports and unanimously rejected the following proposal:
There is credible evidence to support a conclusion that antidepressant drugs cause the emergence and/or the intensification of suicidality and/or other violent behaviors.
Note: Internal Lilly documents revealed that the FDA had already been working with Lilly on the suicide issue (and that previously Lilly had disclosed to German regulators that Prozac doubled the risk of suicide compared to placebo). However, at the meeting, the chair of the FDA committee interrupted an outside expert who tried to share this, resulting in most of the presentation being conducted by Lilly employees who were able to present Lilly’s narrative to everyone). Similarly, at the time this hearing occurred, the FDA’s own employees had been raising concerns about the safety of Prozac. Furthermore, a later obtained document showed that the FDA knew that the suicide rate on Prozac was 0.52% (vs. 0.18% on placebo), and that in Pfizer’s Zoloft submission (which reported a 26% decrease in suicide attempts), when the FDA counted the deaths correctly, there was actually a 29% increase in them.
Sadly, buying out “expert” committees is a standard industry practice. To further illustrate the illegitimacy of these committees (who are entrusted to decide much of public policy), consider this report from Kim Witczak, a citizen activist who was able be appointed to one of them:
Fast forward, after Pfizer settled the Chantix lawsuits Pfizer went to the FDA to ask to have the black box neuropsychiatric warning removed from their drug label. By this time, I was the Consumer Representative on the FDA Psychopharmacologic Drugs Advisory Committee. We were going to review Pfizer’s new EAGLE study. I was really looking forward to being part of this committee and had many questions to ask about the safety, the lawsuits, the internal company documents discovered and reviewed by experts, and most importantly, the victims. After all, Pfizer just settled the lawsuits for almost $300 million and silenced everyone. One would think the FDA committee would want to have all information including what was discovered in lawsuits involving 2700+ victims before making any decisions to remove the warnings.
A few days before the FDA Advisory Committee, I received an email from the FDA that they wanted to talk with me about the upcoming advisory committee meeting. Someone (cough Pfizer) brought it to their attention that I had an “intellectual bias” and shouldn’t serve on the committee. The roomful of FDA staffers told me that I was being recused from serving on this meeting. I told them if they think safety is an intellectual bias (or a point of view), I will always have one.
Much to their surprise, I said I would still like to address the committee and speak during the open public hearing. I ended up flying out a few days later on my own time and dime to make sure my comments and questions were asked even though they wouldn’t be part of the official public record of this meeting.
Ultimately, in an unprecedented move, the FDA removed this serious black box warning that involved violence, hallucinations, suicide, and other psychiatric side effects. To this day, this story has never really been told by the media. These side effects didn’t suddenly go away. Just the FDA black box warnings.
As detailed above, lawsuits against SSRI manufacturers like Lilly have repeatedly revealed those companies deliberately concealed the adverse events that occurred in their trials. Similarly, Lilly also chose to commit fraud by illegally failing to report 76 of 97 cases of suicidality from Prozac in a post-marketing surveillance study it submitted to the FDA.
Furthermore, Lilly also failed to report that, Cymbalta, an SNRI frequently marketed for treating chronic pain, was found to cause severe withdrawals once discontinued in half of those who had received it for at least 8 weeks. In turn, in the first quarter of 2012, more reports were submitted to the FDA on serious drug withdrawal effects for Cymbalta than for any other regularly monitored drug, including two opioids.
Note: Paxil is also notorious for being highly addictive (e.g., in their original license application they stated 30% of trial subjects experienced withdrawals), but for the first ten years it was on the market, GSK adamantly claimed it was not addictive. Eventually (in 2001) the WHO stated Paxil had the greatest withdrawal issues of any SSRI on the market (which was followed by a warning from the FDA in 2002). GSK in turn finally “admitted” this by revising its prescribing instructions to state the risk of withdrawals was not 0.2% but instead 25% (a 125 fold increase).
Organized Cover-Ups
One of the most blatant examples of how far the FDA will go to protect the industry occurred in 2003, when while examining a clinical trial for giving Paxil to children, the FDA noticed that more episodes of “emotional lability” (rapid, often exaggerated changes in mood) were reported in children on Paxil than those on a placebo. The FDA decided to investigate what the actual symptom Paxil’s manufacturer was concealing behind this label, and was informed most cases referred to suicidality. One of the FDA’s safety officers, Andrew Mosholder, a child psychiatrist, further investigated this issue and concluded that 22 studies showed that children given antidepressants were nearly twice as likely to become suicidal as those given placebos.
His superiors at the FDA who had recently hidden Paxil’s tendency to cause suicidality in children predictably disputed his report, and did not allow it to be released to the public or presented at an advisory meeting. A year later in 2004, the report was leaked, and in a very telling move, the FDA chose to conduct a criminal investigation of the leak rather than address the clear safety concerns it had raised.
