How DMSO Protects and Heals the Internal Organs
The evidence behind DMSO's utility for a myriad of challenging diseases

Story at a Glance:
•The therapeutic actions of DMSO make it well suited to treat challenging conditions throughout the body, including many of the internal organs.
•In this article, we will examine how DMSO protects organs from injury (e.g., poisoning or blood loss) and some of the specific diseases DMSO has been proven to treat.
•These include: heart attacks, liver cirrhosis, gallstones, ARDS, lung damage from inhaling smoke, pulmonary fibrosis, pancreatitis, diabetes, nephritis, kidney stones, polycystic kidney disease, cystitis, epididymitis, genital pain, prostatitis, urethral syndrome, enlarged prostates, tubal infertility, endometrial inflammation, and fibrosis.
•This article will review DMSO treatment protocols for those conditions (along with non-DMSO approaches we utilize for them) and provide general DMSO information for those looking to use DMSO for their own health.
Note: I am currently in the process of updating this article with the applicable data from the roughly 100,000 DMSO studies I collected from October to April. Currently the male genitourinary (sexual health) section has been updated but the rest has not.
Dimethyl sulfoxide (DMSO) is a remarkably safe compound that can treat a variety of challenging conditions. Since DMSO is remarkably effective for treating chronic pain, arthritis, and injuries like sprains or burns (discussed further here), it quickly spread across America as a miracle drug. Thousands of studies were conducted to confirm its value, and before long, hundreds of thousands of people considered it to be the most important therapeutic ever discovered.
Unfortunately, due to various negative political factors, the FDA went from embracing DMSO to going to war against it, and eventually, the pharmaceutical industry reluctantly followed suit. Sadder still, the FDA refused to relent even once:
•DMSO was shown to effectively treat strokes, traumatic brain injuries, spinal cord injuries, and many circulatory disorders (discussed here).
•DMSO was shown to cure a variety of “incurable” autoimmune and connective tissue disorders (discussed here).
•DMSO was shown to treat a variety of challenging (and often incurable) eye, ear, sinus, and dental conditions such as tinnitus and blindness (discussed here).
Since publishing those articles, I’ve received roughly a thousand reports from people of the remarkable effects DMSO has had on them (which can be read here), which while unbelievable, are almost identical to what people experienced in the 1960s before the FDA erased DMSO from the public’s memory.
Likewise, I’ve received almost as many questions (which is why I am trying to make these articles as thorough as possible). One of the most common questions I’ve received is if DMSO can help with various disorders of the internal organs.
How DMSO Heals the Organs
As highlighted in the first part of the series, DMSO is able to protect tissues from otherwise lethal stressors (e.g., cold, radiation, heat or having their blood supply cut off for a prolonged period). While some of these could potentially be explained by DMSO restoring a compromised a blood supply, or its ability to protect against the ischemia-reperfusion injuries that follow a lost blood supply being restored (something which has been demonstrated in many different organs), that alone is not sufficient to explain what transpires. As such, it’s important to review two other critical properties of DMSO.
Shocked Cells
Frequently when cells receive a potentially lethal stressor, they will shut down their normal functions to survive and repair themselves. In many cases, this process is essential for survival, but in some cases, it instead becomes the root cause of disease because cells get stuck within the non-functioning state (a pathologic Cell Danger Response) or transition from being non-functional to dead (with these “penumbras” that later die being extremely common after strokes).

There are a few key points about this model:
•In many cases, due to past injuries, tissues will have certain cells stuck in the cell danger response, resulting in their functionality being greatly diminished.
•Typically, more potent stressors make it progress faster (e.g., strokes rapidly kill brain cells). In contrast, weaker and more chronic stressors make it progress slower (e.g., I previously discussed how the cell danger response underlies many “inexplicable” chronic diseases).
•The further down this progression a tissue is, the harder it is to reverse (but with the correct therapy it can almost always be done).
•Many regenerative therapies essentially work by getting “shocked” cells to come back to life and start working again, which in many cases is critical for overall health since those tissues not working can disrupt the entire body.
•DMSO can reverse this process (discussed further in the first part of this series), but it is typically more helpful for the rapidly progressing instances coming from a significant stressor (e.g., a stroke or a severe injury or ingesting a poison). This in turn, explains why DMSO can sometimes give motor function back to people who were paralyzed by strokes years ago, but it is dramatically more effective if given shortly after a stroke, traumatic head impact or spinal cord injury, and likewise why individuals on DMSO suddenly “notice” things in their body that had stopped working come back.
Note: caspase proteins play a central role in programmed cell death. DMSO, in turn, has been shown to protect heart, liver, and airway cells from caspase proteins.
•For slower and more chronic versions of this process which have already progressed, one typically needs a systemic regenerative therapy (discussed further here).
Stem Cell Differentiation
Initially, human cells have the potential to become any human cell, but as time goes on, their range of possibilities becomes more restricted until they settle on the cell type they are supposed to be in each part of the body (a process known as differentiation). Because of this they can be extremely useful in healing injuries or repairing damaged tissue because the stem cells can differentiate into the missing cells and then replace the ones that were lost (allowing the organ to regain function).
Conversely in cancer the reverse happens, and with cancer cells being much less differentiated than typical cells and hence less able function in harmony with the body. DMSO, in turn, belongs to a narrow set of agents which cause cells to differentiate (e.g., causing cancer cells to become benign heart cells), which is how it able to cure a wide ranger of cancers.
Likewise, since DMSO is a potent differentiation agent, it is frequently used in stem cell research to induce their differentiation into target cell types—which often requires DMSO in conjunction with an agent that already occurs in the tissue (as stem cells need something to guide them into transforming into the cell type each tissue needs). As so many paper have explored and validated this concept, rather than cite each of them, I’ll use an AI generate table to summarize some of the cell types DMSO has been observed to trigger differentiation in:
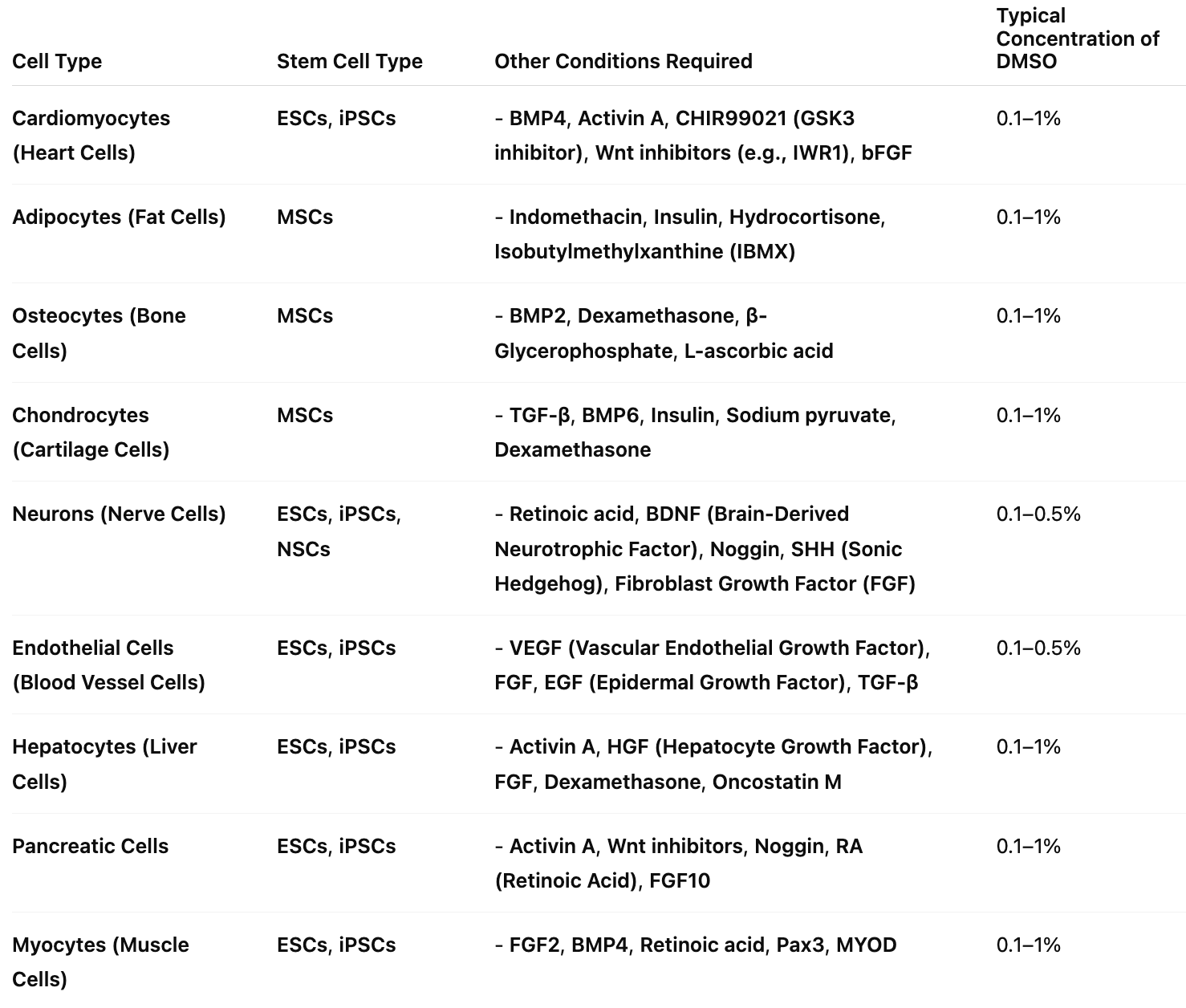
Note: many of these cofactors (e.g., BDNF) are present within the tissues and provide signals to the cells to differentiate into. Likewise, many organ specific peptide products also signal stem cells to differentiate into that tissue, and in some cases have been observed to differentiate synergistically with DMSO.
In turn, I believe that a key reason why DMSO is able to regenerate organs is because it induces stem cells already within the body (e.g., bone marrow MSCs) to differentiate into the missing tissue and hence repair the damaged organ.
Note: the clinicians I know who get the best results with peptide therapies use organ specific peptides concurrently. However, I am not familiar with anyone who has combined all three (excluding those who use DMSO preserved stem cells).
Let’s now look at what DMSO does for each organ.
Heart
Like the brain, if the heart’s blood supply is cut off (e.g., during a heart attack), heart cells rapidly die. DMSO has been repeatedly shown to prevent this.
In a 2012 study, rat hearts had their blood supply cut off for 30 minutes and then were reperfused for 120 minutes. DMSO being given beforehand was found to preserve coronary blood flow and reduce the resulting tissue necrosis (death) by 57.6% and left ventricular dysfunction, particularly if it was given for a few days beforehand, rather than just immediately preceding the blood supply being cut off.
Similar results in rats and pigs were reported in 2015, 2010, in 2001, in 1987, and in 1982, when a heart attack was simulated (e.g., one study found DMSO reduced the damaged portion of the heart by 76.18%, another found it significantly reduced intramyocardial hemorrhage and gross pathological changes and a third found it prevented contracture bands from forming in heart tissue). Additionally, a rabbit study found that if hydrogen peroxide (H₂O₂) was given concurrently with DMSO immediately after cutting off the blood supply to the heart, the damage the heart experienced was further reduced, presumably due to H₂O₂ providing oxygen to the heart tissue.
Numerous studies also show DMSO preserve heart function during this time (e.g., cardiac output and brain perfusion in dogs, heart contractile strength in rabbits or mitochondrial function in rabbits). Likewise, when a common cellular enzyme which typically breaks down ATP (extracted from cow hearts) was mixed with DMSO, it instead synthesized ATP, suggesting DMSO is able to create a unique cellular environment which facilitates the creation of energy (particularly when the normal conditions cells rely upon for energy generation are not present).
DMSO has also been shown to protect the heart from other stressors which cause comparable damage to the heart’s blood supply being cut off (e.g., reperfusion injuries from calcium ion containing solutions, endotoxin-induced myocardial injury, IV potassium at the same dose used for lethal injections, toxic doses of H₂O₂ and isoproterenol-induced heart attacks,1,2,3,4.5) with improvements such as reduced oxidative stress, tissue necrosis, ventricular aneurisms, ventricular ruptures, and subsequent myocardial fibrosis frequently being reported.
Note: DMSO also protected older rat hearts from the stress caused by prolonged immobility and from dietary copper deficiencies.
•One mechanism to explain the damage that occurs in heart cells after a shock or stressful conditions (e.g., heart failure) is that the t-tubules within the heart cells will seal and remodel. In one study, 1% DMSO (but not 10% DMSO) was found to prevent this from occurring and this process was hence hypothesized to at least in part explain DMSO’s ability to protect heart cells from significant stressors.
Additionally:
•In patients who survive heart attacks (and are brought back to life) they frequently have a variety of complications. In one study of 42 severely ill patients who had septic complications of postresuscitation disease, IV DMSO was an effective therapy, even in cases where sepsis came from antibiotic resistant bacteria.
•A key component of regenerative medicine is using stem cells (which have the potential to differentiate into many different cells) to replace damaged tissues (particularly those within critical organs). DMSO (especially with another medication) was shown to cause stem cells to differentiate into heart cells.
•When heart cells were exposed to low concentrations of DMSO (less than 0.5%), their respiratory control ratio and cellular viability relative to the control cells were enhanced (whereas at 3.7%, DMSO became harmful to them).
•DMSO can also increase or decrease the force of heart contractions and membrane potential1,2,3(e.g., a 70 mM DMSO concentration or less has a positive inotropic effect, while a higher one can do the opposite or create a mild hyperpolarization that prolongs the action potential) in a manner independent of beta-adrenergic receptors, and does not alter cardiac rhythm. Conversely, DMSO also increases parasympathetic function (through inhibiting acetylcholine esterase), in one study being found to have no effect alone but to potentiate acetylcholine slowing the heart rate and in another study, to cause a dose dependent relaxation of thoracic aorta (blood vessel) strips precontracted with phenylephrine or KCl, indicating DMSO can significantly facilitate vasodilation.
When stem cells are mixed with DMSO alone (rather than including another differentiating agent), the cells are most typically reported to differentiate into heart tissue.1,2,3,4,5,6,7,8,9 (including in MSCs1,2,3)—suggesting DMSO has significant value in heart stem cell protocols. Additionally certain agents, such as oxytocin (the bonding hormone) potentiate DMSO’s ability to differentiate stem cells into heart cells, as do proteins present in cancer cells (which have been shown to boost the regeneration of new heart muscle).
Stomach
DMSO has been repeatedly shown to heal the stomach and modulate its function, particularly when injuries follow excess acidity:
•A study of 138 patients with duodenal ulcers (mostly in remission), one gastric ulcer, or chronic gastritis found that 50% DMSO applications to the epigastric area often reduced gastric juice volume and acidity in those with duodenal ulcers and hypersecretion, and enhanced antral mucosa neutralization in some with acidic conditions. In chronic gastritis with preserved secretion, DMSO effects varied (no change, reduced, or slightly increased secretion/acidity). In secretory insufficiency, DMSO had no stimulating effect, either unchanged or slightly reduced secretion. In short, DMSO generally normalized hypersecretion.
•In lab tests, 9% DMSO increased pepsin enzyme activity by 83.4%, lowered the Km value to 1.50 mg/mL, and altered pepsin’s molecular conformation without inhibiting aromatic amino acid absorption—hence making pepsin more effective at digesting protein.
•In 115 hospitalized patients with pelvic fractures or hypovolemic shock at risk for stress-induced gastric ulcers, 22% of 58 controls developed ulcers, compared to only 4% of 57 receiving DMSO and 3% of 62 receiving allopurinol. Notably, none of the DMSO-treated patients deteriorated or required emergency surgery, whereas 8 controls and 1 allopurinol recipient did, with 3 control patients dying.
•In 101 patients with hematemesis (coughing up blood) due to erosive gastritis, oral DMSO and allopurinol (administered every 6 hours for 5 days) resulted in 8% having further hematemesis episodes, and 9% having endoscopies showing hemorrhagic inflammation, whereas in contrast 29% of untreated controls had further hematemesis episodes, and 44% showed hemorrhagic inflammation. No treated patients required surgery, while three controls did, with one death.
