Why Medicine Won't Cure You (and What's Finally Changing)
The predatory business model that requires lifelong patients faces its first federal challenge with Kennedy's historic SSRI initiative

Story at a Glance:
No industry, organization, or cause tasked with solving a problem will actually solve it, because the problem disappearing threatens their economic livelihood or political power—a dynamic visible everywhere from non-profits which constantly seek donations but never produce results to dating apps that deliberately prevent users from finding partners and leaving the platform.
The pharmaceutical industry has perfected this model: drugs are designed to be taken perpetually rather than cure, side effects create demand for additional drugs, and the entire regulatory apparatus is structured to protect this status quo by suppressing affordable natural therapies like DMSO that challenge it.
SSRIs epitomize this dynamic—massively overprescribed, frequently life-ruining, and nearly impossible to withdraw from—yet for decades, the industry successfully kept all criticism of them out of mainstream discourse.
Recently, efforts to connect SSRIs to mass shootings shifted the Overton window, making SSRI injuries gradually become acceptable to discuss, culminating in Secretary Kennedy recently holding a panel where victims shared devastating testimonies of what SSRIs had done to their lives.
Kennedy then announced a multiagency federal effort to combat inappropriate SSRI prescribing, train providers in how to correctly taper patients off antidepressants, and provide non-pharmaceutical alternatives—marking the first time in memory a federal health initiative has aimed to help get patients off a major drug class rather than on one.
Conversely, those who embrace the constant challenge of actually solving problems rather than managing them—in medicine and elsewhere—consistently find it is the most fulfilling way to practice, which is why Kennedy's approach of giving physicians a supportive framework to break from the status quo holds so much promise.
When I was in high school, I observed a few discouraging events which led me to postulate: “no industry, organization or cause tasked with solving a problem will actually solve it because the problem disappearing threatens their economic livelihood or political power.” Since that time, I have observed more examples than I can count in so many different spheres that I’ve accepted this dynamic is a common feature of society, and likewise, have come across many similar observations by others, my favorite of which was:
Nothing is so permanent as a temporary government program—Milton Friedman
Recently two noteworthy examples of this principle came to my attention.
First, a frustrated patient shared with me they’d recently learned all of the online dating apps had switched from formats which allowed people to find suitable long term partners (e.g., with lengthy compatibility surveys) to ones which prevented people from matching because if someone found a good match on a platform, they would then stop paying more money for the service, whereas if they were hooked on it and spending hours each day trying to find someone, they would be a sustainable source of revenue. More remarkably, once one company figured out this approach made more money, they bought out all of their competitors (sometimes with threats of spurious lawsuits) and shifted them all over to this predatory model as well (all of which is detailed in these six articles1,2,3,4,5,6). I found this example noteworthy as:
One of the greatest sources of distress I find in patients (particularly now) are relationship challenges, particularly a lack of one, and I believe much of this traces back to apps taking over courtship.
Beyond the personal cost this dynamic creates, one of the largest challenges most developed countries are facing is a low birthrate which is primarily due to low marriage rates. My belief, in turn, is that many of the heavily contested policies we are seeing (e.g., reducing social support for the elderly, mass migration, or replacing workers with robots or AI) ultimately are due to the fact policy makers believe the declining birthrate means it will not be viable for the younger generation to support the society (particularly the elderly) so alternatives need to be found regardless of how objectionable they are.
A common cycle predatory industries in America follow is presenting a “superior” way to meet an essential need of humanity that replaces the traditional one that’s worked, then once the old one is completely displaced, tightening the screws with the new one (to milk as much out of the population as possible) until things are far worse than what preceded it and massive social cost is accrued (e.g., the Rockefellers did this in various ways with food, energy, and medicine).
Note: because online dating has now become so bad, the companies that monopolized the market are starting to lose a lot of users and money, signaling there may be a chance for this cycle to reset itself.
Second, a federal DOJ indictment recently charged the SPLC (one of the country’s leading civil rights groups that built its reputation fighting hate) with wire fraud, bank fraud, and money laundering. Prosecutors alleged it paid over $3 million in donor funds to informants embedded in white supremacist groups (including the KKK and National Alliance) while soliciting donations to “end hate,” and that one paid informant participated in planning chats, attended, and helped with logistics for the 2017 Charlottesville Unite the Right rally. Many, in turn, were outraged about this, in part because of how much political capital was extracted from the event (e.g., Biden made opposing it a central justification for his 2020 presidential campaign and Harris to a lesser extent did so as well in 2024) but also because of just how much money it made:

Unfortunately, these are far from isolated examples, and it would be impossible for me to cover even a sliver of them here. As such, this article will focus on how this principle applies to medicine and why I believe beyond greed, complacency also plays a central role in the continual recurrence of this dynamic across societies.
Is Money The Root Of All Evil?
The origins of our faith and devotion to money have raised many questions throughout the ages. The love of money, in turn, has long been recognized as one of the most powerful forces for twisting human hearts towards evil (which often results in immense destruction to the people or the environment), while simultaneously, its value is often completely arbitrary—money gets printed and then assumes value because everyone holds a collective faith in it the ruling class controls us through. At the same time, money is a remarkable force for both developing and organizing society, and many of the things we depend upon are only available to us because of the economic system we live within.