Kim Witczak spearheaded many different initiatives against the SSRIs. For example, she filed a wrongful death, failure to warn lawsuit against Pfizer (which Pfizer responded to by sending investigators around her neighborhood to dig up dirt on her). Her lawsuit was able to obtain many crucial documents from Pfizer proving that they knew how dangerous their SSRI was (including the same out-of-body experiences which her husband had had before killing himself). Her lawsuit eventually provided the ammunition to get a black box warning (easily visible red-alerts the FDA occasionally mandates for pharmaceuticals) placed on the SSRIs.
Note: documents showed that Lilly initially planned to have a warning for Prozac causing psychosis in the USA package insert, but ultimately only did so in Germany, as their regulators, unlike the FDA, required Lilly to insert this warning.
Because of her efforts, like the previous example showed, Witczak was provided with a direct view into the corruption within the FDA. For example, this is how they addressed the “problem” that lawsuits against the SSRI manufacturers were causing their confidential documents (detailing the actual harms of the drugs) to be released:
Pfizer used the FDA to intervene in Baum Hedlund’s civil lawsuits. It was discovered that Pfizer paid industry defense lawyer Dan Troy $300k for some legal work shortly before he was appointed FDA Chief Counsel by President Bush. In his new role at the FDA, Dan Troy was the mastermind behind the FDA preemption amicus “friend of the court” brief intervening on behalf of pharmaceutical companies in civil lawsuits. The brief [falsely] argued that because drug was FDA approved, the lawsuits were “preempted” and should be dismissed.
The brief [falsely] claimed even if a company wanted to warn consumers, the FDA wouldn’t let them update their warning label if the FDA didn’t agree. Many Zoloft suicide lawsuits were tossed out by judges who believed the FDA was final authority on the drug label. Pfizer even tried arguing the FDA preemption brief in my lawsuit. Not once, but twice. Federal Chief Justice James Rosenbaum disagreed with Pfizer and allowed my lawsuit to proceed.
We worked with NY Representative Maurice Hinchey to help expose the $300k Dan Troy received from Pfizer. Ultimately Dan Troy resigned his FDA Chief Counsel post but not before damage was done. He ultimately went back to work for private industry including becoming global Chief Counsel at GlaxoSmithKline, the maker of Paxil, another SSRI.
Sadly, paying off regulators (e.g., by giving them cushy jobs of the pharmaceutical industry) is very common (the practice is known as the “revolving door”). For instance, many of the authors of government studies (e.g., FDA employees) who questionably determined the SSRIs were “safe and effective” were also paid off by the SSRI manufacturers.
In 2004, due to the mounting political pressure, the FDA finally released a black box warning linking SSRIs to increased suicidality in children. Despite knowing about this problem long before the SSRIs came to market, it took over two decades for the FDA to provide this critical warning. More importantly, this only happened after massive public pressure, countless lawsuits proving these effects were deliberately concealed by the manufacturers, public hearings, and leaked reports publicly shaming the FDA.
Note: in 2006, the warning was extended to everyone under the age of 25. As this cut off was completely arbitrary (many of the SSRI suicides occurred in much older individuals) a large press conference was organized the day beforehand so those believing it needed to be applied to all ages could have the time to speak the FDA would not permit them to have during its hearing. Although their action did not convince the FDA to change course, next year in 2006, the FDA did and applied that warning to all ages groups.
By 1990, the public was demanding for the FDA to determine if SSRIs were linked to increased suicidality. As the evidence proving this was unambiguous, the FDA deliberately avoided publishing a report on this topic. Sixteen years later, shortly after the FDA was exposed for suppressing the link between suicidality in children and SSRIs, the FDA finally published a meta-analysis addressing this question. The 2006 meta-analysis encompassed 372 placebo-controlled trials of SSRIs (and related drugs) involving 100,000 patients, and showed that up to the age of 40, SSRIs increased suicidal behavior, while in older patients SSRIs decreased this risk.
Note: A common tactic in the pharmaceutical industry is to hyper-focus on one specific set of side effects so that the other side effects can be covered up. For example, from comparing the incidences of blood clots I hear about relative to the percentage of people who chose the J&J vaccine, I am relatively certain that the mRNA vaccines are more likely to cause blood clots than J&J’s, but whenever this topic is raised, people default to believing only J&J can cause blood clots since it was linked to a few cases of central venous thrombosis and there was a brief period where the vaccine was suspended by the FDA to “assess” this risk.