•In 58 patients with NSAID-induced erosive gastritis, DMSO reduced re-bleeding, stabilized hemodynamics, and promoted gastric erosion healing (7% had erosions at 48 hours) compared to placebo (50% of 59 patients), with fewer patients requiring transfusions or surgery.
•In 40 patients with multiple fractures and hemorrhagic shock, DMSO reduced stress-induced acute gastric mucosal injury incidence to 2.5% (1/40) compared to 23.8% (10/42) with placebo, with fewer requiring surgery.
•In rats with corrosive esophageal burns, intraperitoneal DMSO reduced stricture formation by decreasing malondialdehyde, nitric oxide, tumor necrosis factor-alpha, and interleukin-6 levels, lowering the stenosis index and histopathologic damage scores compared to controls.
•In rats, DMSO significantly accelerated healing of reserpine- and 5-hydroxytryptamine-induced acute ischemic gastric mucosal injury, reducing injury severity over 4 days compared to placebo.
•In rats, DMSO (1%, 2%, or 5%) reduced reserpine and serotonin induced ischemic gastric mucosal injury after 2 days of pretreatment, with 1% reducing injury area, 2% protecting 60% (reserpine) and 80% (serotonin) of rats, and 5% preventing injury entirely, compared to placebo, without altering H+ output.
•In rats, DMSO (1%, 2%, or 5%) reduced ethanol-induced gastric mucosal injury after 24 hours (2% and 5% solutions) and 48 hours (1% reduced injury in 70% of rats, 2% and 5% eliminated injury entirely), with healing confirmed by regeneration, compared to placebo.
•In rats, DMSO (1%, 2%, or 5% solutions) reduced reserpine-induced chronic gastric ulceration after 4 weeks, with 1% reducing ulceration incidence to 60%, 2% to 20%, and 5% providing complete protection, compared to 100% in placebo, without altering H+ output.
•DMSO (2 or 5% solutions) completely protected rats against aspirin-induced gastric mucosal injury (0% incidence vs. 30% without pyloric ligation and 80% with ligation in placebo) and ethanol-induced injury (0% incidence vs. 100% in placebo), without affecting H+ output.
•In rats subjected to water-immersion stress, DMSO inhibited gastric ulcer formation. Similarly, in rats with cold-restraint stress, DMSO, allopurinol, or their combination significantly reduced lipid peroxidation and stress-induced gastric and lung injuries compared to saline controls.
Note: other studies have also shown DMSO protects against gastric stress ulceration.
Other data also corroborates DMSO’s ability to heal severe gastric conditions and support recovery in challenging cases:
•A 1968 patent application reported oral DMSO effectively treated gastrointestinal conditions: 28 patients with acute gastritis resumed work within 5–8 days, free of nausea, vomiting, and pain, with 21 remaining symptom-free after one year; 13 patients with chronic gastritis improved after 1–2 months and stayed relapse-free for a year with periodic retreatment; 5 patients with recent peptic ulcers were cured without recurrence over a year; 6 patients with enterocolitis improved after 8 days and returned to work within 2 months; and 3 patients with mucomembranous colitis were cured after 3 weeks.
•In patients with refractory gastric and duodenal ulcers unresponsive to three months of cimetidine and one month of bismuth chelate, oral DMSO achieved complete healing within four weeks with no significant side effects, compared to placebo.
•In 126 patients with healed duodenal ulcers and Helicobacter pylori infection, oral DMSO reduced one-year ulcer relapse to 6%, compared to 47% with placebo and 24% with cimetidine, showing superior efficacy. No comparison between DMSO alone and DMSO with allopurinol was reported.
•In 12 patients with refractory peptic ulcers (eight duodenal, four gastric), oral DMSO achieved complete healing within four weeks, compared to placebo.
Likewise, in a feline case of viral enteritis (likely from panleukopenia), DMSO created a clinical improvement, again indicating protective effects on gastric and intestinal lining.1,2
Finally, DMSO has also been shown to alter other characteristics of the stomach (e.g., it made the stomach more transparent, increasing light transmittance by 29%, it increased the stomach’s sensitivity to vagal stimulation, and above a 50% concentration, it decreased stomach acid secretion in a dose dependent manner).
Note: Numerous key human studies cited in this section and the next (where DMSO was often administered orally with a nasogastric tube) were conducted by a DMSO researcher in Iraq between 1990–1994, during a period when its medical system was robust before economic sanctions and conflicts disrupted healthcare infrastructure, a pattern also observed in Libya post-NATO intervention.
Intestines
Numerous studies have explored DMSO’s interactions with the small and large intestines. For example, autoradiography in mice showed that radiolabeled DMSO selectively accumulates in the large intestinal mucosa, which may help explain its notable effectiveness in treating bowel inflammation. Additionally:
•Despite being an acetylcholinesterase inhibitor (and hence parasympathetic activator), DMSO (0.2-1.4%) contacting the intestines does not promote peristalsis (which is fortunate as otherwise diarrhea would be a frequent side effect of oral DMSO use). Conversely, another study (of pig intestines) found it was nonspecific antagonist of carbachol, histamine, and nicotine on isolated guinea pig ileum (all of trigger peristalsis).
•DMSO at low concentration (e.g., between 0.16%-5%) typically did not affect intestinal permeability or the gut absorption of other substances.1,2,3,4 However, in certain circumstances it did (e.g., if high amounts of glucose or galactose were present DMSO increased their absorption by allowing them to directly diffuse through the intestines and at DMSO concentrations above 0.3M it reduced intestinal absorption of amino acids with completion seen at 1M).
Note: assuming a DMSO mixture gets diluted by 50% once it is mixed with the stomach and intestinal fluids, the typically recommend oral dose results in an intestinal DMSO concentration roughly half the 0.3M threshold identified in that study (although I suspect it’s actually lower since of the DMSO will diffuse directly into the body as it travels through the digestive tract).
DMSO’s protective properties shield the bowels from a variety of serious injuries. For example, cutting off the blood supply to the small intestine will rapidly cause the tissue there to die and often rupture (leading to fatal peritonitis). DMSO has been repeatedly shown to prevent this:
•In rats, giving IV DMSO to rats after 30-60 minutes of their entire intestinal blood supply being cut off (or 150 minutes of one section’s blood supply being cut off), resulted in 28 out of 29 not developing gangrene, and within 24 hours, there was no evidence of ischemic damage to the intestines. Similar results were obtained in a 1985 study (which also noted significantly reduced inflammation and adhesions) and a 2016 study which showed greater tissue protection with higher DMSO doses (along wit hit stabilizing blood pressure and improving metabolic status)..
•In horses, DMSO has been shown to prevent intestinal ischemia-reperfusion injuries (particularly within the jejunum or ascending colon) and to reduce intestinal microvascular permeability, edema, inflammation and bowel to bowel adhesions.1,2,3,4,5,6
•Similar results have also been seen in other animals such as dogs or calves (e.g., one study found DMSO significantly improved pH, PCO₂, PO₂, O₂ saturation, and peritoneal fluid lactic acid levels).1,2,3,4
Additionally:
•In rats, oral DMSO (1%, 5%, or 10% solutions) provided dose-dependent protection against acute and chronic duodenal ulceration, reducing incidence to 80%, 30%, and 30% (acute) and 40%, 20%, and 20% (chronic) compared to 100% in placebo groups, without altering hyperchlorhydria (stomach acid levels.
•In rats, DMSO and allopurinol reduced acute duodenal ulceration incidence to 70% at 2 days, 30% at 5 days, and 0% at 7 days (vs. 100%, 80%, and 50% with placebo) and chronic duodenal ulceration to 80% at 5 days, 30% at 10 days, and 10% at 15 days (vs. 100%, 90%, and 80% with placebo) without altering hyperchlorhydra.
•DMSO has been observed to reduce intestinal cell death in jaundiced rats (following bile duct ligation).
DMSO’s protective properties has also been shown to protect the intestines from other lethal stressors:
•In rats with 20% third-degree burns, compared to placebo, DMSO solution applied to the mesentery reduced white blood cell adhesion in microveins, improved microcirculation and preserving immune-active white cells.
Note: blood sludging is a common consequence of severe burns that likely triggers many of the systemic complications they create.
•In dogs, oral DMSO improved survival by 75% against 12.5 Gy (a lethal dose) of abdominal radiation and prevented radiation-induced intestinal damage.
•In mice exposed to lethal radiation doses (9.0–9.5 Gy doses), oral DMSO given 15 minutes to 4 hours before irradiation achieved 100% survival along with, increased bone marrow and intestinal stem cell regeneration, reduced blood cell loss and intestinal damage, and extended survival up to 500 days by alleviating radiation-induced injuries to lungs, kidneys, liver, and heart.
Note: this review paper discussed DMSO’s use in preventing nuclear radiation damage to organs and tissues.
•DMSO (a widely used cryopreservant) has been shown to protect intestinal segments in dogs from necrosis following cryoinjury (dying after being frozen).
In addition to protecting intestinal tissue from injury, DMSO has also been shown to heal them:
•A study randomized 302 consecutive patients with previous symptomatic duodenal ulceration that was shown to have healed, and who were smokers and social drinkers, to receive four different treatments. Of the 220 available for evaluation, 65% who received a placebo had a recurrence of the ulcer, 30% of those who received cimetidine, 12% of those who received allopurinol, and 13% of those who received oral DMSO.
•Another author reported on a doctor who had 5 patients with recurrent duodenal ulcers and were social drinkers he gave DMSO to. They were examined once a month for a year, and all 5 had no recurrence of ulcer symptoms (along with having better health than expected and excellent attendance at work). He also highlighted the case of a 55 year old woman with severe digestive tract issues (e.g., internal bleeding leading to her being anemic with a hemoglobin of 5.0), weakness, fainting and shortness of breath. After receiving an emergent blood transfusion and being diagnosed with angiodysplasia in her GI tract, she was started on IV iron (which is not pleasant and did not help her causing her to progress to being terminal). She was then started on injected DMSO and B-12, recovered, and over the six years of follow-up, did not require any subsequent blood transfusions.
•In a patient with refractory duodenal ulceration unresponsive to three months of cimetidine and one month of bismuth chelate, oral DMSO achieved complete ulcer healing within four weeks, compared to no improvement with placebo
Note: this type of chronic internal bleeding is quite challenging to treat (e.g., the only other approach I know of that consistently helps here is a Chinese herbal formula).
•A randomized double-blind study of 363 consecutive patients whose duodenal ulcers that did not heal despite 3 months of treatment with cimetidine (and who were cigarette smokers or social drinkers), were given either cimetidine twice a day alone or with DMSO or allopurinol. In 315 patients who were evaluable for analysis, at 8 weeks, 60% of those who had cimetidine recovered, whereas 100% of those who received DMSO or allopurinol recovered. Additionally, the one year relapse rate was 29% for cimetidine alone, 8% for those who took allopurinol, and 7% in those who took DMSO.
Note: another study used DMSO in combination with electrophoresis (to direct DMSO to the ulcer) to treat peptic and duodenal ulcers.
•A randomized double-blind study took 238 patients with symptomatic acute duodenal ulceration who were smokers and social drinkers were randomized to receive for 8 weeks cimetidine or 8 weeks of a half dose of cimetidine plus oral DMSO (400mg two times a day) or allopurinol. After 8 weeks, 69 of the 87 (79%) who only received cimetidine recovered, whereas 100% of the 85 who received DMSO did. Additionally, 67% of those who received cimetidine over the next year relapsed, compared to 6% of those who also took DMSO.1,2
•In rats where part of the colon had been removed (requiring each remaining end to be joined together), a DMSO quercetin mixture given intraperitoneally post surgery significantly improved healing (e.g., bursting pressure along with hydroxyproline, malondialdehyde, superoxide dismutase and catalyze levels had a 1.4-3.9 fold improvement).
Note: many studies show DMSO significantly improves healing from surgery and heals chronic wounds.
•A Russian suppository containing (50%) DMSO and hyaluronic acid (along with vitamin C, collagen, and coenzyme Q10) was developed to treat rectal fissures.
Note: the gastrointestinal tract appears to be more sensitive to DMSO than most parts of the body and in some of the studies I reviewed, DMSO could injure its gastrointestinal lining. As injuries like those suggested by the studies are never reported in practice, I believe those results were due to significantly higher concentrations of DMSO contacting the gastrointestinal lining than are seen following typical oral consumption (much in the same way, as mentioned above, DMSO can inhibit the absorption of amino acids, but in practice parents around the world have found the combination of two is profoundly transformation for developmental delays and Down Syndrome). In my eyes, all of this strongly argues for avoiding higher oral DMSO doses than those widely used by the DMSO community.
DMSO’s anti-inflammatory properties (and histamine receptor antagonism) have also been repeatedly shown to treat inflammatory bowel diseases:
•A double-blind, randomized study evaluated patients with recurrent attacks of proctosigmoidal ulcerative colitis that were not being prevented by their prophylactic medical regimen, three different combinations of standard therapies, or a standard therapy with DMSO (46) or allopurinol (45). After two weeks, 51% recovered from a standard regimen (sulfasalazine or prednisolone), while 84% of those using DMSO or allopurinol recovered. Over the next year, those treatments were continued and it was observed that the standard treatment (sulfasalazine) had a 25% relapse rate, whereas that rate was only 5% of those taking DMSO or allopurinol.
•In mice with encapsulating peritoneal sclerosis (EPS), a severe complication of peritoneal dialysis which leads to intestinal obstruction with or without peritonitis, DMSO treatment reduced parietal and visceral peritoneum thickening by 30% compared to controls. It also decreased CD4, CD8, and IFN-γ-producing T cells and Ascites cytokines (IFN-γ, IL-17a, TNF-α, IL-23) while increasing IL-4, IL-10, CD69 T cells, and Treg cell differentiation—all of which reduces inflammation. Finally, these results were corroborated by using DMSO to differentiate Treg cells in a test tube and once those cells were implanted in mice, they also prevented EPS.
Note: DMSO has also been used to treat ascites in hamsters with melanoma.
•Amyloidosis (the deposition of irregular proteins which clump together) is frequently seen alongside autoimmune disorders. As DMSO stabilizes and solubilizes proteins, it effectively treats amyloidosis, and due to the lack of effective treatments for amyloidosis, many studies have conducted demonstrated DMSO’s utility for amyloidosis (listed here). These include cases where amyloid deposition had been causing severe gastrointestinal issue which fully resolved following DMSO,1,2,3 including cases which would have otherwise been fatal.
•In one report, daily oral DMSO successfully treated 10 out of 15 patients with AA amyloidosis linked to autoimmune disease; notably, all 4 cases related to Crohn’s disease achieved full remission. Among the 6 patients presenting with gastrointestinal symptoms, all experienced resolution of diarrhea and protein-losing gastroenteropathy—with no serious adverse effects reported.
Note: in another report, a 1.2 by 1.2 cm and a 1.0 by 1.2 com gastric lesion from localized amyloidosis completely resolved following oral DMSO taken three times a day.
•Intraperitoneal injections of zymosan trigger are used to trigger systemic inflammation akin to sepsis. In two separate rat studies, compared to placebo, DMSO was shown to reduce inflammation, preserve intestinal blood flow and prevent damage to the gut and intestinal lining (a major issue in both chronic and subtle inflammatory bowel disorders).1,2
•In a third similar study, subcutaneous DMSO given one hour after zymosan increased 24-hour survival from 55% to 90%, reduced liver, kidney, and intestinal swelling by 10-20%, lowered inflammatory markers (TNF-α, IL-6) by 20-30%, and improved organ blood flow and tissue damage
Likewise, in numerous animals, intraperitoneal DMSO has also been repeatedly found to improve peritonitis, including purulent or diffused cases,1,2,3,4,5,6,7As DMSO potentiates antibiotics, some of those studies used a combination (e.g., DMSO and kanamycin) to successfully treat peritonitis,1,2 while others found DMSO altered abdominal antibiotic absorption, caused antibiotics to concentrate in the peritoneum and increased bacterial sensitivity to them.1,2,3
Note: with standard hospital care, peritonitis kills 13.16% for patients under 50 years and 33.33% of patients over 50 years—making the improvements seen with DMSO quite profound.