When the question of money is looked at, it is often seen through a lens of greed being a deadly sin. However, I would argue the core issue is that for many people, effectively accumulating money becomes the foundational axiom (guiding principle) used to navigate life, causing them to rationalize a variety of unethical positions (they often lie about) to make money, because their internal algorithm will frequently default to the choice that acquires more money. Recognizing this, in turn, provides an invaluable tool for understanding the world around you, as the motivations of others often become far clearer once you cut through all their rhetoric and view things strictly through what they stand to profit from.
Algorithms of Business
In the same way that a default behavior to seek the most profitable choice helps to explain many of the individual actions we observe around us, businesses also follow a relatively predictable set of behaviors aimed at optimizing profit, which you can see in a wide range of industries.
In general, most large businesses aim for the following, prioritizing whichever are most feasible:
Continual growth
High markups on their product
The widest possible market
Market exclusivity (to protect and maximize sales)
Repeating sales far into the future
The main problem with this framework, which society largely applauds and equates with success, is that businesses routinely prioritize profit, even when it conflicts with the interests of customers or society. Because of this, we frequently see:
Artificial “needs” being created through marketing, making unnecessary products seem essential.
Harmful products (environmentally damaging or toxic to humans) being aggressively marketed and kept on the market despite the damage.
Extreme markups on essential products, pushing dependent customers closer to poverty.
Monopolies and exclusivity tactics used to block competing (and often better) solutions from entering the market.
Products deliberately designed for repeat purchases rather than full solutions, such as planned obsolescence or proprietary consumables (e.g., Gillette’s classic “razor-and-blades” sales model, and its modern equivalents like Amazon’s sinus irrigator that only works with its expensive proprietary pods that you quickly run out of).
The pharmaceutical industry, not surprisingly, excels in all of these, which helps to explain why they have managed to sustain steady growth for decades, and why one-fifth of all money spent in the United States goes to healthcare despite our country receiving very poor returns on that investment.
Note: annual adult vaccines (which frequently do nothing. particularly because they are often for the wrong strain) are an excellent example of an unsafe, unproven and ineffective product that is pushed on everyone because it fulfills the need for perpetually recurring sales.
Lifelong Patients
A frequently shared meme highlights that members of the medical community frequently face the same dilemma dating companies do.
The more time I’ve spent in medicine, the more I’ve come to appreciate that many principles you see in business are not only replicated in medicine but inevitably will guide medical practice. For example, much of modern medicine is only possible because it has successfully made the case it represents the “pinnacle of science” and that medical services are both essential and deserve a premium price far exceeding what anyone else has paid historically (which allows immense amounts of American money to be invested into creating medical infrastructure and developing new therapies).
At the same time, this creates an inherent conflict of interest for the entire profession, as if major disease categories are “solved,” the lobbying power (which the industry depends upon) is reduced, and funds allotted to treating or researching that condition dry up. Most importantly, the entire industry (and regulatory apparatus) is structured around this status quo, so anytime someone tries to deviate from it, countless stakeholders will emerge to oppose it.
This was best demonstrated by a 2018 report which provoked considerable public outrage when it was publicized by the mainstream media:
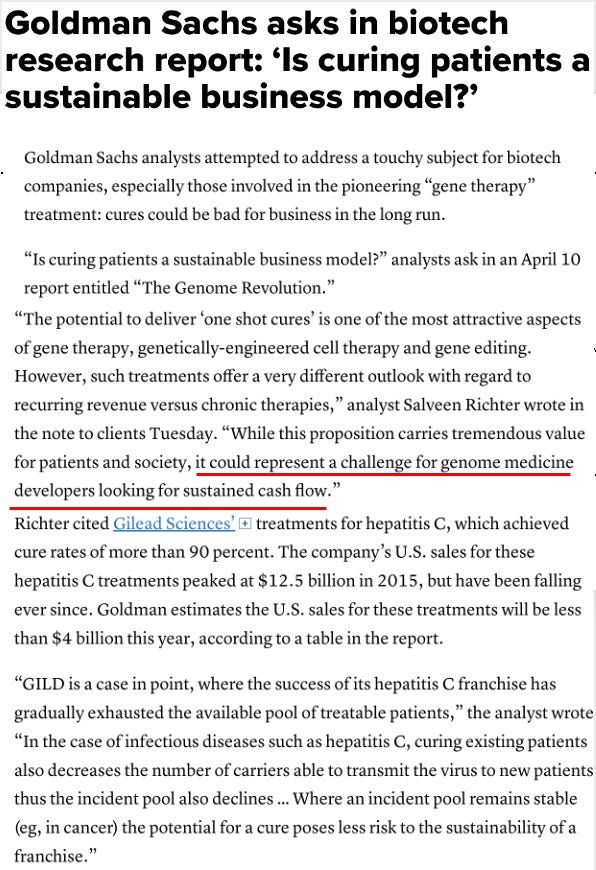
Note: while I can’t prove this, given how rarely the media will expose pharmaceutical misconduct, I believe the reason it did in this specific case was not to help the public but rather to send a message to the industry (and investors) to avoid curative genomic therapies.
