How DMSO Treats "Incurable" Autoimmune and Contractile Disorders
The decades of research that could have prevented an immense amount of human suffering

Story at a Glance:
•DMSO is a remarkably safe substance that effectively treats a variety of conditions (e.g., chronic pain, acute injuries, and strokes) that medicine has struggled with for decades. Many readers here have already experienced profound benefits from using it.
•DMSO is a powerful (but safe) anti-inflammatory agent that is often extremely helpful for autoimmune conditions. For example, it’s frequently used to treat asthma, inflammatory bowel diseases (e.g., ulcerative colitis and irritable bowel syndrome), interstitial cystitis (painful bladder syndrome), ITP, lupus, multiple sclerosis, myasthenia gravis, scleroderma, Sjogren's syndrome, and uveitis.
•DMSO is also remarkably effective at stabilizing and refolding proteins. This allows it to treat a variety of “untreatable” genetic disorders, and conditions characterized by the abnormal accumulation of misfolded proteins in the body (e.g., amyloidosis) or chronic deposits of excessive contractile collagen (e.g., surgical scars, abdominal adhesions, Dupuytren’s contractures, and Peyronie’s disease). Two of the most dramatic examples of this are scleroderma and fibrodysplasia ossificans progressiva—both “untreatable” conditions where DMSO can provide truly lifesaving benefits.
•In this article, I will present the wealth of evidence substantiating each of those uses, share my theory on how the unusual antimicrobial properties of DMSO explain some of these benefits, and present DMSO treatment protocols for many of those disorders. Additionally, since many readers requested it, I put together a simplified guide on how to use DMSO orally or topically.
Note: over the last few days, I switched my focus to preventing an immensely unjust execution in Texas that shed light on how parents are often falsely accused of killing their babies after a vaccine death. Thanks in part to all of you speaking out, a miracle happened, the right people noticed (I can’t disclose what happened behind the scenes but consider this Tweet RFK Jr. put out which referenced a post referencing the article here) and a series of unprecedented actions happened to delay and possibly overturn an execution (which in reality was due to a baby dying from clearcut case of medical malpractice). This case still needs a great deal of support, so if you can contact either the governor (here) or the Texas legislators trying to overturn this (here and here) that would be immensely helpful.
Dimethyl sulfoxide (DMSO) is a simple and readily available naturally occurring chemical that rapidly enters the body through the skin and has a variety of remarkable therapeutic properties. When it was discovered, its proponents believed it (much like antibiotics) represented a new therapeutic principle in medicine and once adopted, would completely change how medicine was practiced. Unfortunately, the FDA conducted a reprehensible campaign against it and was able to successfully bury it.
Since there are so many uses for DMSO, to effectively present them, I’ve had to comb through well over ten thousand pages of scientific literature and then order them into a logical sequence (of what will be roughly a nine-part series). For instance, in the first part of this series, I discussed how DMSO completely changed the management of neurological injuries and showed that were it to be adopted, millions would no longer be disabled from the common emergencies we view as insurmountable within the current medical paradigm (e.g., frequent disabilities from stroke and the inevitability of becoming a paraplegic after a spinal cord injury).
In turn, after I posted this, I began to receive testimonials from readers who’d found DMSO treated neurological and circulatory disorders they had always thought could not be treated.
In the second part of this series, I discussed how DMSO is remarkably effective for treating injuries and chronic pain:

In turn, after I published this article (since those conditions are some of the most common things people struggle with), I received a lot of comments from readers who expressed their understandable skepticism something like this could actually exist (which is part of why I began this with the wealth of evidence DMSO was paradigm shifting in neurology). At the same time, many were encouraged to try it, and I received numerous testimonials of the astonishing recovery it facilitated from a significant injury they’d suffered since the article had come out. More importantly however, many readers with chronic pain (or immobility) decided to try it, and were overjoyed to discover that after years they could at last get their lives back.
Taking a step back, the fact that something this effective could exist no one knows about is difficult to believe, which in turn suggests there has to be a reason for why no one knows about it—such as DMSO being extremely toxic. In reality, it is purely politics, and to support that, I compiled a detailed article summarizing everything that is known about the safety and toxicity of DMSO, which in my eyes, made the case that DMSO is one of the safest pharmaceutical products in existence and that the widely used alternatives to it (e.g., NSAIDs) are incredibly dangerous and orders of magnitude more harmful than DMSO.
Note: while publishing this article, I realized there was a human study demonstrating its safety in pregnancy (where DMSO was successfully used to treat infertility) that I forgot to include and have now added to the previous article.
Now that I’ve established there is something truly remarkable to DMSO (e.g.,you can read the hundreds of testimonials I’ve received from readers here), I would like to focus on another area where DMSO upends the existing medical paradigm—autoimmune and severe connective tissue disorders. I believe this is necessary because many individuals suffer from autoimmune and contractile conditions, but more importantly, because some of the conditions DMSO has been shown to treat effectively are otherwise death sentences that for decades the medical community has made almost no progress addressing.