Finally, DMSO has also been combined with antibiotics to treat abdominal abscesses, and at concentrations comparable to those oral DMSO will reach in the intestine, inhibit the growth of many common gastrointestinal pathogens (e.g., Escherichia coli, Shigella dysenteriae, Candida albicans).1,2
Liver and Gallbladder
DMSO has also shown great promise for protecting the liver and addressing issues with the biliary (bile) tract
Liver Injury and Protection:
•In rats exposed to chloroform or bromobenzene, DMSO administered 24 hours post-exposure was found by multiple studies to significantly reduce plasma ALT levels, limited centrilobular liver lesions, restore sinusoidal perfusion, reduce leukocyte adhesion and modified Kupffer cell phagocytic activity (mitigating the hepatic inflammatory response), and prevent chloroform-induced kidney necrosis. Delaying treatment beyond 24 hours led to a loss of protection, with progression to bridging necrosis and elevated ALT, emphasizing DMSO’s dose- and time-sensitive hepatoprotective effects.1,2,3,4
•In F344 rats subjected to warm ischemia as non-heart-beating donors, DMSO (2–6 ml/kg, ip) preserved liver and kidney viability, maintaining potassium and LDH levels comparable to non-ischemic controls.
•A study found giving DMSO to rats 10 hours after they were exposed to halothane (an inhaled anesthetic that was phased out of the richer nations due to its toxicity profile), chloroform, or bromobenzene and was found to prevent liver and kidney damage these toxicants typically cause. A followup study instead gave DMSO 24 hours later found DMSO reduced the resulting liver damage 4-fold (which without treatment within 48 hours would have occupied 40-50% of the liver) and ALT levels 8-16 fold.
Note: this study also found DMS (a DMSO metabolite) offered no protective effects.
•In rats exposed to thioacetamide, DMSO reduced liver and brain oxidative stress, lowered liver enzymes (AST, ALT, LDH), decreased hyperammonemia, and increased BUN levels, mitigating lipid peroxidation and preserving glutathione and catalase activity. Similar results were found in another study.
•In rats, daily oral DMSO for 4 weeks was seen to prevent dimethylnitrosamine induced liver damage without any major side effects. Specifically, it prevented body and liver weight loss and the induction of hepatic fibrosis and the expression of mRNA for type-1 collagen in the liver. Additionally, DMSO was also found to inhibit LPS induced TNF-alpha and nitric oxide production (e.g., TNF-alpha mRNA levels were reduced).
•In rabbits subjected to portal vein or hepatic artery clamping, DMSO, in a dose-dependent manner has been repeatedly found to reduce ischemic and ischemia-reperfusion liver damage and oxidative stress.1,2,3,4,5,6,7
•A Brazilian study found that DMSO reduced the oxidative stress that followed part of the liver being surgically removed.
•In primary cultured rat hepatocytes exposed to Tylenol, DMSO reduced toxicity by preserving plasma membrane integrity, restoring glutathione to ~63% of normal levels, and preventing cytosolic free calcium elevation. A second also found DMSO prevented this liver damage, while a third also found DMSO prevented liver damage, but in the presence of natural killers, could instead increase it.
•DMSO administered to Syrian golden hamsters reduced the incidence and severity of acetaminophen-induced hepatocellular injury, attenuating increases in serum glutamic-pyruvic transaminase and alkaline phosphatase activities, indicating a protective effect against liver toxicity potentially through a free radical-mediated mechanism.
•A rat study found DMSO inhibited liver necrosis and oxidative stress triggered by injecting D-Galactosamine and restored liver vitamin C levels.
•In galactosamine-sensitized mice, DMSO (10 mL/kg) inhibited endotoxin-induced hepatic NF-κB activation, reduced plasma TNF-α by 86%, suppressed ICAM-1 mRNA, decreased neutrophil accumulation by 79%, and reduced liver injury by 80%.
•In rats exposed to carbon monoxide, DMSO reduced brain and cardiac ischemic injury, lowering cerebral neuronal alteration, degenerative neuron rates, and cardiac injury scores after one day. Combined with ethyl pyruvate, DMSO reduced hepatic injury scores and further reduced cardiac.
•DMSO was shown to protect liver, heart, and airway cells by inhibiting caspase proteins (reducing cell death).
•DMSO was found to inhibit the NF-kappa B activation, ICAM-1 gene transcription and TNF-α formation which following endotoxin exposure, thereby preventing liver injury.1,2
•A rat study found DMSO inhibited lipid peroxidation in hepatocytes triggered by carbon tetrachloride and improved the antioxidant system’s state. Likewise, a rabbit study found that DMSO and tocopherol prevented the liver damage caused by injecting carbon tetrachloride. Finally, a third liver study found DMO and alpha-tocopherol counteracted the oxidative damage caused by chemical injury.
•In primary cultured rat hepatocytes, 2% DMSO with collagen-coated dishes extended cell survival to 96 hours (vs. 48 hours for controls), maintained 86% cell viability at 96 hours and 78% at 120 hours, preserved cell shape, doubled glycogen content, and retained 50–60% cytochrome P450 content.
•DMSO was repeatedly shown to cause mesenchymal stem cells to differentiate into liver cells, potentially explaining how DMSO is able to regenerate the liver.1,2
•In isolated rat hepatocytes, DMSO and 2% and 8% DMSO caused a biphasic inhibition of sympathetic stimulation of liver cells. Likewise, DMSO was observed to permeate isolated rat hepatocytes, but for it to become less able to at higher concentrations.
•In primary cultured rat hepatocytes, DMSO with collagen-coated dishes extended cell survival, maintained high cell viability, preserved cell shape, doubled glycogen content, and retained cytochrome P450 content
•In Chang liver cells, 0.1% DMSO increased CYP3A4 mRNA and protein expression, while 0.01%–0.05% DMSO increased CYP3A4 protein only; combined with testosterone or rifampicin, DMSO enhanced CYP3A4 and CYP2C9 protein expression.
Liver Failure
•This author reported on a study with 12 patients who had terminal liver cirrhosis who agreed to stop drinking all alcohol for the duration of the program were put on daily oral DMSO and aloe vera. Of the 8 who chose to continue the program for 6 months, all had improved health, significantly reduced vomiting, and improved liver function tests, and rather than all being dead within one year as expected, they were in better condition than they had been at the start of the study.
Note: if using DMSO for cirrhosis, it is critical to stop consuming alcohol, as DMSO can slow the metabolism of alcohol.
Gallbladder and Biliary System
• A rat study created obstructive jaundice by ligating the common bile ducts and found that DMSO mitigated pathologic effects (e.g., normalized laboratory values). Another rat study found DMSO protected intestinal cells from dying after bile duct ligation.1,2
•Injecting 90% DMSO mixed with 5% hexametaphosphate into the biliary tract was found to effectively dissolved gallstones within the liver and be safe for patients.
•In rabbits, D-limonene (from citrus peels) synergistically combined with DMSO to dissolve implanted human gallstone.
•MTBE is sometimes infused into the gallbladder to dissolve cholesterol gallstones (comprising 80-90% of gallstones) but cannot dissolve the rarer pigment (bilirubin) gallstones. A series of Chinese studies demonstrated that once dissolved in DMSO, MTBE can (e.g., outside the body it dissolved 79.12% of the stones within 48 hours significantly outperforming other agents, and likewise in dogs, 76.83% of their stones were dissolved after 63 hours). Finally, a third formulation that also included cyclohexane diamine tetraacetic acid showed an even greater ability to dissolve these gallstones.1,2,3,4
Note: these studies repeatedly emphasized these formulations were safe and showed no toxicity. I am skeptical of this, as MTBE alone is quite toxic (e.g., due to side effects, it was largely withdrawn from medical use about 10 years ago), and it is quite possible combining it with DMSO would increase rather than neutralize its toxicity.
•In 50 patients post-emergency surgery for appendicitis or cholecystitis, 50% DMSO reduced postoperative wound complications to 4%, compared to 14% with 30% DMSO and 24% with traditional methods.
•One study injected DMSO directly into the biliary tree of mice (as sludging of bile in this region can lead to challenging gallstones). That study found that 50% DMSO caused no irritation, but 65% did (e.g., liver enzymes were elevated and necrosis, inflammation and fibrosis were observed). However, the irritation caused by 65% was transient and the rest of the bowel was not affected. Given that direct injections of 50% DMSO caused no issues and typically much lower concentrations of DMSO will contact the bile tract, this suggests DMSO is safe to administer to the biliary tract.
Note: the purpose of this study was to determine if they were harmless agents which could be used to develop treatments for biliary disease (something which can often be quite challenging to deal with).
IV DMSO saved my gallbladder and reduced my inflammation to almost nothing in 2013. Soon after, my alt GI doc no longer had access to it. She was getting it from Switzerland at the time.
Lungs
DMSO protects the lungs from injuries, treats acute respiratory diseases (e.g., acute stenosing laryngotracheobronchitis in children), and also helps with a few challenging conditions.
Lung Injuries
•DMSO was found to prevent ischemia-reperfusion injuries to the lungs.
•In rats, DMSO was found to prevent lung injury from hemorrhagic shock (significant blood loss) and transfusing lost fluids back into the circulation.
•Giving DMSO before alloxan (a toxin) was found to prevent the inflammation, cellular damage, and edema alloxan causes in the lungs.
Note: this study also found DMSO prevents acute pulmonary edema.
•DMSO was found to prevent the oxygen deprivation and inability to exchange gasses through the lungs which results from an Ehrlichia ruminantium infection (which is typically fatal).
•In rats, DMSO was found to prevent the significant inflammation and tissue injury which follows a significant traumatic impact to the lung.
•After sheep experienced a lung injury from inhaling smoke, nebulized DMSO (with heparin) was found to reduce the damage to their lungs significantly.
Note: as I have shown in this section, studies exist that show that nebulizing DMSO can be quite beneficial to the lungs. In contrast, a rabbit study found that inhaling 25-50 ml/hr of DMSO for an hour each day for 8 weeks caused pathologic changes in the liver and lungs. While this was a high dose, nebulizing DMSO has nonetheless been advised against in the DMSO field (which I believe was due to that rabbit study). The best conclusion I can draw from these conflicting data points is that DMSO should only be used for acute injuries in the lungs but not chronically nebulized.
Acute Respiratory Distress Syndrome (ARDS)
ARDS is quite challenging to treat (and a common reason people end up on ventilators), so DMSO’s potential to help the condition is quite noteworthy:
•In hamsters, an inflammatory peptide was put into the airway to trigger ARDS (a severe lung condition that often results in ventilation). When DMSO was subsequently given, it was found to reduce the inflammation and fluid in the lungs significantly.
•A similar mouse ARDS study that used bacterial LPS to injure the lungs also found DMSO reduced lung inflammation and fluid leak along with damage to the lining of the lungs.
•A third mouse study found that DMSO prevented LPS damage to the lungs, kept all treated mice from dying (whereas 58% of controls died), and maintained the ability of the lungs to produce ATP.
Note: a few studies have found that DMSO makes a part of the mitochondria able to synthesize ATP (the source of cellular energy) without the rest of the mitochondria being present. This, in turn, hints at the possibility DMSO can allow compromised cells to continue producing ATP (and thereby play a role in preventing cell death).
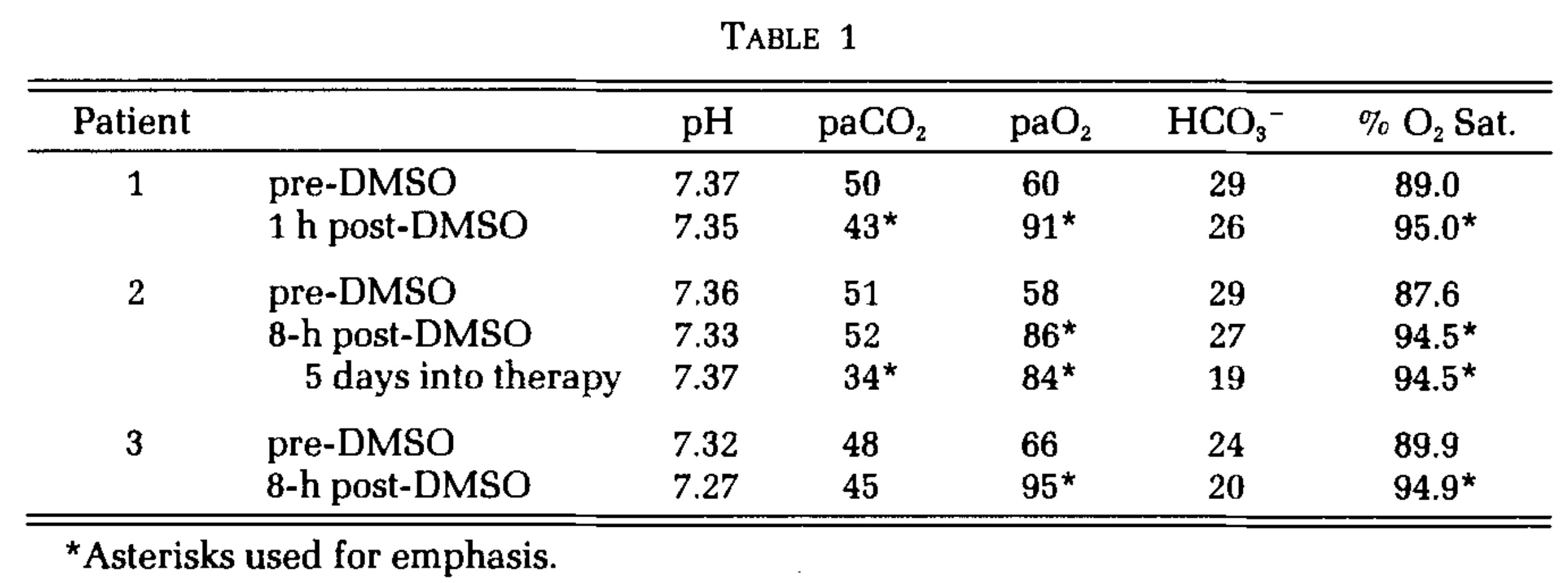
In the one human study where DMSO was used for ARDS (given intravenously at concentrations under 10%) it was found to produce a dramatic improvement in all three patients who received it (e.g., one patient’s lungs were completely normal after a week) and prior to receiving DMSO all three were near death. Additionally, in the one case when DMSO was nebulized, the improvement occurred in 1 hour.
Note: another study found that DMSO reduced immune cell infiltration of a lung infection, which can both be beneficial (as it explains how DMSO prevents the immune system from attacking the lungs), but also problematic as it loses the ability to fight off a significant infection. That study, hence suggests that DMSO should never be used alone as a treatment for bacterial pneumonia (whereas later in this series I will discuss how DMSO can increase the potency of antibiotics).
Chronic Lung Diseases
DMSO was found to reduce chronic pulmonary fibrosis, and this beneficial effect was increased when it was mixed with zinc.
For older patients with chronic respiratory insufficiency (leading to chronically low blood oxygen levels, elevated carbon dioxide levels and an abnormal acid base balance, especially during exercises) due to issues in the lungs or bronchi, daily intramuscular DMSO was found to bring about a recovery without the need for hospitalization in 35/43 (81%).
Note: DMSO has also been shown to treat asthma and chronic non-specific lung diseases.
Pancreas
DMSO (7-16%) has been shown to rapidly permeate the pancreas and shows promise for diabetes and pancreatitis.
Diabetes
Some Type 1 and Type 2 diabetics have reported that DMSO reduces (but does not eliminate) their need for insulin and that DMSO is particularly helpful for the condition since it can also alleviate the pain from diabetic peripheral neuropathy. Studies in this area include:
•Alloxan is toxic to the insulin producing cells of the pancreas and can be used to induce diabetes. A 1977 study found that if DMSO was injected prior to administering alloxan, they did not develop diabetes (although a higher dose of alloxan caused the dose of DMSO only to provide partial protection against diabetes).