All of this, I believe, helps explain why, while many competing therapies will always exist, the medical industry (and regulators) will only target the ones with the potential to scale up enough to meaningfully compete with their bottom line (e.g., we all saw what happened to the off-patent COVID-19 treatments like hydroxychloroquine and ivermectin). In contrast, there are many effective alternative therapies I know of which receive very little pushback from the industry because it will never be possible to deploy them at a scale which meaningfully threatens the industry’s bottom line.
That likewise touches upon a core dilemma I face writing this newsletter: many of the approaches we use (like neural therapy) which (often rapidly) get excellent results for patients are offered by very few physicians and require extensive training to administer optimally. As such, if I focus on them, it’s essentially useless information, as most readers will just feel frustrated they can’t access the therapy (or might end up with someone who does not correctly administer it to them). Likewise, there are many excellent therapies we sometimes use, but in very similar cases don’t, because their interactions with the body make them inherently unsuited for universal protocols (which is a big part of why I have not focused on cancer treatments here).
Because of this, I chose to discuss the therapies we use just enough so that when someone who is likely to benefit from them gets the opportunity to use them, they will be able to recognize the value of that opportunity, but I try to refrain from reaching the point where I feel I’m just wasting your time by telling you about something you won’t be able to use.
Conversely, I have put an immense degree of effort into presenting and accurately laying out how DMSO works, what it can treat and how to use it here because it’s very safe (and costs close to nothing), it has a very wide range of conditions it treats (including many “incurable” ones), and it’s effective enough that the majority of people who use it will experience significant benefit (which is why I’ve now received over 6,000 DMSO reports from readers and this newsletter has reached so many people).
However, despite the focus I’ve given to DMSO here, it’s not actually the primary thing we use in practice. Rather, prior to starting this project, my position was:
DMSO (especially IV DMSO) is life-changing for challenging neurological conditions, especially strokes (discussed here and here).
DMSO is an excellent first aid tool (e.g., for injuries or burns) that if possible should always be in your first aid kit.
DMSO is a significantly more effective and vastly safer NSAID (or Tylenol) alternative for treating tissue injuries and pain (discussed here) and one of the most potent anti-inflammatory options out there—which some patients really need (discussed here).
You can do a lot of really useful things by combining DMSO with another (typically natural) agent and applying it to the skin (discussed here and here).
DMSO is very helpful for herpes and one of the few ways you can reverse antibiotic resistance (discussed here).
DMSO has a lot of different therapeutic effects, most of which are similar to what many of our preferred therapies do. However, the key difference is that DMSO is more broad but less potent than them.
As such, DMSO was more of a “tool in the toolbox” I used when it made sense rather than my primary modality, and I was mostly just outraged it had not seen wider adoption for some of these uses (e.g., strokes or an ibuprofen alternative) since there is such a massive need to have better therapeutic options in those cases (making it be one of the clearest examples of FDA malfeasance, particularly since the FDA stonewalled it for decades despite extensive proof it worked, widespread public and scientific protest, and multiple Congressional hearings).
So, when I started this series, my goal was essentially to elucidate those six points, provide something beneficial everyone here could actually use without needing a difficult to find expert in the field, and try to put 3 months (or maybe 6) into it because I felt the subject had not been given the attention it deserved. Put differently, I never expected DMSO to be the focus of this newsletter or that years of my life would go into researching it (there are other therapies I planned to extensively discuss here). That essentially happened because:
•I saw that there was vastly more pertinent DMSO literature than I had initially imagined (much of which exists outside the databases AI systems use and hence is unlikely to ever be seen).
•From that I discovered DMSO excelled in certain conditions I had not previously known its value in, many of which otherwise are quite hard to treat (e.g., for the eyes and for the lungs).
•The efficacy readers were reporting for DMSO (across a broad swathe of ailments) was higher than what we’d seen since it was rarely the primary therapy we utilized.
•I realized DMSO (due to its ability to partially improve a variety of critical but immensely underappreciated aspects of health) provided an excellent vehicle for elucidating many of the concepts I’d wanted to cover.
•Due to the difficulty of this project and DMSO costing so little that no advertiser will make enough to fund promoting it, I realized it was unlikely anyone else would take the time to compile all the relevant information on DMSO, so it felt like I had an obligation to do the project.
Medical Sales Funnels
In many ways, addictive street drugs represent the purest distillation of the business framework I outlined earlier: it’s easy to continually expand the market by creating new addicts, once people are addicted they will do anything to get the drug (making it possible to sell at a high markup and ensure a large volume of repeating sales), and because it’s so profitable, funding is available to neutralize competitors (e.g., with cartel violence) so market exclusivity is maintained.
Conversely, this business model comes with a massive cost, as it not only removes its customers from productively contributing to society (as their lives are lost to addiction) but also disrupts the lives of those around them (e.g., through the crime needed to fund addictions, turf violence as rival groups compete for customers, and increasing corruption as they try to rope the government into supporting their enterprise). Because of this, for centuries this “ideal” business model has recurred across societies regardless of how harsh the measures governments take to stop it.