I suspect that the FDA’s long-delayed meta-analysis and the black box warning were a direct response to the leaked report proving an indisputable link between SSRIs and adolescent suicidality that was produced to shield the other side effects from scrutiny. Sadly, these warnings have done very little to curb the usage of these drugs, as evidenced by how large their market has become. Rather they served as a way to protect that market as they both were an alternative to pulling the drugs (which is what should have happened) and downplayed the side effects as much as possible (e.g., borrowing from the industry’s playbook, “abnormal thoughts” became abnormal dreams).
Furthermore, the FDA’s meta-analysis almost certainly also understated the risk. For example, the FDA gave the studies they analyzed a free pass on the variety of design flaws that made it easy to conceal their adverse events. In fact, the FDA reached out to many of the SSRI manufacturers and asked them to adjudicate (remove) possibly suicide-related adverse events in their trials as they saw fit and send those results to the FDA.
When analyzing the 2006 meta-analysis, Gøtzsche found numerous other signs of deliberate fraud by the FDA. For example, in many cases (often due to data revealed from litigation), a single study within the meta-analysis was shown to contain more cases of suicide from an SSRI than the 5 suicides the FDA claimed had occurred throughout all 372 of its studies.
From extensively reviewing all the data, Peter Gøtzsche, reached the overall conclusion that there are likely to have been 15 times more suicides on antidepressant drugs than reported by the FDA in its 2006 meta-analysis.
Note: In 2006, 35 million was spent by American’s National Institutes of Mental Health to conduct the STAR*D study, which assessed if SSRIs cured “treatment resistant” depression (making it the largest study on SSRI efficacy ever conducted) and was designed to assess typical patients in real life scenarios (although the care they received was likely better than what is seen in clinical practice). It found 3% or less of subjects had their depression cured (with it not remitting for the year of observation within the trial). However, the NIMH repeatedly stated “about 70% of those who did not withdraw from the study became symptom-free,” significantly exaggerated the improvements in the patients, and that SSRI treatment was far more effective that placebo, despite no placebos being used in the trial.
In my personal opinion, when your results are off by an order of magnitude, this can only occur through deliberate fraud, something many of us have regrettably come to realize has occurred at both the CDC and the FDA throughout the COVID-19 vaccination campaign. As it so happened, by 2013, the FDA employee in charge of the 2006 meta-analysis had completely transitioned to the private sector and had made a consulting firm dedicated to helping psychiatric drugs sail through the FDA.
Note: a variety of other large studies have used similar methods to conceal the dangers of the SSRIs. Since I can’t cover all of them here, I chose to focus on ones conducted by the US government.
The Big Lie
When Hitler wrote Mein Kampf in 1925, he described how people could be induced to believe a colossal a lie because they would not believe that someone “could have the impudence to distort the truth so infamously.” While he initially used this idea to attack others (e.g., the Jews), before long he fully adopted it, allowing the Nazi regime to become one of the most powerful forces of propaganda in history.
Many others have also used this approach. For example (as discussed in a recent article), for decades, US health authorities (and professional medical associations) have repeated the mantra that their vaccine is “safe and effective” while simultaneously suppressing all evidence to the contrary (e.g., from their own scientists). This in turn has resulted in numerous disastrous vaccines (which everyone knew were bad) being pushed onto the market and not being taken off until a significant amount of injuries had occurred.
With the SSRIs, we see a similar degree of audacity, as time and time again the SSRI advocates will insist their drugs are safe and effective despite all evidence to the contrary. For example:
In 2014, the medical director at the Norwegian drug agency, Steinar Madsen, said at a meeting that antidepressants work for 50-60% of the patients. I [Peter Gøtzche] replied that his statement illustrated why we cannot trust our drug regulators and reminded him that the FDA had found in their analysis of 100,000 patients that antidepressants worked for only 10% of the patients.
Throughout the 1990s, while swearing publicly that fluoxetine didn’t increase the risk of suicide or violence, Lilly quietly settled lawsuits out of court and kept the incriminating evidence hidden by obtaining court orders to seal the documents.
[In 2011 the CEO of a company that sold five antidepressants], claimed in a radio programme that SSRIs reduce suicides in children and adolescents. When the stunned reporter asked him why the package inserts warned against suicide attempts, also for Lundbeck’s drugs, he replied that he expected the leaflets would be changed by the authorities!
The radio interview took place while Lundbeck’s US partner, Forest Laboratories, was negotiating compensation with 54 families whose children had committed or attempted suicide under the influence of Lundbeck’s antidepressant drugs.
[BBC Journalist] Shelley Joffre, showed that the GSK spokesperson, Dr Alastair Benbow, lied in front of a running camera. He denied, for example, that paroxetine could cause suicidality or self-harm while he sent data to the drug regulator one month later that showed exactly this, and which immediately led to a ban on using paroxetine in children.