•Type 1 diabetes results from the immune system attacking the insulin secreting cells of the pancreas. One strategy for treating type 1 diabetes is to transplant healthy insulin secreting cells into the pancreas. Unfortunately, this strategy often fails because the immune system will attack the transplanted cells too. However, in a mouse study, DMSO was found to protect those transplanted cells by decreasing IFN-γ expression and the number of dendritic, CD8, and Th1 immune cells while increasing Treg cell differentiation—all of which showed DMSO prevents suppresses spontaneous diabetes and autoimmune recurrence of type 1 diabetes.
•In both rabbit and rat bone marrow stem cells, DMSO combined with high glucose, boosted key insulin promoting genes (e.g., Pdx-1), within 3 days transformed these cells within 3 days into clusters of insulin-producing islet-like cells. Furthermore, in the rat cells, by day 10, insulin, glucagon, and somatostatin were produced (with insulin secretion increasing from 5.56 to 24.5 μU/mL under high glucose conditions).1,2,3
Note: while diabetes due to a loss of insulin producing cells is typically associated with type 1 diabetes, this loss also contributes to type 2 diabetes (particularly as it becomes more severe). As such, DMSO potentially facilitating the body to replace them is quite noteworthy.
•GLP-1 is a key hormone the body uses to regulate satiety and blood sugar (and which diabetes drugs like Ozempic mimic). One study found that 0.5-2.5% DMSO increased GLP-1’s production of insulin by 2-2.5 times. The study’s findings suggest DMSO could help treat diabetes or allow GLP-1 users to use a lower dose of the medication.
•Exposing insulin secreting cells to DMSO was found to enhance glucose-induced and tolbutamide-stimulated insulin secretion without significant effects on basal secretion or potassium responsiveness. Conversely, another study found that at high doses, DMSO would inhibit insulin secretion (however that inhibitory dose is much higher than a DMSO user’s pancreas would ever be exposed to).
Pancreatitis
Pancreatitis is often quite challenging and dangerous (as there are no conventional treatments for it outside of cases where an obstruction causes it—rather hospitals can only support the patient until they recover). Fortunately, DMSO (and ultraviolet blood irradiation) have been shown to be quite effective for treating it. For example:
•After inducing pancreatitis in rats, DMSO was found to improve pancreatic microcirculation and reduce ICAM-1 expression (a key part of the disease process) and subsequent leukocyte adhesion.
•Another mouse study found DMSO significantly reduced the pancreatic edema resulting from dietary induced pancreatitis.
•In rats, DMSO treated acute hemorrhagic necrotizing pancreatitis (a condition which typically has a mortality rate between 25-40%).
•A rat study found DMSO protected the pancreas from cerulein induced pancreatitis (e.g., through inhibiting lipid peroxidation in pancreatic tissue, reducing pancreatic edema, reducing how many digestive enyzmes leave the pancreas and reducing the pathologic vacuolization of the pancreas’s acinar cells).
•A randomized double-blind trial took 78 patients with chronic recurring pancreatitis (and no other confounding gastrointestinal disorders) who presented within 2 hours with signs of pancreatitis but did not have signs of generalized peritonitis. Of them, 26 received 10% DMSO rectally, and at least 57% were free of pain after 12 hours (compared to 17% of controls), and all were free of pain after 24 hours (whereas 48% of controls were still in pain). As a result, all DMSO subjects were discharged within 3 days, whereas only 22% of controls were discharged after 5 days of hospitalization.
•In patients with recurrent pancreatitis, DMSO combined with allopurinol enhanced the efficacy of narcotic analgesics, significantly reducing pain, white cell counts, and serum lactate dehydrogenase levels (indicative of reduced pancreatic and peripancreatic inflammation and necrosis) compared to controls.1,2
•In three patients with chronic alcohol-induced pancreatitis, rectal DMSO achieved complete pain relief within 12 hours and resolved epigastric tenderness by day four, compared to persistent pain with placebo (pethidine, hyoscine, metoclopramide). No comparison between DMSO alone and DMSO with allopurinol was reported.
•DMSO with fluorouracil effectively prevented and treated acute postoperative pancreatitis.
Note: one German author advocates combining IV DMSO with chlorine dioxide (given at a much slower drop rate) for pancreatitis.
Kidneys
Many different facets of DMSO’s interactions with the kidneys have been researched:
Safety
•A rabbit study found that rabbit kidneys perfused for 60 min with DMSO was unaffected by 1.4M (10.8%) DMSO, but higher concentrations (2.1 and 2.8 M) produced appreciable toxic effects to the kidneys.
A study of paraplegics found that IV DMSO caused no alteration of urinary function or urinary sediment (other than a transient increase in blood cells if osmotic hemolysis occurred from too high of an IV DMSO concentration).
•This study of 7 people found 10-40% IV DMSO caused no acute toxicity to the kidneys.
•A dog study found that in dogs with chronic kidney disease, unless they had stage 4 CKD, DMSO had no adverse effects, and in less severe cases, some improvements were observed.
Note: DMSO often functions as a potent diuretic (although the effects are highly concentration dependent). For example, one dog study found after 1 hour 40% IV DMSO caused a fivefold increase in urination, a rat study found giving it topically five times a day increased urine volume 10-fold, and human study also found 40% IV DMSO caused significant urination. Conversely, this diuretic function is often extremely helpful (e.g., it will take excessive fluid outside of regions it has leaked into) and accounts for some of the significant benefits seen from DMSO.
Ischemia-Reperfusion Injuries
•In rats, renal ischemia was induced by cutting off the blood supply to the kidney for 1 hour, after which, DMSO or saline was given intravenously. All the saline treated rats had significantly worsened kidney function and died within seven days, while all the DMSO treated rats survived and had near normal kidney function (with somewhat greater protection seen if DMSO was given beforehand).
•In a nearly identical experiment, equivalent protection was observed, along with urine flow being observed to resume within 15 minutes of the DMSO infusion. Protection was also observed in another rat study and in one where DMSO was given concurrently with vitamin E (resulting in significantly reduced oxidative stress and largely preserved perfusion). Finally, a rat NMR study showed that DMSO significantly reduced the damaging sodium spike seen in kidneys after their blood supply was cut off.
• A similar experiment in dogs found DMSO again preserved a near normal kidney function (whereas in the saline treated dogs, 1 died and 4 had transient renal failure).1,2
•In rabbits, DMSO administered post-ischemia reduced renal damage and apoptosis in an ischemia-reperfusion model compared to saline. Serum creatinine increased less (245% vs. 318%, p=0.003), and histopathology showed milder tubular damage (5% vs. 22% severe lesions, p<0.05) with reduced apoptosis and necrosis, suggesting DMSO’s protective role against acute kidney injury.
•A nuclear magnetic resonance imaging study of rat kidneys (a method which makes it possible to detect minute and otherwise invisible changes) found that DMSO protected the kidneys from the damage that occurred when their access to oxygen was cut off, but it did not prevent the transient drop in kidney function which occurred during this period.
Toxic and Dietary Injuries
•In rats with kidney injury caused by zymosan, intraperitoneal DMSO preserved blood flow and kidney function while reducing kidney swelling and markers of oxidative stress (e.g., there was a 15-24% improvement in blood flow, a 40.5% reduction in plasma creatinine, and a 4.4-5.4% reduction in kidney edema).
•A mouse study found if DMSO was given within 3 hours of injecting mercury subcutaneously, it prevented the kidney damage which typically resulted over the next two days (however at 5 hours it was too late). Additionally, the results suggested this protection was not due to DMSO chelating mercury but rather it neutralizing oxidative damage.
•A rat study found DMSO prevented the kidney damage caused by gentamycin, and that (like the previous mouse study) it also restored the levels of GSH and SOD enzyme activity to near normal.
•Intraperitoneal DMSO given to rats prior to 6 gy of radiation (a near lethal dose) protected rat kidneys from radiation induced kidney damage , with significantly lower markers of oxidative stress found in kidney tissue 24 weeks post-irradiation compared to untreated controls.1,2
•In rats, DMSO was found to counteract many of the complications of a dietary copper deficiencies (e.g., enlarged hearts, or reduced gamma-glutamyl transferase function).
Kidney Function
•When kidney tissues were frozen, DMSO was found to greatly increase the conductivity of the tissue.
•DMSO was found to increase rabbit kidney’s flow rate and changed the GFR, but did not change Na+ reabsorption or fractional water excretion, leading the investigators to conclude DMSO may shift the regulation of urine flow rate from tubular reabsorption.
•Many studies and case reports (listed in this article) have found that DMSO improves renal function in patients with amyloidosis. For example, this study of 15 patients with amyloid A amyloidosis resulting from autoimmune conditions improved the kidney function in 5 out of 10 renal amyloidosis patients but could not help severe cases, while this study of two people with renal failure found both had a dramatic improvement from DMSO.
•DMSO was also found to inhibit the kidney’s Na+-K+-ATPase pump in a comparable degree to Ouabain or atrial natriuretic peptides (ANP), but did so in a manner independent from how either functioned.
Note: Ouabain or its derivatives are often used in integrative cardiology, while ANP is a naturally occurring hormone that protects both the heart and kidneys.
A rabbit study found DMSO caused an increase in filtration fraction, and at high concentrations, a decrease in renal blood flow and urine volume.
In one rat study, DMSO was shown to act as a diuretic by selectively decreasing the osmotic permeability of the region of the kidneys which reabsorb water (causing it to instead be urinated out). In another, 5% oral DMSO significantly increased urinary output by directly acting upon the kidneys (and possibly by altering ADH secretion).
•Exposing kidney cells to 10-20% DMSO was found to increase their metabolism, while higher concentrations (which are never used in humans) was found to be toxic to the kidneys.
Note: one dog study found that DMSO was contraindicated in dogs with stage IV kidney disease.
Autoimmune Diseases
•Many kidney autoimmune diseases result from immune deposits in the kidneys (one of which is Heymann nephritis, an experimentally induced form of nephritis where antibodies that target the kidneys are injected causing immune deposits on the glomerular walls). In a rat study of Heymann nephritis, DMSO was found to reduce protein leaking into the urine, suggesting it prevents autoimmune kidney damage. Another rat study (which was more detailed) also had similar results, as did a third rat study.
•A 1985, another 1985, and a 1987 study of DMSO treated rats (and controls) with lupus nephritis found that those who received DMSO had nearly normal kidneys, whereas the controls had significant damage to their kidneys. For example, one study found a 25.2% reduction in proteinuria after 5 months, a significantly reduced urine protein to creatinine ratio, and at 7 months, 83% of DMSO treated rats had normal kidneys whereas 75% of untreated rats had focal proliferative glomerulonephritis, crescents, and glomerular obsolescence (which correlate to serious kidney damage).
Kidney Stones
•A study of 6 patients with kidney stones (5 of which were confirmed by ultrasound) found IV DMSO resolved the condition in 2-3 treatments (although one patient had a complete resolution after a single infusion).
Note: I located a rat study which I believe found similar results, but I could not find the actual study to verify this.
A 1967 study fed rats a diet designed to create kidney stones, and found that after two months, 40 of the 45 water-drinking rats had developed stones in the kidney, bladder or ureter, while only 11 of the 46 DMSO group did.
Note: the author of that study later conducted another studythat strongly suggested DMSO eliminated kidney stones by improving their colloidal dispersion (zeta potential). We in turn, have had a great deal of success treating kidney stones by improving the physiologic zeta potential.
Urinary Tract
The majority of urinary tract research has been for interstitial cystitis (the one condition which DMSO has FDA approval to treat), and is detailed here. However, DMSO has been used to treat many conditions throughout the urinary tract. For example:
•A 1967 study found DMSO treats a wide range of genitourinary disorders:
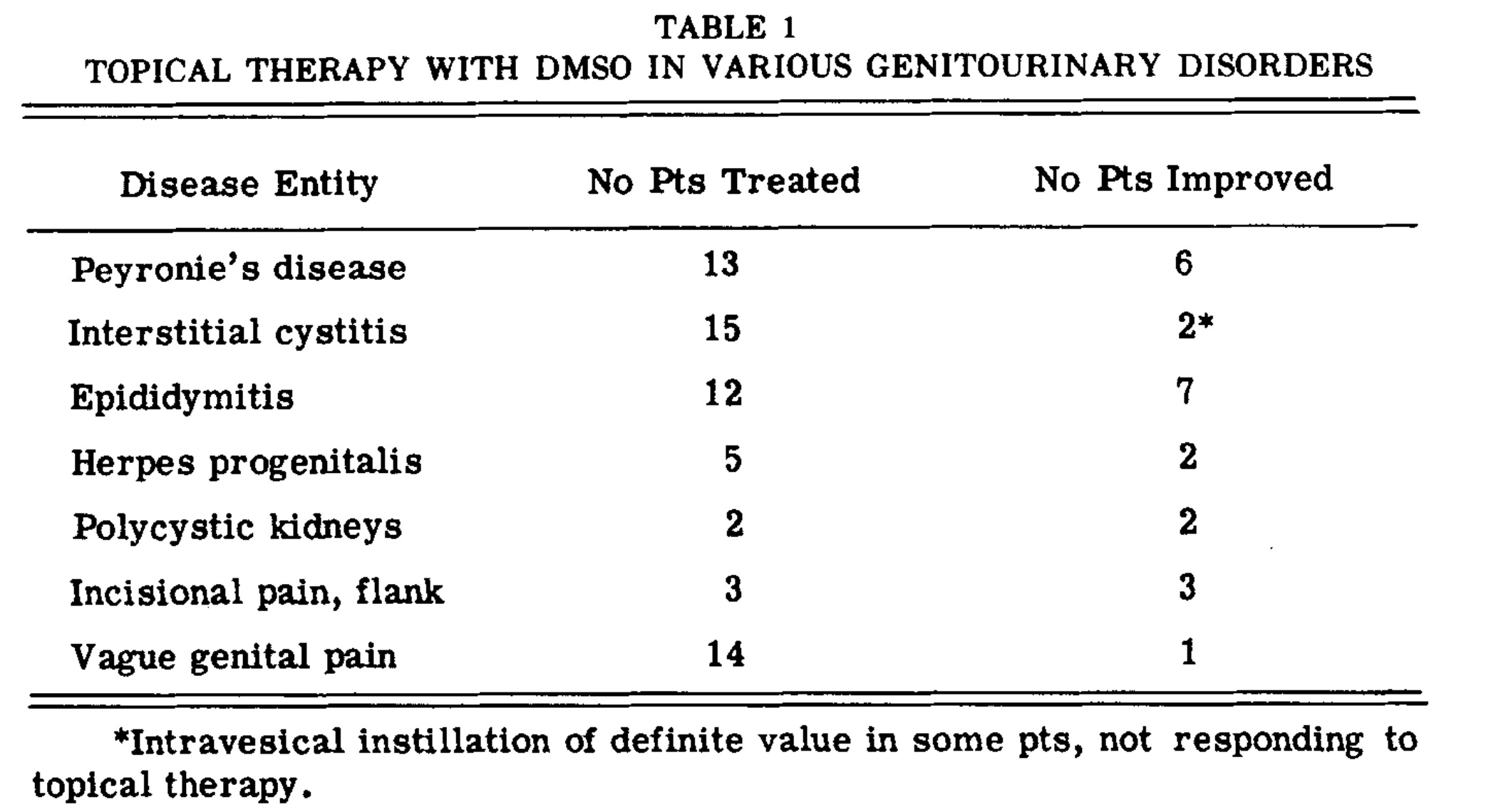
Note: this publication was preceded a preliminary report which had less data, but specified the type of pain (e.g., suprapubic, genital, renal colic—of which kidney stone and surgical pain syndromes had the best response).
•A 1978 study found DMSO frequently treats inflammatory conditions of the urinary tract:1,2,3

Note: another study of 26 patients with radiation-induced hemorrhagic cystitis, intravesical DMSO instillation combined with green laser hemostasis significantly reduced hematuria, pelvic pain, and frequent urination by 6 months, with effects comparable to hyperbaric oxygen, though some experienced recurrent hematuria by 12 months.