One of the most common critiques of the pharmaceutical industry is that the entire enterprise is a more sophisticated form of this model: the drugs that are widely sold are designed to hook people for life and the immense lobbying the industry can afford (so the government supports them) effectively takes the place of cartel violence to maintain their market monopoly.
Note: other common criticisms include several of the largest pharmaceutical companies (e.g., Bayer via IG Farben) having been deeply entwined with Nazi Germany, and that many major pharma firms were once leading marketers and manufacturers of cocaine, methamphetamine, and heroin (Bayer famously marketed heroin as a “non-addictive” wonder drug).
Furthermore, unlike classic drug enterprises which have to market their products from the shadows, the state sanctioning of their business model makes it possible for them to publicly market the products to the entire society, acquire far more customers than an illegal enterprise ever could, and buy out both the media and government so criticisms of their products are not allowed to be aired.
Seeking to maximize profit, the industry hence seeks out "blockbuster" drugs and feeds each one into their robust sales apparatus. For this model to work, as the Goldman Sachs memo illustrates, the drugs need to be taken perpetually so curative ones that are taken briefly are not permissible.
Note: a significant amount of the research I cite in this newsletter originates from less wealthy countries with robust scientific infrastructure (e.g., Russia). I believe this is because those countries cannot afford to subsidize costly perpetual medical care, and hence are motivated to explore less costly options that can cure illnesses and require far fewer administrations.
Fittingly, the medical profession has largely moved away from the language of “cure.” For centuries, major medical dictionaries—including the Oxford Concise Medical Dictionary, Bantam Medical Dictionary, and Barron’s Dictionary of Medical Terms—either omitted a clear definition of “cure” or defined it only minimally.1 2 The word is also notably absent from the indexes of core references such as Merck’s Manual and Harrison’s Principles of Internal Medicine.1 2 In practice, physicians are strongly discouraged from promising or even declaring a “cure” in many contexts, particularly for chronic conditions. You cannot be accused of failing to achieve something the profession rarely claims is possible.
Note: while this linguistic caution is understandable as it helps protect patients from false hope and physicians from liability when relapses occur, it simultaneously fosters a toxic cultural mindset in which “managing” chronic conditions becomes the ceiling rather than the floor, discouraging both doctors and patients from diligently pursuing root-cause resolution or promising alternative therapies.
Because of this, every successful pharmaceutical lies somewhere along a spectrum of being "addictive" to "ineffective." Much of this results from the fact the body is designed to maintain homeostasis and resist unnatural alterations of physiology, so since most drugs work by inhibiting an enzyme, inhibiting a receptor, or stimulating a receptor, the body will counteract this by creating the opposite effect. As such, the human response to medications is frequently either:
•For the effect to be temporary and only last as long as medication is there
•For progressively higher doses of the medication to be required to elicit the same effect
•For the body to shift to an unnatural baseline where it can no longer function without the artificial counterweight of the medication (which in many cases equates to a chemical dependency and addiction to the drug because of how severe the withdrawals are).
Note: sometimes additional steps are involved. For example, acid reflux frequently results from a lack of stomach acid (which prevents the top of the stomach from getting the signal to close) which argues for supplementing meals with stomach acid (that beyond frequently curing reflux, provides numerous other health benefits). However rather than do this, the preferred approach is to completely suppress stomach acid production so nothing is there to reflux, making it very difficult to stop the medications because once small (insufficient) amounts of acid return, they will reflux and cause heart burn.
Since this business model is so reliable, my view is that it’s inevitable more products than I can count will emerge to support it and it’s an exercise in futility to stop it. Because of that, my focus has been directed to three areas:
•Identifying the (typically non-addictive) pharmaceutical drugs which I nonetheless think make a lot of sense to use in certain contexts.
•Finding better alternatives to the commonly marketed drugs.
•Directing my energy towards opposing the most harmful (rather than useless) medications.
Sadly, despite restricting my focus to the last category, there’s simply no shortage, as beyond the design of pharmaceutical drugs inevitably producing side effects (due to some of the functions they suppress being essential for health), those side effects are often actually an upside for the industry because they create additional problems that require other drugs to treat, hence creating a robust “sales funnel.”
“Sales funnels” for context, are a classic marketing concept: cast a wide net with a low cost (or free) product with a high rate of conversion, pull a certain number of those caught into buying a more expensive product, and then in each successive funnel, get a smaller number of people to buy an even more expensive option.
When observing medicine, I hence cannot help but notice just how many things in it are effectively sales funnels (e.g., general practitioners not only function to provide a steady stream of patient referrals to the more expensive medical services, but also, for “wellness” give patients a large number of tests that convert a significant number of patients into taking the common lifelong drugs which half of American adults are on at least one of).