DMSO and Protein Disorders
One of DMSO’s remarkable properties is its ability to function as a chemical chaperone and stabilize the three dimensional structure proteins assemble (fold) themselves into. This is important as many complex illnesses (e.g., many genetic disorders) result from misfolded proteins and presently can only be (ineffectively) managed with expensive drugs that aim to normalize the function of the abnormal proteins.
In turn, a few drugs have been developed to refold misfolded proteins, and to my knowledge, the most helpful ones on the market were the ones developed to treat cystic fibrosis (after the Cystic Fibrosis Foundation gave 150 million to bring these medications to market which currently are priced at roughly 300,000.00 a year). However, unlike the existing pharmaceutical chaperones (which are very specific to the misfolded protein), DMSO’s effect is remarkably universal.
Note: improving the physiologic zeta potential (as explained here) can also stabilize protein folding (while worsening it causes aggregation and misfolding). Likewise, DMSO has been shown to dissolve numerous enzymes without irreversibly inhibiting them, which authors felt suggested DMSO could compensate for genetically defective enzymes.
Studies have shown DMSO can improve the functionality of the dysfunctional proteins that are seen in genetic disorders like cystic fibrosis,1 hereditary nephrogenic diabetes insipidus,1,2 Machado-Joseph disease,1 Niemann–Pick disease,1,2,3,4,5,6 and a defective protein that causes motor disorders and early death in mice.1 Likewise, it can also treat a variety of complex diseases which result from misfolded proteins damaging surrounding tissue.
For example, amyloidosis is a challenging condition that results from aggregates of insoluble proteins accumulating in the surrounding tissues. DMSO in turn has been shown to solubilize the amyloid aggregates and enabling the body to break down and eliminate them (e.g., one study tested 125 Bence Jones proteins and found that DMSO prevented their conversion to amyloid fibrils and stopped most of them from precipitating). As a result, at least 40 studies and case reports have shown that DMSO can treat numerous types of amyloidosis.1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37. 38, 39,40
Likewise, DMSO has also been shown to revert the protein responsible for the devastating neurological prion diseases Creutzfeldt-Jakob disease1 and scrapie1 (which suggests it could also be helpful for mad cow disease).
Note: the previously mentioned studies are discussed in more detail here.
Presently, numerous human studies have shown that DMSO can treat amyloidosis, and one showed that it treated Neiman-Pick’s disease. Additionally, DMSO in this and this animal study and in this human study has been shown to treat Alzheimer’s disease, another condition linked to misfolded proteins (along with another one where adults with a variety of different degenerative brain conditions were treated). Likewise, we’ve clinically observed Parkinson’s (another disease that can be linked to misfolded proteins) responds to treatment with DMSO, and recently, one reader here reported:
I ordered DMSO immediately after your first article appeared. I am now in the 4th week of testing DMSO for Parkinson's disease. [The initial dose I took was too high so I stopped] On the second day of the break my Parkinson's symptoms almost disappeared and I felt better than I had felt for ages. The biggest improvement was in relief from bradykinesia. After being slow for the past years, I suddenly became Mr Speedy. At [a lower] dose I get minor brain fog for about one hour and the benefits of DMSO for the rest of the day.
In terms of symptom response to DMSO, in these first 4 weeks, pain, speed and the range of movement were most improved, followed by stiffness. Tremor seems to take more time to respond but there are already subtle signs of improvement. I and my family have also noted improvements in a whole range of other symptoms: brighter facial expression, eye comfort (more irrigation), stronger voice, more energy, better left/right hand coordination (fewer typing errors when using computer keyboard) and improved handwriting. Most importantly, I have periods of feeling really good which were previously absent. I have no doubt that DMSO is doing something good.
Note: since many cancer causing proteins are misfolded proteins, it is thought that this may partly explain DMSO’s anticancer properties.
While I am very open-minded to unconventional medical ideas and knew DMSO could treat a variety of otherwise incurable neurological diseases (e.g., ALS), there was one thing I always had a bit of difficulty believing. DMSO allegedly had been shown to cure Down Syndrome, demonstrated both in three clinical trials (e.g., this one and this one) and numerous remarkable case reports that were presented by multiple corroborating medical witnesses in Congressional testimony, along with numerous studies showing DMSO improved the cognition and behavior of developmentally delayed children. To explain this impossible benefit, I theorized it was likely due to DMSO’s protein stabilizing benefits, as Down Syndrome is characterized by “the aberrant accumulation of unfolded/misfolded proteins resulting from over-burdened protein quality control systems.”
In turn, one reader recently shared:
We’ve been giving some [DMSO] to our young daughter who has Down Syndrome. We've been giving her extra vitamins based on the treatment protocol of some studies that I found after reading your previous posts on this topic.