•A 1980 study gave DMSO to 8 patients with inflammatory conditions of the urinary tract (e.g., interstitial cystitis, urethral syndrome, incrustation of the prostatic cell, actinic cystitis and chronic prostatitis), all of whom had a positive response and no side effects.
•A 1985 study gave 4 men with chronic excessive (and untreatable) urination due to either chronic prostatitis, chronic cystitis, tuberculous contracted bladder and interstitial cystitis DMSO. Three of the four had an excellent response to treatment, with the one non-responder having an unclear disease process (the doctors’ best guess was that it was chronic cystitis).
•A 1987 study found urethral syndrome (chronic irritation of the urethra without signs of an infection) responds to DMSO.
DMSO has also been shown to increase bladder wall absorption of intravesical agents with minimal systemic absorption:
•A 2019 safety study found six healthy adult Japanese males retaining DMSO for 15 minutes had no side effects (besides four having a mild-like like breath) and that DMSO generally stayed within the bladder (e.g., it only was found in the bloodstream of one of the six and overall 83.7% of DMSO being recovered from the bladder).
•A 2023 rat study found DMSO increased the absorption of epirubicin (an intravesical chemotherapy) into the bladder wall and reduced the bladder damage (e.g., fibrosis) typically seen with the therapy. Likewise, a 1982 dog study showed DMSO increased the bladder wall absorption of cisplatin, likely in a dose related manner.
One cause of incontinence is overactivity of the bladder muscle, which is sometimes treated by intravesical injecting Botox into the bladder wall, a procedure which while effective has side effects. Because of this, researchers have explored instead delivering intravesical botox with DMSO:
•In rats, intravesical 25% DMSO and Botox was shown to synergistically enhanced Botox absorption, resulting in 56.8% of SNAP-25 protein (Botox’s target) being cleaved within 7 days. It also increased expression of CGRP mRNA four-fold 1-2 weeks later, which resulted in a suppression of CGRP release and hence reduced inflammation and contractile impairment (e.g., that triggered by acetic acid).1,2
•In a phase 1/2 trial, 25 women with medication-resistant idiopathic detrusor overactivity received intravesical instillation of 300 units of botulinum toxin A mixed with 50 ml of 50% dimethyl sulfoxide (DMSO), resulting in no serious adverse effects or significant increases in postvoid residual. Among the 21 women who completed phase 2, median incontinent episodes decreased from 4 to 2 at 1 month, with improved scores on the Incontinence Impact Questionnaire (13 to 7) and Urogenital Distress Inventory (10 to 5), and severe urgency reduced from 52% to 5% at 1 month and 14% at 3 months.1,2
Note: studies also show DMSO affects bladder emptying with the effects varying by concentration. In one, it enhanced rat bladder permeability, enhancing the effects of intravesical ions, osmolality, and pH on the bladder’s volume-pressure response, potentially being of benefit in conditions with renal insufficiency or excessive urinary retention. In another, 0.5-5% DMSO enhanced acetylcholine (ACh)-induced rat urinary bladder smooth muscle contractions by inhibiting acetylcholinesterase while suppressing carbachol and potassium induced contractions. Finally, in a third, 40% DMSO abolished the ability of electrical fields to simulate bladder contractions, whereas 30% DMSO reduced contractions to reduced their force by 40% (wearing off in 30 minutes) and 25% had no effect. Additionally, DMSO also reduced acetyl choline and potassium induced contractions (roughly halving it).
Male Reproductive Tract
The previously cited study is the most detailed assessment I have located on the effects of DMSO upon the reproductive tract, however can also help many other parts of the urinary tract:
Many studies other studies have corroborated these results.
Prostate
Prostate issues are a frequent concern for men (e.g., prostate cancer is the most common cancer in men, benign enlargement eventually afflicts most aging men, and chronic prostatitis is notoriously refractory to treatment—in part because the prostate is difficult for drugs to penetrate). DMSO hence was explored for each of these issues, and alone or in combination with another therapy has shown significant benefit, particularly in Russia and Ukraine (where it is frequently administered via the urethra or rectum).
Prostate cancer. DMSO can differentiate malignant, fast-dividing cells back toward a more mature, slower-growing state. In cultured human prostatic adenocarcinoma cells, DMSO inhibited growth and induced differentiation,1,2 while in rat prostate adenocarcinoma cells it was cytostatic (growth slowing) rather than toxic, slowing division and shifting the cells toward a differentiated phenotype while suppressing the glycosaminoglycans that tumors shed to invade1,2 (and separately, DMSO has been measured as roughly eight times more toxic to prostate cancer cells than ethanol1 ). DMSO also restored the normal (non-malignant) pattern of metabolic enzymes in rat prostate tumor cells,1 and drove normal prostate epithelial cells toward specialized transport function (indicating it has a specific affinity for differentiating prostate tissue).1
That differentiation translates into slower tumor growth in living animals. In the aggressive Dunning rat prostate carcinoma model, oral DMSO alone significantly slowed tumor growth1 whether given before tumor implantation, at the time of implantation, or after tumors were already established, with longer treatment producing greater inhibition and no toxicity or weight loss.1
Note: DMSO’s metabolite DMSO2 (MSM) has also been shown to induce apoptosis and reduce invasiveness of prostate cancer cells.1
Furthermore, DMSO sensitizes cancers to chemotherapy and this effect has also been seen for prostate cancer: in the Dunning rat model, DMSO enabled sub-therapeutic, normally ineffective doses of 5-FU, cisplatin and cyclophosphamide to markedly shrink tumors, without added toxicity.1
Note: while DMSO generally enhances chemotherapy, due to its affinity for platinum compounds, some studies find it reduces the potency of these agents (e.g., one study found DMSO induced up to roughly threefold resistance to cisplatin in testicular embryonal carcinoma lines1).
These therapeutic effects are also cumulative. A recent study found DMSO reduced prostate cancer cell growth on its own and more so when paired with nelfinavir,1 and DMSO concentrations known to induce differentiation also markedly increased the cancer-cell-killing of onconase in prostate (and leukemia) lines.1
In humans, DMSO has also been used to counteract the complications of prostate cancer. A 2011 study gave DMSO combined with sodium bicarbonate intravenously to patients with metastatic prostate cancer which significantly improved major cancer symptoms and was accompanied by significant objective improvements.1,2
Likewise, in a single advanced (stage IV, metastatic) case, a disulfiram-in-DMSO preparation produced a marked PSA drop (from 697 to 12.6), weight gain, and restored quality of life over roughly three years.1
DMSO has also been used as the carrier for hematoxylin, a compound that selectively kills cancer cells and safely produces remarkable results rarely seen in oncology, including for prostate cancer (the full story of D-hematoxylin is told here).
Finally, a very large body of studies used DMSO as the vehicle to deliver some other agent against prostate cancer, thereby (like hematoxylin) allowing them to be more effective than they would be alone and providing numerous potential therapeutic combinations to consider. Lastly, beyond the shared anti-cancer properties being seen across a variety of agents suggesting part of the benefits seen arose from DMSO, many studies also explicitly noted the safety of the combination (again reaffirming DMSO’s safety).
Note: DMSO’s safety for the prostate was also validated in a variety of studies on a DMSO based reversible contraceptive, one of which (with NMR) found after 8 years, prostate-derived citrate, acid phosphatase and fructose all remained normal (indicating preserved prostate and seminal-vesicle function).1,2
Among natural compounds delivered in DMSO, curcumin⬖ reduced tumor weight and enhanced immune function in prostate-cancer-bearing mice,1 dihydroartemisinin⬖ induced apoptosis and restored p16 expression in PC-3 cells and xenografts (cancers implanted onto animals),1 S-equol⬖1 suppressed three prostate cancer lines and xenograft growth while sparing normal cells, and equol⬖ lowered PSA and DHT and reduced prostate weight.1 Apigenin⬖ shifted Bax/Bcl-2 toward apoptosis in xenografts,1 silibinin⬖ blocked the cancer-associated fibroblast transition,1 ginsenoside Rh2⬖1 and Rg3⬖1 drove apoptosis (which Rg3 did via ROS1), and berberine⬖ overcame paclitaxel resistance by suppressing IL-6/STAT3.1 Melatonin⬖ blocked the epithelial-mesenchymal transition driving prostate cancer spread,1 andrographolide⬖ and asiaticoside⬖ inhibited bone-metastatic prostate cells via Notch suppression,1 and sparstolonin B,⬖1 aloperine⬖1 and fangchinoline⬖1 each triggered apoptosis through the PI3K/AKT/mTOR or mitochondrial pathways. Additional natural agents that treated prostate cancer when combined with DMSO include platycodin D,⬖1 afzelin,⬖1 emodin,⬖1 triptolide,⬖1,2 resveratrol esters,⬖1 ginger extract,⬖1 astragaloside,⬖1 ellagic acid,⬖1 the lignans enterolactone⬖ and enterodiol,⬖1,2 pterostilbene,⬖1 Morus nigra extract,⬖1 ashwagandha,⬖1 Croton leaf extract⬖ (via lupeol),1 tolfenamic acid,⬖1 Turkish propolis,⬖1 sulforaphane,⬖1 and the DMSO-prepared herbal extract Yangzhengxiaoji (where DMSO is integral to the active formulation), which suppressed prostate and other cancer cell migration through PI3K/AKT.1
A parallel set of synthetic and repurposed drugs mixed with DMSO also demonstrated anti-prostate cancer activity: itraconazole,1 lovastatin,1 fenbendazole,1 rapamycin,1 celecoxib,1 salinomycin,1 the HSP90 inhibitor 17AAG,1 dexamethasone,1 the STAT3 inhibitor AG-490,1 the NF-κB inhibitor BAY 11-7082,1 the SIRT1 inhibitor sirtinol,1 the CXCR2 antagonist SB225002,1 the deubiquitinase inhibitor b-AP15,1 the p53 radiosensitizer PRIMA-1met,1 the gap-junction enhancer PQ1 with cisplatin,1 the Plk1 inhibitor with HDAC inhibitors,1 morin potentiating paclitaxel,1 and the ferroptosis inducers RSL3 and erastin potentiating docetaxel and cisplatin.1,2
Several readers, in turn, have described using DMSO as one component of a self-directed cancer regimen, generally alongside other agents. These reports include a man with stage IV prostate cancer reporting he was approaching no evidence of disease on a protocol combining DMSO with ivermectin, fenbendazole, high-dose IV vitamin C and other supplements,1 a chemist who developed prostate cancer after decades of recurrent infections and later used DMSO regularly,1 and a reader using a 50% DMSO bladder instillation after high-dose IV vitamin C for recurrent urothelial carcinoma who reported his symptoms fully resolved1 and one who noted the value in rectal DMSO for targeting prostate cancer.1
One reader I correspond with has also reported using topical DMSO-ivermectin directly over his patient’s tumors: in addition to a metastatic colon cancer, he described an apparent good response in five prostate cancers (along with one breast and one ovarian cancer) that had not metastasized, though he cautioned that conclusive data is still being awaited and that roughly thirty further patients given the protocol could not be followed up.
Prostatitis: Chronic prostatitis is common, painful and famously hard to cure as antibiotics struggle to penetrate the prostate. DMSO not only solves the antibiotic problem (and does so for a wide range of challenging infections), but also directly treats prostatitis through its own anti-inflammatory, analgesic and fibrinolytic action. The bulk of the evidence showing this is a large body of Russian and Ukrainian clinical work in which DMSO, delivered rectally or through the urethra, was successfully combined with a variety of antimicrobial agents.
The single most consistent finding is that adding DMSO-based local delivery to standard therapy improves outcomes. In men with chronic bacterial prostatitis (including those whose fertility was impaired), rectal microenemas of a DMSO-enzyme-antibiotic mixture added to standard treatment produced significantly greater reductions in symptom scores, better clearance of inflammatory cells from prostate secretions, improved sperm parameters, and better restoration of prostate blood flow than standard therapy alone (e.g., leukocytospermia normalized in all but 7.1% vs. 42.9% of controls, maximum urinary flow rose by 4.1 ml/s, and prostatic blood flow improved in 76% vs. 33% of controls).1,2 Combined physiotherapy regimens delivering chymotrypsin with DMSO by electrophoresis raised cure rates and shortened treatment in hundreds of outpatients with chronic infectious prostatitis (84.9% pathogen eradication versus 56.6% in controls, with symptoms regressing about 10 days sooner and remission sustained in 89% at 6 months).1,2,3 For chronic chlamydial and trichomonad prostatitis, DMSO mixed with enzymes or antiprotozoals and delivered through the INTRAMAG device (which uses a pulsed magnetic field to drive medications through the urethra into the prostate) or by iontophoresis improved pathogen eradication, shrank prostate volume (from roughly 35 to 22 cm³), and normalized prostate-secretion findings beyond systemic drugs alone.1,2 DMSO microclyster regimens combining antibiotics, heparin and other agents (sometimes with rectal hyperthermia or a barochamber) achieved sustained improvement in the large majority of chronic prostatitis patients across a range of infectious causes.1,2,3 DMSO has also carried antibiotics and peptides into the prostate via suppositories, ointments, propolis-based gels and umbilical (navel) plasters, all reporting symptom relief and reduced inflammation (e.g., 80-95% of those receiving propolis gel improved).1,2,3,4
The most remarkable single result comes from the physician in Ecuador who refined D-hematoxylin: his work, with the support of Stanley Jacob (the pioneer of DMSO), began with curing 44 of 45 cases of microbiologically confirmed chronic bacterial prostatitis using DMSO combined with antibiotics applied directly into the bladder (much as DMSO is FDA-approved to treat interstitial cystitis), with patients testing negative for infection 15 to 20 days after treatment and no subsequent recurrences, demonstrating DMSO’s ability to counteract bacterial resistance (after which he was inspired to begin exploring the approach to treat prostate cancer).
Reader reports independently echo this combination. One described roughly forty years of chronic prostate infections that never responded to antibiotics and always returned within weeks; knowing DMSO’s penetration-enhancing action, he tried taking his antibiotic with a small amount of DMSO and reported immediate relief from infections that then never returned, noting only that he wished he had tried it many years earlier.1 Another reader reported relieving a prolonged bout of prostatitis with a painted-on mixture of DMSO, water and food-grade aloe vera.1 Other readers similarly reported DMSO resolving chronic or recurrent prostatitis in themselves and relatives.1,2 Lastly, Pierre Kory shared a case with me of a patient whose prostatitis was resolved with DMSO.
For chronic abacterial prostatitis and chronic pelvic pain syndrome (CPPS), the most common and most frustrating form, DMSO has been used both for its direct anti-inflammatory effect and, increasingly, for its action on the pelvic floor. Intravesical DMSO has been noted to relieve the symptoms of category III prostatitis, suggesting a role for it in the neurogenic inflammation underlying the condition.1 Rectal DMSO combined with anti-inflammatories and antispasmodics has relieved CPPS pain and urinary symptoms (e.g., in one CPPS protocol pain fell from 4.2 to 1.1 points),1,2 as has DMSO-prostatilen (peptide) suppository therapy paired with perineal vibromagnetic treatment (where pain fell in 67% versus 34% of controls, NIH-CPSI dropped 72% versus 53%, and Qmax rose 29% versus 13%).1 The pelvic-floor angle is mechanistically supported by work in women, where intravaginal DMSO measurably relaxed the levator ani muscles and normalized their resting electrical activity (shifting 85% of patients toward a normal EMG pattern with reduced activity on straining); this normalization of pelvic-floor muscle tone paralleled relief of their pelvic pain, leading the authors to conclude DMSO exerts analgesic, anti-inflammatory and muscle-relaxant effects on the pelvic floor.1 Men have the same pelvic-floor muscles, whose spasm and hypertonicity drive much of CP/CPPS, so the same mechanism plausibly applies. Several of these chronic-prostatitis regimens also improved the sexual function of treated men.1,2,3
Calculous prostatitis (prostate stones). A distinct application uses DMSO to carry stone-dissolving agents to prostatic calculi. DMSO combined with chelators (such as Trilon B) or collagenolytic enzymes (Fermenkol), delivered rectally as suppositories or by electrophoresis, has dissolved or shrunk prostate stones, reduced fibrosis, relieved pain, and improved urination and fertility across multiple patient series (e.g., (in one series of 17, stones disappeared or shrank in 12; in another of 100, smaller stones dissolved in 94-100% of cases alongside a 26-32% reduction in prostate volume; and adding the enzyme-DMSO mixture raised overall efficacy by 30% over controls).1,2,3,4
Benign prostatic hyperplasia (BPH). DMSO has a long history with prostate enlargement, beginning with Stanley Jacob himself, who recommended DMSO for enlarged prostates that made urination difficult (one man in the historic DMSO literature reported it let him sleep through the night again). Jacob also recounted a Texas physician who injected DMSO plus progesterone into enlarged prostates, with biopsies reportedly showing a return toward normal, which is plausible given that progesterone, like DMSO, has independently been reported to shrink enlarged prostates.1,2
Note: I suspect DMSO’s benefits in BPH are due to its muscle relaxing and anti-inflammatory properties, its ability to reduce congestion and prostatic edema (thereby decreasing glandular swelling) and possibly, its capacity to circulation and nutrient delivery to the prostate (particularly since additional prostate benefits are often seen when DMSO is combined with an essential mineral).