SSRI Antidepressants
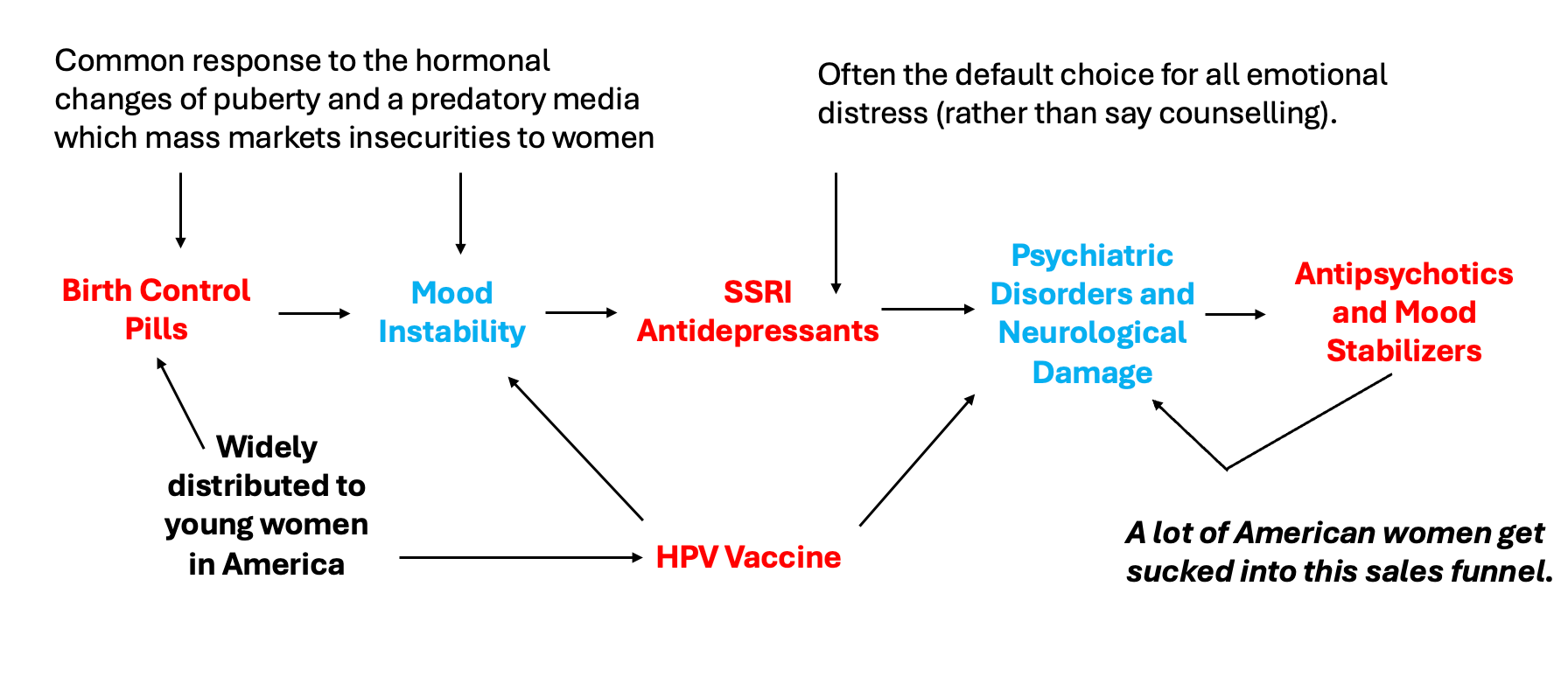
From the start, I decided to focus on SSRIs as while they significantly help a subset of patients, I also feel they are one of the worst offenders on the market. Beyond being massively overprescribed, they frequently ruin people’s lives (often in very cruel ways), are often nearly impossible to withdraw from, and have predatory sales funnels that affect large numbers of American women:
Unfortunately, SSRIs languished in the same place many other toxic drugs did: they harmed a significant number of people but the drugs made enough money (one in six adults take psychiatric medications) that it was possible for industry to corral the entire government and media into sweeping them under the rug, so this issue remained largely unknown outside of those affected by them (whereas with the COVID vaccines, we finally crossed the threshold where so many people were injured it simply was at last not possible to sweep everything under rug).
To try to shift this, I decided to focus not on the common side effects of the drugs (which are easy to ignore if you aren’t directly affected by it), but rather the psychotic violence and mass shootings they occasionally cause. A very strong case existed for this, but up to that point, all the supporting literature for it was either in dense books most people were unlikely to read (e.g., Peter Gøtzsche’s Deadly Psychiatry and Organized Denial) or in news articles which only presented slices of the evidence and did so in an excessively sensationalistic manner unlikely to persuade a neutral reader.
My theory, was that since so much effort has gone into politicizing mass shootings and the ensuing arguments over gun control, the right (segments of which already identified with using fewer psychiatric medications than the left) would be very receptive to the fact SSRIs were triggering many of the shootings being blamed on inadequate gun control. Furthermore, my hope was that once this position was adopted, it would spur an interest by its proponents (e.g., political commentators) into finally looking at all the other far more common side effects SSRIs cause and make enough people talk about them that it was finally an acceptable topic of discourse (as previously, much like vaccines, beyond being ridiculed for believing SSRIs were dangerous, you would also be chastised for hurting patients by reducing their access to these “life-saving” medications).
So, I tried to draft a very clear case for this (along with a follow up explaining the dangers of SSRIs and the corruption that allowed them to come to market) and then (at a time when this newsletter was much smaller) put them out immediately following a school shooting which was large enough to become the national media story. That article1,2,3 somehow made it to Tucker Carlson, who then, five weeks later, for the first time in the mainstream media, did a segment on the topic for Fox News:
Following this, as more and more political figures on the right were willing to broach the subject, it became a gradually acceptable topic to discuss (e.g., during his 2024 campaign, RFK Jr. shared a thread on the article I wrote stating: “Any conversation about gun violence is incomplete if it doesn’t touch on mental health and the suppressed evidence implicating SSRIs in suicide and homicide”).