Note: The UK drug regulators also lied to the public to cover for GSK (which is based in the UK) by stating that the discovery Paxil caused those suicides was completely new to the company (whereas documents showed it had in fact known about it for at least eight years). Furthermore, when US senator Charles Grassley later asked GSK for how long the company had known that paroxetine increases the suicide risk, GSK repeated this lie, claiming GSK had not detected the risk until 2006.
Given their willingness to blatantly lie, even to a US Senator, it should come as no surprise these companies concocted elaborate ways to silence their critics. For example, GSK has publicly stated:
Major depressive disorder is a potentially very serious illness associated with substantial morbidity, mortality, suicidal ideation, suicide attempts and completed suicide. Unwarranted conclusions about the use and risk of antidepressants, including paroxetine, do a disservice to patients and physicians.
Many psychiatrists (especially those being paid off by the pharmaceutical industry) in turn have used similar arguments to silence all criticisms of their drugs.
Sadly these tactics are not unique to the psychiatric industry. For example, in a previous article I discussed the significant dangers (and complete lack of benefit) from statins. In turn, whenever statins are questioned, rather that defend them, cardiologists will often insist you are “killing patients” by scaring them away from the drugs, and this argument has been successfully against both physicians and news programs which questioned statins.
In turn, as you might guess, that tactic has also been used against critics of the SSRIs.
In New Zealand, psychiatrists and suicidologists managed to convince the government [with very weak evidence] that publishing information on suicides causes copycat suicide, which in turn made it a criminal offense for victims or the media to publicly discuss SSRI suicides.
Likewise, this same playbook has been used against critics of a controversial vaccine. Sadly, since there had been numerous trial runs with other deadly products, by the time COVID-19 happened, the “dangerous misinformation” playbook had been developed, and that label was immediately plastered onto anyone who questioned any part of the pandemic response (e.g., the lockdowns, the suppression of early treatment or the COVID-19 vaccines).
This in turn set the stage for where it somehow became acceptable to argue people should be forced to vaccinate against their will despite a significant amount of evidence (and public opinion) existing that argued against vaccinating. In many ways, this is not that different from how psychiatric medication mandates are often pushed upon patients who (due to their side effects) simply do not want them.
Note: there are many sad stories of this—including numerous ones where the courts supported the psychiatric mandate no matter how much work was done to overturn them.
Conclusion:
In my eyes, one of the most important things to consider in this article is just how many people are taking SSRIs, and by extension, just how many injuries the percentages I provided in this article translate to. Whenever a drug is being considered for approval, one of the primary concerns by the regulator used to be the total expected harms suggested by the preliminary data—yet as we can see both in the SSRI saga and throughout COVID-19, that principle has simply been discarded.
As I ponder how things could have gotten this way and how symbiotic the relationship has become between the pharmaceutical companies and the drug regulators, I am reminded of this iconic scene from Idiocracy:
The saddest thing about the SSRI saga is that as inexcusable as it was, things were much less corrupt then than they are now, especially within the federal government. At the time that the public challenged the SSRIs, the media would air stories critical of the malfeasance within the federal government and lawsuits could compel the pharmaceutical companies to disclose the harms they were hiding from the public, and Congress was willing to investigate.
Now, all the vaccine manufacturers have almost complete protection from liability and except for a few commentators on Fox News, no one so much as dares to question the vaccines (or any other pharmaceutical for that matter).
One comment Kim made on our sad state of affairs really stuck with me:
Note: Renowned journalist Sharyl Atkinson has made an excellent case the prolific censorship we have become accustomed to began during the Obama presidency.
My hope is that the harm of the COVID-19 vaccines is so egregious and unambiguous, and more importantly, has affected so many people, that it will prompt enough public outcry to fix or at least improve this systemic corruption.
I thank each of you for reading through this rather lengthy article and your continued support of this Substack (you make the work I do here possible). In the final part of this series, I will discuss how the pharmaceutical industry created the market for depression and the best (non-pharmaceutical) approaches I have found for actually addressing it.
Lastly, if any of you are considering stopping a psychiatric medication, for your own safety, please do not do so until you have discussed the subject with someone who has clinical experience in this area. Since tapering off a SSRI is a complex subject, I tried to provide a comprehensive discussion of it here.
One thing that I have noticed as a regular citizen is that we have all been trained to almost completely ignore any warnings or information on the inserts about adverse reactions of any medication or injection. I suspect it’s because of the endless commercials for prescription medications that show happy, smiling, healthy people with upbeat music doing fun things while a kind sounding voice discretely says that “death may occur”. I don’t think our minds are able to grasp such a shocking message while fun music and happy people are dancing around the tv screen. It’s a true PSY-OP every time someone turns on their tv.
If it were just a matter of making money, they could release safe placebos.
In my opinion, they seek not only to rob us, they want to hurt and kill us. That includes our own government.