The largest body of BPH evidence involves DMSO-prostatilen (peptide) rectal suppositories. Across multiple patient series, these suppositories relieved obstructive urinary symptoms, reduced residual urine, improved urinary flow rate, and lowered symptom scores, with benefits persisting between treatment courses (IPSS fell from about 17 to 10, daytime urinations from roughly 9.4 to 5.3, residual urine by over 50%, and maximum urinary flow rose from roughly 7.9 to 17.8 ml/s).1,2,3,4 The clearest evidence that DMSO itself contributes comes from a controlled comparison: in 96 BPH patients, the prostatilen suppository containing DMSO produced markedly better improvement in urinary flow and residual urine than an otherwise identical suppository without DMSO, despite equal peptide dosing (maximum flow rose from 8 to 18.1 ml/s with DMSO versus only 11.9 ml/s without it, and residual urine fell to 21 ml versus 33 ml).1,2 DMSO-camphor rectal preparations have also been patented for BPH (and prostatitis)1,2 and DMSO-delivered oxidized-dextran suppositories reduced the prostatic changes of experimental BPH.1
Numerous readers also corroborated DMSO’s utility for BPH. Several men taking oral DMSO (typically a teaspoon in water once daily) described frequent urination improving by roughly half within one to two weeks,1,2 the return of being able to sleep through the night without rising to urinate,1 and easier flow with reduced urgency; others applying it topically reported reduced urinary urgency and other significan improvements within days,1,2,3 with one man discontinuing Flomax after using topical DMSO once daily for a couple of weeks,1 and another using daily mini-enemas finding his prostate smaller and smooth again.1 One reader’s account captured the systemic pattern seen throughout this series: after a TURP (surgical reduction) for BPH he still passed water with difficulty and woke each morning feeling pressure on his kidneys, but within five days of oral DMSO he reported passing water far more easily, along with sharper thinking, somewhat improved eyesight and hearing, and a fall in blood pressure from 160/90 to 150/80.1
DMSO has likewise served as the vehicle in studies of natural and hormonal agents against BPH, including red clover isoflavones⬖ inhibiting BPH stromal cells,1 Plectranthus tuber extract⬖ reducing testosterone-induced prostate enlargement comparably to finasteride,1 2-methoxyestradiol attenuating testosterone-induced BPH,1 and Pygeum africanum⬖ (a classic BPH herb) where DMSO’s solubilizing role let it inhibit the leukotrienes driving prostatic inflammation.1 Additionally, plant extracts (such as Phellodendron amurense)1 and compounds (such as the Kv7.4/7.5 channel activator URO-K10)1 have been shown to relax prostate smooth muscle and ease lower urinary tract symptoms.
Prostate tuberculosis. A niche but well-documented application: in prostatic tuberculosis, where drugs notoriously fail to reach the gland, anti-tuberculosis agents (especially rifampicin) have been delivered by rectal suppository or microenema in DMSO. One regimen using rifampicin suppositories containing DMSO achieved 80.7- 96.6% positive responses across 68 patients.1 In prostate-TB patients, DMSO-rifampicin microenemas (combined with spermatoprotective therapy) improved both infection control and fertility parameters, and a comparison of delivery routes found the rectal DMSO cocktail best preserved sperm quality while controlling infection (the rectal route cut pyospermia by roughly 60%, comparable to intravenous delivery, while reducing sperm motility by only 14.5% versus 74.3% with the intravenous route).1,2 A documented case of prostate tuberculosis with prostatic caverns was successfully treated with a DMSO containing regimen.1
Radiation injury from prostate cancer therapy. DMSO is an established treatment for the radiation cystitis (bladder) and proctitis (rectum) inflammation that complicate pelvic radiotherapy, most commonly after prostate cancer treatment. Beginning with a 1978 American study in which half of longstanding radiation-cystitis patients responded to intravesical DMSO,1,2 a large literature (much of it Russian) has used intravesical DMSO instillations and rectal DMSO microenemas to control the bleeding, pain and inflammation of late radiation injury in prostate cancer patients, with high rates of symptomatic improvement (e.g., in one series of 149 men with late radiation rectitis, comprehensive DMSO-based therapy gave satisfactory results in 95%).1,2,3,4
Note: radiation cystitis from a variety of other cancer treatments has also responded to DMSO.
Lastly, DMSO mixed with lidocaine and instilled rectally significantly reduced the pain of probe insertion during transrectal ultrasound-guided prostate biopsy1,2 and when added to radiographic contrast, DMSO improves contrast penetration into the bladder wall and prostate, sharpening CT staging of bladder and prostate tumors.1,2
Testicles, Semen, Epididymis and Scrotum
The testicles are exquisitely vulnerable to oxidative stress and DMSO has been repeatedly shown to protect them from injury.
Radiation: Radiation-induced testicular injury has no approved preventive or treatment agent, which makes DMSO’s protective effect notable.1 When given before total body irradiation, DMSO preserved fertility (83.3% of females impregnated vs. 50% in irradiated controls, with larger litters and faster conception), restored testosterone, LH and FSH toward normal, reduced testicular atrophy, recovered epididymal sperm counts 1.7–2.3 fold, preserved spermatogonial stem cells, suppressed germ cell apoptosis, normalized oxidative stress, and reduced persistent DNA damage by enhancing homologous recombination repair (upregulated BRCA1 and RAD51).1,2. A separate radioprotective mixture of DMSO with glutathione and cysteamine, given 20 minutes before 6 Gy irradiation, raised surviving spermatogonia to 33% of control (vs. 6% irradiated-only), preserved sperm counts and viability, halved abnormal sperm, and lifted overall survival to 95% (vs. 35%).1,2. An earlier (1977) version of this combination likewise outperformed any single radioprotective agent 1.
Testicular torsion (ischemia/reperfusion): Across numerous rat testicular torsion models (which temporarily cuts off blood to the testis), DMSO alone (typically 3% given intraperitoneally before detorsion) cut testicular MDA (lipid peroxidation) and raised reduced glutathione, attenuating the oxidative injury of reperfusion.1,2,3 In one study, DMSO dropped MDA from 27.5 to 7.9 µmol/g at the end of ischemia and tripled GSH, with the effect holding throughout reperfusion.1 In studies testing ternatin, lipoic acid or carvacrol against torsion (delivered with DMSO), DMSO alone produced significant protection, which the tested agents then built upon.1,2 Tyrphostin and rapamycin torsion studies using DMSO found a similar protective effect.1,2
In cultured Leydig (testosterone producing) cells DMSO preserved P-450 steroid producing enzymes (17α-hydroxylase, C17-20 lyase) by scavenging hydroxyl radicals,1 and enhanced basal and hCG-stimulated testosterone output over days 2–4, especially under low oxygen, consistent with protection of the enzymes from free-radical damage.1 DMSO can also raise testosterone on its own: oral DMSO (2 ml daily) significantly increased serum testosterone in rats on days 2, 14 and 28, with the Leydig cells becoming more numerous and enlarged, indicating DMSO stimulated the testosterone-producing cells directly.1,2 It may also amplify testosterone’s downstream activity, since DMSO combined with testosterone induced the metabolic enzyme CYP3A4 beyond what testosterone produced alone.1 In sperm directly, DMSO scavenged reactive oxygen species and reduced the loss of motility caused by activated neutrophils.1,2,3
Several readers also reported effects consistent with this direct stimulation of the testosterone-producing cells. One, recovering from low testosterone after a weight cut reported that applying DMSO to the testicles (and the head of the penis) produced a rapid return of erections within a few hours, which he likened to a “wake-up call” for his gonads, along with noticeably firmer erections afterward.1
DMSO has also been used in combination with a variety of agents (which if natural are marked with a ⬖) to protect the testicle against toxic insults, and across a wide range of combinations consistently preserved testicular histology, sperm parameters and testosterone that would otherwise be damaged (e.g., proanthocyanidin⬖ in DMSO blunted glyphosate’s testicular toxicity in male rats, preserving motility and testosterone and reducing DNA damage and oxidative stress1). The most extensively tested combination is curcumin,⬖ which protected against toxicity from cyclophosphamide,1 cisplatin,1 methotrexate,1 doxorubicin,1 cadmium,1 aluminum,1 cigarette-smoke1 and counteracted diabetic-induced hypogonadism1 (which triggers low testosterone, libido and bone density along with fatigue and erectile dysfunction). Additional DMSO-carried agents that protected the testicles against specific insults: hesperidin⬖1 and sulforaphane1 against radiation, thymoquinone⬖ against varicocele,1 fisetin⬖ against scrotal heat stress, 1, apocynin,⬖1 acacetin⬖ and MMINA against cisplatin,1,2 tert-butylhydroquinone1 and Pleurotus eryngii extract⬖1 against doxorubicin, myricetin,⬖ aucubin⬖ and resveratrol⬖ with naringenin⬖ against the endocrine disruptor nonylphenol,1,2,3 rutin⬖ against restraint stress,1 Spathodea bark⬖ against lead,1 Rhus tripartita⬖ against propylparaben,1 and olive leaf extract⬖1 against busulfan. Likewise a BET inhibitor JQ1 reversed inflammation-driven (LPS) spermatogenic dysfunction,1 and where testosterone itself protected Sertoli cells against palmitic-acid injury by restoring tight-junction proteins and antioxidant defenses.1 The Korean herbal formula Woogyuyeum,⬖ also protected Leydig cells from oxidative stress,1 and resveratrol⬖ improved sperm density, motility and testosterone in an aging model.1
Note: Like most antioxidants, DMSO’s testicular benefit is concentration- and timing-dependent. At very high doses (users are unlikely to reach) it has measurable toxicity to testicular tissue.1
DMSO is well tolerated by the testicle. Topically, DMSO gel applied to the scrotum twice daily for 54 days (1 g/kg) produced no significant change in seminiferous tubule morphology, tubule diameter, spermatocyte, spermatid or Sertoli cell counts, or spermatogenic yield versus saline.1 Injected directly into the testicle, pure DMSO did not alter seminiferous epithelium structure (and was specifically validated as a safe intratesticular infiltrating agent),1,2 2% DMSO injected into the testicle did not affect sperm count,1 and 4%1 and 0.5% intratesticular1 were likewise tolerated without effect on histology, hormones or sperm (and in another study where systemically toxic doses of DMSO were used, the testicular and epididymal tissue alone remained histologically normal1). Beyond these direct tests, a large body of studies used DMSO as the vehicle control while testing some other agent, and in every one the DMSO group was indistinguishable from untreated controls across testicular histology, testosterone, oxidative markers and apoptosis (demonstrating DMSO safety).1,2,3,4,5,6,7,8,9,10, 11,12,13,14,15,16,17,18,19,20, 21,22,23,24,25,26. The same held for sperm-level outcomes specifically: across studies where DMSO was the negative or blank control, it produced no change in sperm count, motility, viability, morphology, DNA integrity or acrosome function relative to untreated controls.1,2,3,4,5
Note: one of DMSO’s most popular uses is to preserve cells and tissues that are frozen (which is only possible due to DMSO’s low cellular toxicity). Extensive research explored DMSO’s use in preserving sperm, finding it preserved post-thaw motility, viability, membrane and mitochondrial function across an unusually wide range of species: human1,2 boar,1 buffalo,1 ram,1 rooster,1 and numerous fish, with even bee (drone) semen preserved.1,2,3 For human sperm, 10% is the practical optimum (while 20% is both least protective and most toxic1), and DMSO also extends the fertile window of cold (non-frozen) storage when combined with quercetin⬖1. Combining DMSO with antioxidants such as royal jelly⬖ or turmeric⬖ improves freezability and conception rates further.1,2
Infections (orchitis, epididymitis). In one of the original 1967 urological DMSO studies, 7 of 12 patients with epididymitis improved with topical DMSO.1 Dimexide (DMSO) has since been used, usually as a scrotal compress or application alongside standard antibacterial therapy, to treat orchiepididymitis and mixed urogenital infections, with reports of sufficient therapeutic effect and no adverse effects from the DMSO-containing dressings.1,2,3
Additionally, one reader described a painful left varicocele (enlarged scrotal veins) he had lived with from age 16 to 42, with pain he compared to the lasting ache of being kicked, persisting for 26 years; applying DMSO topically to the scrotum once or twice daily, he reported the pain subsiding within 15 to 30 minutes of the first application and then returning in progressively weaker and shorter waves with each successive dose (12 hours, then 24, then 48) until after one final application it did not return, and he reported the previously palpable “bag of worms” of enlarged veins had completely resolved.1
Improving fertility and virility. Beyond protecting the testicle, DMSO has been used to improve sexual and reproductive function, both through its own support of testosterone-producing cells and, more often, as a carrier that makes other agents work. Melatonin⬖ delivered in DMSO increased semen volume, concentration, motility and total sperm count while enhancing testicular blood flow over 60 days, correlating with higher steroid hormones.1 A transdermal iodine⬖ preparation carried in DMSO (”Iodon”), applied along the spine of iodine deficient breeding bulls, improved sperm quality across all parameters, sexual reflexes and fertility, raising thyroid hormones, gonadotropins and testosterone with no toxicity.1,2 Andrographolide⬖ in 5% DMSO enhanced sexual behavior and raised serum testosterone,1 and DMSO served as the delivery vehicle in numerous plant-extract studies (Citropsis,⬖ Caesalpinia⬖ and others) that improved testosterone, mating behavior and testicular histology.1,2 DMSO has even been used to electrophoretically drive hCG through the skin to treat cryptorchidism, achieving permanent testicular descent in fewer sessions than intramuscular hCG.1 It has carried a range of agents that improved sperm quality or testosterone synthesis: resveratrol⬖ restored motility and acrosomal enzyme activity in asthenozoospermic (low-motility) human sperm,1 IGF-1 raised testosterone in seminiferous tubules and reversed opioid-induced suppression,1 α-linolenic acid⬖ boosted testosterone production in Leydig cells,1 evening primrose oil⬖ increased testis weight, testosterone and mating performance,1 osteocalcin⬖ restored spermatogenesis and androgen signaling in azoospermic mice,1 and Sertoli cell transplantation raised sperm and testicular cell counts.1 Lastly the vas deferens itself propels sperm during emission through co-released norepinephrine and ATP driving its contractions, and in isolated-vas studies paclitaxel with DMSO strongly potentiated those contractions.1,2
Delivering androgens to the rest of the body. DMSO’s permeation-enhancing property has long been used to carry testosterone and other androgens across skin and into tissue. In humans it increased percutaneous penetration of testosterone and hydrocortisone roughly 3.5–4 fold,1,2,3 and it functions as a working vehicle for androgens across many routes: dissolving testosterone for transdermal and immersion delivery1,2,3, carrying testosterone enanthate for injection,1 and enhancing testosterone permeability as a drug-delivery additive,1 with DMSO-delivered testosterone reaching and acting on distant tissue such as the kidney,1 and serving as the vehicle for dihydrotestosterone in intratesticular studies.1 That systemic absorption is real enough that anabolic steroids dissolved in DMSO and applied produced the same testosterone and testicular suppression seen with conventional injected steroids,1 and it supported the differentiation of stem cells into testosterone-producing Leydig-like cells.1 Beyond merely delivering them, DMSO was itself therapeutic in several of these whole-body androgen models: as the vehicle for intra-articular DHEA⬖ in osteoarthritic rabbit knees, where the regimen reduced cartilage and synovial damage, lowered MMP-3 and aggrecanases, and raised protective TIMP, 1,2 and as the vehicle for DHEA in chronically stressed rats, where treatment restored body and adrenal weight and reduced cardiac and hepatic lipid peroxidation.1,2 DMSO-delivered DHEA likewise supported bone blood flow and density.1
Note: Because DMSO drives whatever it is mixed with through skin, this delivery property cuts both ways. Phthalate plasticizers (such as DEHP) and bisphenol A applied to skin in DMSO are carried in along with it, and these are testicular toxicants; it is sensible not to let DMSO contact plastics before applying it1 (though, in one study oral DMSO administered alongside oral DEHP actually reduced the resulting testicular atrophy by 14–17%1). Lastly, testosterone is not stable stored long-term in DMSO at room temperature, degrading substantially over weeks, so preparations must be made immediately prior to application.1
Hair regrowth. A primary driver of male baldness is DHT (a more potent form of testosterone) so finasteride, a drug which blocks its conversion to DHT has long been used to treat male baldness. As DHT is essential for male health, finasteride has a host of systemic side effects including severe sexual dysfunction, fatigue, cognitive impairment, anxiety and depression which can persist long after stopping the drug and create profound disability for some finasteride users. Since testosterone is converted to DHT at local sites throughout the body (e.g., the hair follicles), in addition to DMSO directly counteracting hairloss, DMSO coated liposomes have been used to facilitate the targeted delivery of finasteride to the hair, which effectively prevented testosterone induced hairloss while simultaneously avoiding the problematic systemic finasteride applications.1 Likewise, in a primate model of androgen-dependent baldness, DMSO carried the antiandrogen 4-MA into the scalp and successfully prevented follicle miniaturization (hairloss), while DMSO alone showed no effect.1 Separately, sulforaphane⬖ (delivered with DMSO as vehicle) promoted hair regrowth in mice by accelerating the liver’s breakdown of DHT, lowering circulating DHT, a different (less toxic) way to reduce DHT.1
Note: extensive evidence shows DMSO combats hair loss and many readers have successfully used it for this application (e.g., one man reported light brown hair growing in beneath his gray after about two months1).