Likewise, the successive attention which bubbled up in the alternative media to the frequent side effects of SSRIs (and Secretary Kennedy’s public acknowledgment of it) has gradually brought mainstream attention to this, including at a recent May 4th panel (covered by the press) which began with victims of SSRIs sharing what they (like many others) have experienced:
Note: Lauren’s story (beginning at 17:00), went viral online due to many being understandably shocked SSRIs could take away your ability to have sex or emotionally connect with your partner.
The panel then concluded with Secretary Kennedy stating we need to do better, that withdrawing from SSRIs is significantly more difficult than withdrawing from heroin, and announcing that the Federal Government would begin combatting this. He laid out a multiagency national effort to do so which will educate health care providers across the country in the dangers of SSRIs (particularly inappropriate prescribing—which is one of the largest issues with SSRIs), provide non-pharmaceutical mental health alternatives, and train providers in how to correctly taper off antidepressants (along with reimbursing them for doing this).
Note: the full panel can be viewed here and here. Additionally, SSRIs are not the only psychiatric with major issues (e.g., last week immediately before this panel I wrote about the many serious issues with benzodiazepines and treating anxiety and at some point I intend to cover the equally problematic antipsychotics).
Despite everything I’ve seen happen over the last four years, I still never believed something like this would happen. For context, in a period when the pharmaceutical industry had much less influence over the FDA, it took more than a decade of activism, leaks and Congressional hearings to simply get a warning label on SSRIs that they could cause suicide. This hence went miles beyond anything even the most optimistic activists had ever imagined could be possible, illustrating why it is so critical to shift the Overton window and make taboo subjects acceptable for regular discussion.
Additionally, it was quite notable that this entire effort goes contrary to the entire foundation of the medical system, as Secretary Kennedy’s ultimate goal was to decrease rather than increase pharmaceutical sales. As such, predictable criticisms of his completely reasonable approach emerged, such as this one from Senator Tina Smith (D-MN):
People I care a whole lot about rely on SSRIs to make their lives work. I don’t know where I would be without SSRIs. RFK Jr. can get his fucking hands and crazy conspiracy theories out of our medicine cabinets”
Protective reactions like these are inevitable, and illustrate precisely why this issue has taken so long to gain traction. But rather than wait for the system to reform itself, my approach has always been to focus on what I can actually offer patients right now.
The Natural Approach to Medicine
Throughout my career, I have tried to prioritize natural therapies, in part because they are often more effective for addressing root causes of illness, but more so, because they simply have less toxicity so you are much less likely to injure people with them. This, essentially, is why, much in the same way I do not critique mediocre drugs I feel provide minimal benefits, I have not focused on many of the same unscrupulous dynamics I've highlighted throughout this article existing within the natural medicine field (e.g., many marginal products are widely pushed simply because they have large profit margins, and a lot of the drama in the health freedom movement over the last few years has ultimately originated from competing parties trying to sink their competitors so they can monopolize sales to this newly created market).
Note: one of the most disillusioning things for me when I entered the natural medicine field was meeting well-known male holistic doctors who rallied against the egregious conduct of the pharmaceutical industry or doctors in general, that then did many of the same things they’d described to their own patients to maximize revenue. From this, I gradually concluded that the more aggressively and audaciously people promoted themselves, the more likely they were to be dishonest.
In my own case, much of my own medical philosophy essentially boils down to:
•Safety is more important than efficacy (so I am very hesitant to use therapies I think have potential risks, and will back off much earlier than others when I see adverse reactions emerge), which in most cases I believe is all-around correct, but simultaneously not appropriate in acute settings (where some degree of harm is often required to save someone’s life).
•If you have to perpetually give someone a therapy, it probably means you are not treating the disease correctly (or only treating the periphery of it), so in those instances (outside of ones where no viable alternative exists such as replacing a critical hormone the body can no longer produce), the focus should always come back to figuring out how to address the underlying illness (which often requires untangling some type of complex connected web in the body or the body, mind, and spirit).
•People frequently develop tolerances or sensitivities to therapies, so if something does work, you only want to use it when it’s clearly needed to avoid being caught in a situation where it doesn’t work when it’s really needed.
As you can imagine, these beliefs aren’t particularly common as they go against the sales focused mindset of the medical industry.
Since I receive many questions on this topic, I’d like to briefly illustrate how these principles intersect with DMSO.
First, many diseases (particularly degenerative neurological ones) essentially follow this progression:
1. Something pathologic is present in the body.
2. It repeatedly injures the body (e.g., the nervous system).
3. Over time, tissue damage (or tissues being stuck in a shocked state) accumulates, and the function of the tissue is gradually compromised.
4. The tissue damage creates functional impairments the individual notices and wants addressed.
Typically, the earlier in that chain you can affect the process, the closer you get to treating the “root cause” of the illness (whereas if you only treat stage 4, which is what many pharmaceutical drugs do—in part due to their design and in part because stage 4 shifts are the easiest to quantify with conventional research), all you accomplish is reducing symptoms and needing to take the drug in perpetuity. Conversely, while treating stage 1 is ideal, it isn’t always possible to do, and in many cases, even if you do, the existing damage is still there.
Since DMSO essentially does a lot of different things many other therapies I routinely use do, but much less potently, it frequently addresses multiple of the above stages without being strong enough to cause a significant reaction, which is essentially why DMSO can frequently fix a wide range of complex illnesses without requiring as much precise targeting by a skilled clinician. Conversely, its ability to do each one varies, with it typically being the least effective at addressing stage 1.
Because of this, for example, we long believed that DMSO could not cure ALS, but as it seemed to help counteract stage 2, it could prevent the progression of the disease, making it a far from ideal option for the disease (but nonetheless still a dramatic improvement over what they could otherwise expect and thus justifiable). I hence was quite surprised to receive reports like this where the reader reported DMSO reversed their ALS (allowing them to regain strength and mobility that had been gone for years) and concluded that the symptoms returning once he stopped DMSO indicated it was addressing stages 2, 3, and 4 for him (discussed further here)
Likewise, when someone else reached out to share their gratitude for me publishing the DMSO series because high oral doses was what finally gave him the ability to walk (due to severe arthritis in one joint on each side), my response was: “if you’ve taken that much DMSO for a year and it has not permanently fixed the issue, you need to look into the root cause, and given what’s going on, I would do either this or this.”
Note: in his case, while I disagreed with perpetually treating the issue with DMSO, it’s also important to acknowledge the only option most people in those circumstances would have is to perpetually take an NSAID, which would be both significantly less effective and expose them to a real risk of a serious complication (prior to the COVID vaccines, NSAIDs were the arguably deadliest pharmaceutical drug in America due to all the gastric bleeds and kidney injuries they cause). So while I would prefer a different approach, compared to the standard options, DMSO management was a miracle.
I mention all of this because one of the most common questions I receive from readers is if they can take DMSO perpetually because of how good it is for you. My answer, in turn, has always been:
“If you can’t trace a clear benefit to taking it (or are at high risk of a condition it prevents), I would not take it perpetually. This is partly because I am philosophically opposed to that approach to medicine, partly because one segment of the DMSO community believes longterm use stresses the liver as the liver detoxifies it (although to the best of my knowledge no data corroborates this—while in contrast liver failure has been cured with DMSO), and partly because in chronic pain, if break days aren’t periodically used, it can lose its effectiveness. That said, there are people who’ve taken it daily for 30 years and reported no issues from doing so, but ultimately the data to solidly answer if this is helpful or harmful will likely never be collected.”
Institutional Inertia
Most societies and institutions follow a similar trajectory: initially, they are the underdogs and have to be as innovative, flexible, and dedicated as possible to establish themselves. However, once they do, their focus shifts to maintaining their newfound position rather than advancing their original mission, and in many cases, this eventually leads to decadence, decay, and collapse (e.g., empires throughout history typically last seven generations because they all succumb to this cycle—a process which is initiated by members of the newly prosperous society collectively shifting their focus from advancing the national interest to finding ways to make as much money as possible for themselves and then once the wealth is accumulated, everyone aimlessly drifting into intellectualism, then decadence and then a societal collapse).
Likewise, whenever an industry or organization becomes assigned to addressing an issue, while bold strides are initially taken, the focus gradually shifts to protecting the institution and maintaining the status quo. For example I’ve never forgotten one clip from a documentary about soldiers who were injured by the (completely unnecessary) experimental anthrax vaccine, which much like the COVID vaccine, ended the careers of many promising soldiers despite widespread resistance against the shots.
Often times you find that people will protect the institution rather than disclose the truth. And as long as the institution stays intact, they’re protected.
Note: a documentary was recently made by CHD exposing the similar (illegal) travesty that happened to our military with the COVID-19 vaccines. I was requested to help promote it so enough people can attend the initial screening for it to make the impact they are hoping for. If this is an issue that is important to you, a trailer for the film and information on purchasing tickets can be found here.
This shift in focus commonly translates to the goal moving from solving the issue to providing an “indispensable service” by perpetually managing rather than fixing it (much in the same way many patients are perpetually treated with medications that cause increasingly severe side effects as they age).
As this process has occurred throughout history, it typically is attributed to financial incentives. For example, despite countless attempts over the decades, government contractors are notorious for overcharging and underdelivering on projects they’re paid to do, with California’s high speed rail being one of the most well known examples (which after more than 30 years of work and 15 billion spent, has only assembled 59 train bridges, not laid any track, and now is estimated will cost 4-7x what was promised when the funding was secured by a 2008 ballot initiative).
Because of this, many believe that spending more money on things (which desperately need help) can actually be counterproductive, as it incentivizes the responsible party to switch their focus to securing funding and planning spending rather than garnering results. Sadly, beyond government spending, this principle encapsulates why it is so difficult to find authentic charities to donate to (both within medicine and outside of it). Likewise, it illustrates why monopolies are so problematic in medicine, as it is only with real competition that the medical system will be motivated to find treatments which actually help their patients.