Therapeutic germ-cell depletion (busulfan). DMSO is the standard solvent for busulfan when it is injected directly into the testicle to deplete endogenous germ cells in preparation for spermatogonial (sperm producing) stem cell transplantation. The intratesticular route, enabled by DMSO, causes far less systemic toxicity than intraperitoneal busulfan (near-zero mortality vs. up to ~40%), achieves complete germ-cell depletion, and restores fertility with donor-derived offspring.1,2,3,4 In every case the DMSO-only arm preserved normal testicular histology, confirming the depletion was the drug’s effect rather than DMSO’s and that DMSO is safe for the testicles.1,2,3
Cancer: in addition to protecting testicular tissue from cancer radiation therapy, it has also demonstrated specific utility in male cancers. These include it delivering ethanedimethanesulfonate (which necrotized spontaneously-occurring testicular Leydig cell tumors in old rats in 78% of tumors examined),1 and the androgen DHEA⬖ which suppresses pancreatic cancer (and leukemia cell growth).1,2 Likewise, DMSO’s ability to differentiate stem cells into essential tissue and cancer cells into less-cancerous (or non-cancerous) cells have been used differentiate a testicular choriocarcinoma line (raising hCG secretion and inhibiting proliferation)1 and to push stem and progenitor cells toward spermatogonial and other reproductive lineages.1
Note: while DMSO generally enhances the potency of chemotherapy, some studies show its affinity for platinum causes it to reduce the potency of platinum containing ones, and in one study, DMSO induced up to roughly 3-fold resistance to cisplatin in human testicular embryonal carcinoma lines.1
Scrotum (trauma and topical use). DMSO’s therapeutic properties have been repeatedly shown to reduce skin injury and heal injured skin (detailed here), and when tested, also were demonstrated in the scrotum. In a reviewed series of childhood testicular trauma, topical DMSO applications were used as part of conservative therapy for scrotal injuries and testicular contusions,1,2 and a 25% DMSO solution in twice-daily dressings was used on the scrotum after surgery for a complicated hernia, with serous drainage stopping by the second day and primary wound healing.1 For scrotal hematoma, a DMSO-plus-heparin gel (Dolobene) helped clear the collection within about ten days.1 In a one case, a man developed a painful chemotherapy extravasation injury of the scrotum (after mitomycin C); topical 60% DMSO relieved the pain and visibly reduced the redness within seven hours of the first application.1
Likewise, one reader shared his brother developed fluid, inflammation and swelling of the right testicle (without pain) following a hernia repair operation, and after spraying on DMSO with castor oil the testicle returned to its regular size.1
Reversible Male Birth Control
The most developed application of DMSO in this area is as the solvent that makes a reversible “vasectomy” possible. The contraceptive itself is a polymer, styrene maleic anhydride (SMA), dissolved in DMSO forms an injectable gel marketed as RISUG. Injected into the vas deferens, the SMA-DMSO complex forms a charged, porous coating that partially occludes the vas and disrupts passing sperm by lowering local pH and destabilizing the sperm membrane, producing azoospermia (ejaculate missing sperm) without stopping sperm production.1,2,3,4,5,6
This preparation is reversible because flushing the vas with DMSO dissolves the polymer plug back out, restoring anatomical patency (opening), full regeneration of the vas lining, and normal spermatogenesis.1,2,3,4,5 In animal models DMSO reversal restored 100% fertility with healthy offspring and no genotoxicity, and the interval to reversal can be tuned (from about three months to several years) by varying the SMA dose.1,2,3,4,5 Relatedly, DMSO appears able to help restore obstructed reproductive ducts: on the female side it has been used successfully to treat tubal-obstruction infertility1,2,3,4 (with one protocol being successful in 75–85% of cases1), and recently, when a colleague asked for help in restoring fertility after reversal of a longstanding vasectomy, he fathered a child following the DMSO protocol I suggested.
In humans, the SMA-DMSO injection has passed through Phase I–III trials in India: a single injection produced azoospermia (84% within two months, with most subjects sterile by 60–70 mg doses), provided contraceptive protection for many years (up to a decade or more), preserved libido and sexual function, and caused only mild transient scrotal swelling in some men.1,2,3,4 Long-term human and primate safety data found no effect on the prostate (normal seminal citrate even after 8 years), no systemic toxicity at up to five times the contraceptive dose in monkeys, and no teratogenicity in offspring conceived after reversal.1,2,3,4,5,6 The bulk of the supporting toxicology spans rats, rabbits, langur and rhesus monkeys, and human volunteers, consistently attributing safety concerns (where raised) to the SMA constituents rather than to DMSO.1,2,3
A related hydrogen-releasing hydrogel (HFMC) works on the same principle, killing sperm by altering vas pH and reversing once DMSO dissolves it out, with toxicology in mice, rats and rabbits showing no deaths, organ changes or genotoxicity.1 Two variations on the RISUG concept have also been explored: a “smart” version incorporating iron-oxide and copper particles that can be activated by a pulsed magnetic field to cut sperm count and motility on demand,1 and a proposal to use the same vas implant to inactivate HIV in semen and reduce sexual transmission.1
However, not every polymer is DMSO-reversible. Uryx, an ethylene vinyl alcohol polymer also dissolved in DMSO, reliably produced azoospermia in rabbits but could not be flushed back out with DMSO, and DMSO injection after Uryx increased inflammation; the reversibility advantage is specific to the SMA and HFMC systems.1,2
Note: DMSO has separately been used to transport agents that sterilize animals. Many such as calcium chloride (cats and bulls),1,2,3 zinc gluconate (dogs and pigs),1,2,3,4 chlorhexidine (in dogs and bulls)1,2,3,4,5 and CBD (guinea pigs),1 were used to destroy the sperm-producing or sperm-storing tissue directly through intratesticular or intra-epididymal injection. Others permanently plugged the vas deferens or spermatic cord by scarring the tube shut.1,2,3 Finally subcutaneous coumestrol1 and sulfapyridine2 have also been used to non-invasively reduce fertility.
Penile Conditions
DMSO has been applied to most of the conditions that affect the penis, with the same therapeutic properties seen elsewhere benefiting this organ too.
Erectile dysfunction. Many readers have reported DMSO benefitted erectile dysfunction including men not looking for it. One 75-year-old reader with no history of ED, applying large topical doses of DMSO across his sacral area and hips for severe spinal stenosis pain, described an unexpected and pronounced erection two to three minutes after application with no sexual stimulation involved; he attributed it to DMSO’s enhancement of blood flow and possibly to relief of the nerve impingement affecting his pelvic region, and noted the effect recurred reliably whenever he used a larger volume.1
Multiple other readers independently reported reversing long-standing erectile dysfunction (including ED from from using statins1,2)—which in several cases was present for fifteen to twenty-five years after applying topical DMSO, several of them having started it for foot pain and reasoned that its circulatory benefits might extend to erectile function; most described starting at 50-70% to limit irritation and seeing improvement within a week or two.1,2,3,4 One couple in their late fifties and sixties described resolving two problems at once: the wife applied DMSO to perineal scar tissue from old episiotomies that had made postmenopausal sex painful and reported the scarring healed, and when her husband subsequently developed ED he massaged a DMSO castor oil mixture on himself into the same area daily for about a month, after which they reported their sex life restored.1
The most direct evidence comes from DMSO relaxing the smooth muscle of the corpus cavernosum, the central event in an erection (as the cavernosal muscle relaxes, the penis fills with blood and becomes engorged). In isolated human corpus cavernosum strips precontracted with phenylephrine, DMSO produced dose-dependent relaxation beginning at very low concentrations (from around 10⁻⁹ M) and reaching roughly 29% maximal relaxation.1,2 A separate study found that at higher concentrations DMSO abolished resting tension entirely.1 Because DMSO is so readily absorbed through skin, the concentrations that relax this tissue hence are easily reached by topical application to the penis.
That relaxant effect compounds when DMSO carries an erectogenic agent, and because DMSO relaxes the tissue on its own, the benefit credited to each agent is measured against DMSO’s own baseline (meaning part of the shared effect is likely DMSO’s). As a 50% vehicle it potentiated sildenafil’s (Viagra’s) relaxation of cavernosal smooth muscle many times over (roughly 16- to 80-fold),1 and in men with erectile dysfunction unresponsive to PDE5 inhibitors like Viagra, DMSO both relaxed corpus cavernosum directly and potentiated the relaxation from guanylyl-cyclase-targeting drugs.1 Testosterone (which, as covered in the testicle section DMSO independently raises) dissolved in DMSO produced a rapid, dose-dependent relaxation of erectile tissue from men with ED, reaching 41-71% (greatly exceeding DMSO alone).1,2,3 DMSO has also served as the vehicle across a wide range of other agents shown to relax erectile tissue or restore erectile function: the PDE inhibitor BAY 73-6691 (which amplified and prolonged nitrergic relaxation),1 the Rho-kinase inhibitor Y-27632 (which relaxed tissue from men with severe ED and was additive with Viagra’s cousin vardenafil),1 chloride-channel blockers (which raised intracavernosal pressure in living rats),1 and icariin⬖ (horny goat weed), which in diabetic rats restored erectile hemodynamics, preserved smooth-muscle and endothelial content, and downregulated the profibrotic TGFβ1/Smad2 pathway.1,2 Beyond erectile tissue specifically, DMSO has been the vehicle for nitric-oxide-releasing nanoparticles that induced spontaneous erections in a post-prostatectomy rat model1 (a situation that commonly causes incontinence) and patented for topical use carrying papaverine (with or without nicotinic acid): submerging the penis in the warmed DMSO-papaverine solution under mild vacuum restored erections adequate for intercourse in all 20 men under 50 and 72% of those over 50.1 Camphor-dimexide rectal preparations have likewise been patented for impotence (among other prostate conditions),1,2 and a patented topical preparation combined DMSO with local anesthetics and botanical extracts to prolong intercourse and reduce premature ejaculation.1
Note: DMSO’s relaxant effect on erectile tissue is also seen in the channel-activator URO-K10, developed (with DMSO as solvent) to open Kv7.4/7.5 potassium channels and relax both corpus cavernosum and prostate smooth muscle for ED and lower urinary tract symptoms.1 DMSO has also been the vehicle in numerous other successful cavernosum-relaxation studies (adenosine/ATP A2B-receptor work, heme-oxygenase signaling, and cannabinoid-related NANC relaxation),1,2,3 and for evening primrose oil, which raised penile prostaglandin and testosterone and improved mating performance.1 The relaxant effect is genuine but concentration-dependent: in one rabbit study using an unspecified (likely low) concentration, DMSO showed no relaxation,1 consistent with the threshold seen in the human-tissue work above.
A second route to improving erections is indirect, by treating the chronic prostatitis that so often causes or worsens ED. As covered in the prostate section, DMSO-based local regimens for chronic prostatitis repeatedly improved erectile function as a secondary benefit (for example raising normal-erection rates to 58-72% versus 41% in controls, and improving ED scores more than antibiotics alone).1,2,3,4 The historic DMSO literature noted the same: one early account reported DMSO let men resume intercourse where pain or urethral blockage had previously made it impossible.1 And in a 1981 study, a urethral-dialysis regimen using 10% DMSO (with novocaine and calendula) in 24 men with chronic prostatitis, vesiculitis or urethritis resolved the inflammation and restored libido, erection, ejaculation and orgasm in all of them, versus 13 of 20 controls on standard therapy.1
Note: DMSO’s relaxant effect on the pelvic floor likely contributes here too. As covered in the prostate section, intravaginal DMSO measurably relaxed the levator ani muscles in women; men have the same pelvic-floor musculature, whose spasm and hypertonicity can compress the arteries and nerves supplying the penis and contribute to ED.1
Peyronie’s disease. This is the penile condition with DMSO’s deepest record. In Peyronie’s, fibrous scar plaques form within the tunica albuginea (the penis’s outer sheath), causing curvature, shortening, pain and (because the plaques obstruct blood flow into the penis) erectile dysfunction. It is estimated to affect anywhere from 0.3% to 16% of men (estimates range widely because men are reluctant to report it), and every conventional option is unsatisfactory: traction therapy demands hours a day for months, ED drugs (while somewhat alleviating) do nothing for the plaque, collagen-dissolving injections help only about half of patients, and surgery creates more scarring.
Note: Peyronie’s matters for ED even when it is subclinical (not yet causing visible curvature or palpable plaques). In a study of 386 men undergoing Doppler ultrasound for ED or penile pain without curvature, about 10.6% had detectable Peyronie’s plaques, 73% of whom had ED as their main complaint and about half of whom showed reduced blood flow past the plaque,1 and other studies have similarly found elevated ED rates in men with subclinical Peyronie’s,1,2 so DMSO’s plaque-dissolving action may help a subset of ED that has no obvious external cause.
Because DMSO dissolves scar tissue (and offers a non-embarrassing way to treat the condition at home), the DMSO field recognized early that it could help here. There is also mechanistic support for this: DMSO downregulates type I and III collagen gene expression in human fibroblasts (the cells that build the plaques), with half-maximal inhibition around 2% and low toxicity at that level,1 and it strongly represses stromelysin-1 (MMP-3), an enzyme that drives the aggressive matrix remodeling underlying Peyronie’s, Dupuytren’s contracture, keloids and other fibroses.1
Note: the same scar-dissolving property is why DMSO helps Dupuytren’s contracture, the hand-fibrosis condition that is essentially Peyronie’s of the palm.
Clinically, the early reports were promising: across the original urological DMSO studies, topical DMSO improved roughly half of Peyronie’s patients (6 of 13 in one series, and softening or resolution of 2 of 4 patients’ plaques in a separate preliminary report).1,2,3 DMSO combined with prednisolone was also developed as a local Peyronie’s treatment in the 1970s.1,2 Larger combination regimens built on this. In 66 men treated with topical 50-70% DMSO daily over 20 sessions (alongside other conservative agents), plaques shrank in 72.7%, dissolved completely in 18.1%, softened in 43.9%, curvature improved in 37.9%, erectile function improved in 42.4%, and pain resolved in most.1,2 In a long-term protocol centered on topical 50-70% DMSO rubbed into the plaque twice daily, 5 of 6 evaluable patients fully recovered with no recurrence over 2-4 years and the sixth stabilized with restored erectile function.1 Another multimodal series of 41 patients including topical 20-25% DMSO reported pain relief in 54%, improved sexual activity in 38%, and plaque/curvature reduction in 40%.1
DMSO has been also been used in numerous other publications to treat Peyronie’s,1,2,3 often combined with agents such as verapamil, lidase, longidaza, steroids and vitamin E within multimodal regimens,1 and DMSO appears in the standard reviews of Peyronie’s treatment options.1
Conversely, it must be emphasized that like Dupuytren’s and cutaneous amyloidosis, DMSO is not always effective (e.g., the figures I cited above showed it helped Peyroine’s about half the time, an older work noted DMSO gave only “so-so” results,1 and several multimodal series where DMSO was one component of complex therapy reported overall conservative efficacy in roughly 15-30% of patients, with plaques persisting in most and many eventually needing surgery1). Because of this, DMSO is best suited as a “conservative treatment” which is worth trying in the hope that it works (given its low cost, safety and the issues associated with other options for Peyronie’s) rather than something which can be definitely relied upon. That said, Stanley Jacob discovered combining DMSO with one forgotten (but still available) antifibrotic agent—which was ineffective on its own—significantly increased treatment success in Peyronie’s, scleroderma and Dupuytren’s.
Note: topical DMSO has also been utilized for localized urethral amyloidosis.1
The same scar-dissolving action likely also extends to other post-surgical scarring near the reproductive tract. For example, one 69-year-old reader described sharp pain on ejaculation that had persisted for eight and a half years after hernia surgery, which his physicians attributed to scar tissue that had regrown around the vas deferens; while using DMSO for unrelated knee pain, he reported the ejaculation pain disappeared completely, and he specifically noted this occurred more than eight years after the operation, contrary to the expectation that DMSO must be applied soon after surgery to affect scar formation.1
Priapism. In priapism, blood becomes trapped in the engorged penis and cannot drain, which is a medical emergency that can permanently damage the tissue, and which is difficult to treat given the area. DMSO’s ability to improve stagnant blood flow and reduce inflammation suggested a role, and in a 1966 case report DMSO rapidly improved and within a week fully resolved a postinfectious circulatory priapism in an 11-year-old boy after other treatments had failed.1,2 Intravenous DMSO has also been used in the postoperative management of priapism in horses, to reduce inflammation, promote venous drainage and limit ischemic injury.1,2 (although in one case it was not successful1).
Note: this same ability to improve stagnant blood flow and drainage in the corpora cavernosa complements DMSO’s direct relaxation of cavernosal smooth muscle, providing additional mechanistic support for DMSO’s potential in vasculogenic or inflammation-related ED.
Infections. DMSO has demonstrated consistent efficacy against herpes, however while most published reports suggest efficacy for male genital herpes, specific outcomes are rarely provided. For example, in an early study where DMSO was used to treat five patients with genital herpes,1 patient genders were not provided, and when one (now deceased) author reported that DMSO allowed four patients in genital herpes to have sexual intercourse after only two days of treatment,1 gender also was not specified (although it is more probable that description summarizes male cases).
In addition to DMSO being used alone for herpes, it has also been combined with other agents, one of which, the antiviral idoxuridine (ineffective on its own since it could not penetrate the skin) was shown in numerous clinical trials (typically at 5% in combination with DMSO) to effectively treat herpes and shingles (leading to an approval in Europe but not the United States). For genital herpes:
•In one report, DMSO-idoxuridine rapidly improved necrotizing herpetic balanitis (a severe herpes complication in the penis).1
•DMSO-idoxuridine shortened viral shedding in genital herpes across several controlled trials, though concentration matters (high-concentration idoxuridine in DMSO can macerate the thin genital skin).1
•In one trial of men and women with recurrent genital herpes, DMSO-interferon caused 66% of lesions to be culture negative within 24 hours, while DMSO alone did so for 25% (along with subsequently eliminating the lesions and preventing recurrences), however like other trials, the exact breakdown was not provided.1
DMSO has also shown promise for challenging HPV genital warts:
•A German author reported success treating them with Verrumal (a DMSO mixture sold in Europe, Asia and the Middle East containing 5-fluorouracil and salicylic acid).1
•In the 1970s (when treatment for anal and genital warts was disfiguring), a cancer surgeon, appalled at the situation developed a treatment that used DNCB to stimulate an immune response against warts and cancers, noting in a 1975 publication that DMSO enhanced the treatment,1 and in a 1978 trial of 23 patients with treatment resistant genital warts, noted that all but 1 improved from the DNCB immunotherapy1 (but did not specify if DMSO was used here too). Commenting on his work, Pat McGrady stated Moore’s DMSO-containing therapy worked so well in homosexual condyloma patients that demand reportedly overwhelmed the hospital.1
Note: given that DMSO increases the immune response to topical allergens, it is plausible it would enhance topical immunotherapies, but this area remains unexplored.
Likewise, one reader reported that a 3 by 4 cm patch of condylomata acuminata on the shaft of the penis, which he had struggled to clear for months, began visibly resolving after only four or five applications of DMSO from a roller applicator and became nearly flush with the surrounding skin, with no further applications needed.1
Additionally:
•In bulls, DMSO combined with an antibiotic healed ulcerative inflammation of the prepuce (foreskin) that had resisted standard treatment.1
•In foreskin-fibroblast models DMSO has also served as the vehicle for antiviral agents: a liver-X-receptor agonist that cut cytomegalovirus titer more than a thousandfold.1
•A cigarette-smoke concentrate in DMSO inhibited Kaposi-sarcoma herpesvirus entry into foreskin-fibroblasts.1
Cancer and tissue protection. DMSO has carried chemotherapy into penile cancer (bleomycin dissolved in DMSO alongside laser hyperthermia and radiation),1 and topical DMSO contributed to complete regression of a malignant histiocytoma on the prepuce of a dog.1 It is also a recognized antidote for the tissue necrosis caused by chemotherapy extravasation: as covered in the testicle section, topical DMSO relieved the pain and redness of a mitomycin-C extravasation injury, and it is noted as a topical antidote for mitomycin-induced necrosis of the glans.1
Other uses. A 2008 randomized trial found that using DMSO in place of lidocaine as the lubricating gel for cystoscopy (which passes a probe through the penis to reach the bladder) halved the pain score reported after the procedure.1
Safety. Like the testicles and prostate, a lack of toxicity to the penis was observed across the DMSO studies performed (e.g., DMSO injected directly into the penile bulbocavernosus and ischiocavernosus muscles as a tracer vehicle caused no adverse effects1). The only potential issues observed came from the use of higher concentrations of idoxuridine (which produced premalignant skin changes that healed once treatment stopped1) and an unusual lymphoma case not otherwise reported in the literature.1
Female Reproductive Tract
Numerous studies have shown DMSO heals each part of the female reproductive tract and restores fertility.
Ovaries
DMSO has repeatedly been shown to protect the ovaries from lethal stressors:
•When rats had the blood supply to one ovary cut off for 3 hours (by simulating an ovarian torsion), DMSO given 30 minutes prior to reperfusion significantly reduced the resulting oxidative stress and tissue damage.
•Ovarian cells (from Chinese hamsters), were protected from lethal hyper-osmotic injuries by 5 and 10% DMSO. Some of these protective effects were a result of DMSO reducing an otherwise lethal sodium and potassium ion fluxes and (shown via electron microscopy) preventing the surface changes in their membranes which preceded death.1,2,3
•DMSO reduced the sensitivity of Chinese hamster ovary cells to ethidium bromide (a DNA mutagen) by decreasing intracellular of it by reducing its ability to enter the cells (which is quite noteworthy as typically DMSO increases the uptake of chemicals).
Note: When DMSO was microinjected directly into the ovarian bursa of cyclic female rats, no toxicity or adverse effects on ovulation were observed. DMSO, in turn, has been used as a vehicle to deliver medications to the ovaries and to successfully replace missing sexual hormones in rats who could not produce them.
Additionally, in a rat model of polycystic ovarian syndrome (PCOS), DMSO improved metabolic markers of the disease (e.g., fasting hyperglycemia and 2-hour glucose levels) and reduced the associated oxidative stress.
Fallopian Tubes
•A 1975 Chilean study at a Navy hospital took 69 women who were infertile due to an obstruction in their fallopian tubes and injected a DMSO mixture into their fallopian tubes via ascendent hydrotubation (the specific mixture was 5ml of DMSO, dexamethasone, and chlorpheniramine diluted in 20 ml of distilled water). A series of 6 DMSO hydrotubations was given (every 3 days) followed by temporary breaks of varying lengths, and then an evaluation to determine if the tubes had opened. Once the tubes were opened, the patient was instructed to lead a normal sex life, and then repeat the hydrotubations if they had not gotten pregnant.1,2
The authors reported carrying out a total of 426 DMSO hydrotubations in 69 patients, of whom 47 were available for analysis at the time the article was published. Of those 47, 27 (57.4%) subsequently became pregnant, including one who got pregnant twice (without any further assistance). Of the 27 pregnancies, 12 resulted in successful deliveries, 7 had a normal pregnancy at the time of publication, 4 patients chose to have abortions, and 3 had spontaneous abortions, and 1 had an abnormal pregnancy requiring a surgical intervention, and 0 had ectopic pregnancies (one of the risks of surgically opening the fallopian tubes). Additionally, in the 426 DMSO hydrotubations, 4 experienced discomfort and fatigue during the procedure, and 2 had psychiatric changes (in one case a sensation of anguish with difficulty breathing and in the other hypothymia and psychomotor agitation). These rare side effects (occurring in 1.5% of intubations) did not require suspending the treatment, and did not increase overtime.
Note: 25-35% of infertility is due to tubal obstructions (typically from inflammation there). The current surgical approach for opening a tubal obstruction and restoring fertility (which bears some risks) has a 10-30% success rate (figures on this vary widely, but are almost always under 50%).
•In a Russian study, DMSO with Trichopol effectively treated inflammatory tubo-ovarian formations (e.g., abscesses and cysts).
Uterus
•This horse study and this horse study) found that applying DMSO directly into the uterus does not harm its lining (the endometrium) or trigger fibrosis.
Note: there are many studies showing DMSO prefers the function and structure of tissues that get frozen (e.g., this one of a horse’s uterine lining).
•In 43 mares with clinical or subclinical endometritis, compared to saline, intrauterine 30% DMSO was found to reduce inflammation, alter or eliminated uterine microbial load, improve fertility. Additionally, DMSO reduced the excessive uterine vascularization provoked by this inflammation—suggesting a potential utility in the treatment of endometriosis.
•One study administered 10-30% DMSO into the uteruses of horses that could not get pregnant. It found no harm occurred to the lining of the uterus and that 18 out 27 had significant improvement to the lining of their uterus (compared to 2 out of 18 who received a saline placebo), such as a reduction of chronic inflammatory cell infiltrates and reduction of periglandular fibrosis. Additionally, there were signs their fertility improved, but the trial's design made it impossible to be sure this improvement occurred.
Note: these results suggest administering DMSO directly into the uterus could help a few challenging gynecologic conditions, but I do not know of any researchers who have tried this approach. However, I did receive this comment from a reader.
I have been suffering from endometriosis pain since I was 13. I am now 43 and I have tried everything other than surgery. Including a progestin IUD from my gyno that almost killed me (seriously). After giving up on mainstream medicine 3 years ago, I started using bio identical progesterone after reading Dr. Mercola's articles. The progesterone did help with some of the pre menstrual pain but I was still struggling with mid cycle pain, menstrual pain and horrendous inflammation of the endometrial tissue. I started using DMSO 70% topically and then a couple doses orally (1tsp) spaced a week apart. I quickly noticed the reduction in inflammation, cramping and pain. I had no mid cycle pain or PMS for the first time since I was last pregnant. Also, for the first time in years, I did not have to take any medication during my cycle for pain or inflammation. The cramping/inflammation I usually experienced was debilitating but the cramping I had was painless and more like a warm pressure. Truly incredible. I will continue my regimen but I am curious to see if this is a cure or an ongoing treatment I will need to maintain. Thank you Midwestern Doctor for your research and voice.
P.S. Added positive side effects I have experienced: less joint pain and quicker recovery after exercise. No blister or pain after applying DMSO to a small burn from cooking.
Note: DMSO is used by protcologists and gynecologists in Russia.
Cervix
•In women with habitual miscarriage and chlamydia cervicitis, cervical electrophoresis with DMSO and chymotrypsin, combined with magnetic laser therapy and vibroaspiration, enhanced immunity and increased successful pregnancy outcomes by 16.3% compared to standard treatment.
•A Russian study found DMSO could be used to treat erosion of the cervix.
•In sheep, DMSO was found to enhance the activity of enzymes which ripen the cervix, thereby facilitating artificial insemination.
Vaginal Canal
•A study gave 75 women with chronic genital inflammation or neurogynecological conditions, intravaginal tampons with DMSO and 6% novocaine. In those with inflammatory conditions, this significantly alleviated pain and inflammation and normalized pelvic diaphragm muscle bioelectric activity, reducing its amplitude by 36% (whereas no significant improvement was seen in the neurogynecological group)—indicating this combination could be extremely helpful for the muscle spasms associated with these conditions.
A New Therapeutic Principle
When DMSO was discovered, Stanley Jacob quickly realized that it represented a new therapeutic principle since it made so many things which had previously seemed impossible in medicine suddenly possible—and even more remarkably, 60 years later, many of the things DMSO can address still remain a perpetual challenge for the current medical paradigm. As such, I find it remarkable that in the brief time DMSO was in widespread use and being researched worldwide, so many different uses for it that are still just as applicable today were discovered.
For example, much in the same way I recently showed how DMSO could significantly improve surgical outcomes, the data here makes good case that DMSO should be a mainstay therapy whenever someone is at risk of organ failure from being poisoned (e.g., due to a drug overdose). Likewise, the data here shows how numerous immensely challenging diseases that require a hospital or intensive care admission could be dramatically improved with DMSO.
However, while this stonewalling is immensely unfortunate, I am extremely hopeful that we will soon see a paradigm shift on this issues as:
•Much of the public (and much of the medical profession) has lost faith in the medical orthodoxy’s verdict on what does and does not work.
•Twitter (𝕏) now allows the rapid diffusion of information, making it impossible to censor the medical truths the public is craving.
•The incoming administration (particularly RFK Jr.) are strongly committed to this issue.

As such, my goal is now transitioning to trying to support this paradigm shift.
Protocols
In the final part of this article, I will discuss how DMSO can be used to treat the conditions listed throughout this article (e.g., cirrhosis, prostate enlargement, GI ulcers, ulcerative colitis), along with a few other integrative approaches we use for those conditions (e.g., for ARDS, heart attacks, gallstones, gastric bleeds, and smoke inhalation). Additionally, I will also provide a revised set of simplified instructions for the product sourcing and general use of DMSO (as I’ve received a lot of useful feedback over the last few weeks that has provided some important hints for ensuring safety). Finally, I recently updated this article to include all the detailed information for male sexual health protocols (e.g., prostatitis, BPH, erectile dysfunction, Peyronie’s disease) along with key therapeutic combinations for these conditions including a forgotten remedy which effectively treats many fibrotic conditions and instruction for rectal applications of DMSO.