Note: government contracts pay for results upfront so that money can be saved all around by contractors not needing to secure more costly bank financing. I’ve long believed that if this model were switched (contractors were only paid upon successful completion of the contract), while there might be a small increase in overall costs and exclusion of some smaller contractors, this would be counterbalanced by far greater savings from contracts actually being completed for the original price promised. While nothing this extreme has been done, this week, the military announced unprecedented changes to how defense contracts will be procured1,2 which essentially implements parts of that (along with providing the peripheral support it needs to work), something I am hopeful might for the first time in my life curb America’s immense military spending.
Conclusion
While financial incentives are the most obvious driver for institutions to abandon their original mission, from having repeatedly observed how this plays out inside institutions, I (and many others throughout history) have come to believe that plain human complacency and the widespread aversion to change play an equally central (and perhaps even larger) role. Most people would simply rather master a comfortable routine and get paid for it than face the constant uncertainty required to actually solve difficult problems, and once an organization passes its trying founding phase, its culture naturally selects for those people over genuine problem-solvers who disrupt its order.
What then is the antidote to all of this?
When I was much younger, mirroring what I read in spiritual texts, I saw many instances of people who were or became wealthy being far less happy than their less fortunate peers and realized that money without purpose was not only devoid of meaning, but often spiritual poison as one’s life purpose inevitably would warp to revolve around accumulating ever increasing amounts of money or status (along with all the effort it took to maintain) because they believed the happiness and contentment they could never find could be obtained with even more wealth.
Repeatedly observing this dynamic, I concluded that my purpose would be to learn as much about life as I could, and along that journey, find ways to help others, as while I was not born into a prosperous family, knowing what life was like in many places outside America, I felt immensely fortunate for where I had nonetheless ended up and that I had a spiritual obligation to pay that forward.
Because of this mindset, I would always seek out new and challenging problems to solve, and before long gravitated towards medicine because very few things are as complex as the human body (or as meaningful for others when you can finally figure something out and help heal someone). I was hence quite shocked to discover not only that inquisitive medical students were the minority, but more so, that the entire educational process was structured to gradually remove that mindset from trainees, and just how many of the doctors I trained under both had extremely repetitive practices (which to me would be unbearable) and were less than happy about their life, yet unwilling to consider different ways to manage their patients even when it was clear their approach did not work and a (not too controversial) alternative was offered to them.
I’ve hence long wondered what the solution is to all of this. On one hand, I hold the idealistic perspective that if people are presented with a better way to practice medicine, supported in enacting it, and shown that they can find the passion for medicine they had long ago lost, they would eagerly embrace it (as I’ve seen more physicians than I count in those circumstances do so). Conversely, from watching attempt after attempt to reform the medical system at many different scales fail (and seeing how effectively any entrenched industry will resist change unless a disruptive force emerges and rapidly eliminates the entire sector), I’ve adopted the more cynical perspective that medicine will only change if it faces genuine disruptive competition.
RFK’s approach on mental health hence offers an intriguing third (hybrid) option; provide physicians with a safe, supportive and guided framework to break from the existing mold and practice, while simultaneously rekindling their interest in medicine by seeing the results this previously unconventional approach creates.
It’s hard to describe how much joy this brings me, not only because it offers a better path forward for medicine in general, but also because so many people I was close to have had their lives ruined by SSRIs, and (even at the time I wrote the original mass shooting article), it always felt like there was so much inertia behind the drugs that it would be impossible to ever shift that. I hence want to deeply thank each of you for what you’ve done to create the current unprecedented climate we are in and for your help in supporting this newsletter that has allowed a lot of deeply meaningful things I never thought could happen to happen.
Lastly, I’ve been hard at work over the last two weeks on the second part of the neurology series (spinal injuries, peripheral nerve issues, and how many of DMSO’s therapeutic effects are mediated by the shifts it creates within the liquid crystalline water throughout the body—something you can to some extent see if you look carefully as DMSO mixes with water). I’m presently starting the first draft of the final section (neuropathic pain), so in theory it should be done by Saturday and going forward, most of the remaining ones should be easier to write as the densest topics and mechanisms will now have been covered.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.
Thank you for another great article. De-prescribing psychiatric medication is one of the services I offer in my practice. I’ve been in the medical system for over 20 years and the increase in the use of these drugs is mind blowing. I have seen children as young as 7 on these meds. The most suicidal people I have ever seen, were recently placed in these meds and prior to starting them, they were just depressed or anxious. It’s scary because it’s so expected to Rx these drugs that if you do not, you could be held liable for not following guideline. When I was applying for NP jobs, one of the questions I was asked during an interview for an urgent care was would I be willing to rx a ssri for a person who was depressed. My face couldn’t hide the disgust at that question I think. I didn’t get that job.
Two actions are required to stop the cycle of over prescribing prescription drugs. Fraudulent medical research that manipulates statistics to hide the harm that the drug causes should be a criminal offense and prosecuted under criminal law. Second, most of the drugs with side effects, especially those that have blackbox warnings should be banned from the marketplace immediately.. I suspect 80% of all the prescription drugs would disappear and would crush big Pharma. They have been crushing the health of the American people long enough.