Almost immediately we noticed that our little girl was sleeping better through the night, and she's become more verbal. She'll be 2 in less than a week and she suddenly seems like she wants to say words more intentionally now, even if we mostly can't understand them yet. Also, her appetite has improved substantially. She just seems more active, and that's really awesome!
After which I received this comment:
This is such a helpful article! My husband is the one you quoted about using DMSO on our daughter with Down Syndrome...let me tell you, even in the time since he made that comment, we have seen changes in our little girl. The biggest one is that she is now CRAWLING-she had seemed for the longest time like she wasn't even interested, but now she's doing it (she started on her 2nd birthday, in fact!). And her coordination and motor skills are steadily improving as well. She is super close to sitting up on her own, something I was getting really worried about. There have been many other small improvements, and it's almost like she's not even the same kid she was two weeks ago. I write a blog here in Substack about raising a DS kid as naturally as possible, and this is going to give me PLENTY to write about. I am so grateful for your articles about it, and I am so excited to keep learning and seeing what's possible! Thank you so much!
What I find particularly noteworthy about this is that the “untreatability” of genetic disorders (which typically result from a dysfunctional protein) has justified spending incredible amounts of money on both research and treatments for them (e.g., the industry is still in its early stages but 20.4 billion is already spent each year on gene therapies in the United States—which in part explains why there was such a push to bring the unsafe mRNA platform onto the market and open up a massive new drug sector). In contrast, DMSO is virtually free and has been shown to treat many of these disorders we still do not have a good option for.
Collagen Disorders
Irregular depositions of collagen underlie many different diseases (e.g., many rheumatologic disorders and many degenerative results of aging). Fortunately, much in the same way DMSO can address the accumulation of abnormal proteins, it can also address a variety of collagen disorders by “softening” collagen. For example, in a recent article I highlighted how, in addition to DMSO aiding the healing of chronic wounds and surgical scars, it:
•Attenuate excessive MMP-9 activity (which when excessive creates disordered healing and is linked to a variety of fibrotic diseases).
•Decreases experimentally induced intestinal adhesions (a common complication of abdominal surgeries) and eliminates subcutaneous radiation-induced fibrosis (the pathologic deposition of collagen).
•Disrupt the links between collagen fibers and treats keloid scars by flattening and loosening their associated collagen bundles (a result also found in this study of ten patients with keloid scars) and has been shown to allows tight tissues to expand by loosening and relaxing collagen fibers and change the collagen structure detected by advanced imaging approaches.
•Strengthens the tensile strength of healing surgical incisions and post-surgical scars and prevents hypertrophic (excessive) post-surgical scar formation.
Beyond all of this being incredibly beneficial for surgical outcomes and preventing (the fairly common) chronic complications of surgery, it (along with DMSO’s previously mentioned ability to eliminate abnormal protein deposits) also indicates DMSO can help with other collagen disorders.
In turn, the earliest study I know of that found a benefit in collagen disorders was this 1965 study, which reported that over three months of treatment, 5 out of 4 patients with scleroderma had an improved range of motion and softening of their skin, while 3 out of 3 patients with a Dupuytren’s contracture had a reduction in plaque size in the palmar fascia and increased finger motion.
Note: many other reports of DMSO benefitting collagen disorders (e.g., this symposium which provided data on 9,521 patients with a variety of conditions such as Dupuytren's contractures) also exists.
DMSO and Contractures
Dupuytren’s contractures occur when the collagen under the palm builds up and abnormally thickens.

A variety of treatment options exist to address this issue (e.g., injecting an enzyme to digest the collagen, breaking the collagen up with a needle, or surgically removing it), but all have downsides (e.g., complications from the procedure or a recurrence of the contracture). In turn, there is still insufficient evidence to build a consensus on the best way to approach this common condition.
Before the FDA shut down DMSO, this is what Merck reported to their clinical investigators (after roughly 4,000 patients had received DMSO for up to 18 months):
Dupuytren’s contracture—Long-term administration has caused some improvement in fibrous scar contractures. 90 percent is recommended.
In addition to the study mentioned above where 3 out of 3 patients with Dupuytren’s contracture improved from DMSO, another study gave DMSO to 29 patients with Dupuytren’s contracture and found 2 had a complete remission, 14 had a partial remission, and 13 had no response (along with a single patient with a Cicatricial contracture who had a partial remission).
In another study, DMSO yielded good results for 6 out of 9 Dupuytren’s contractures (and 1 out of 3 Peyronie's disease).
Conversely, in another trial of 23 patients with Dupuytren’s contractures that had been present for over 5 years, receiving 80% DMSO 3 times a day for a month did not help any of them. This suggests that DMSO works best early in the disease process, that a month is not long enough to get results, and that 90% rather than 80% may be necessary for this application.
Peyronie's disease
Peyronie's disease is a condition in which fibrous scar tissue builds up in the penis, producing extreme pain whenever a patient gets an erection and gradually curves one’s erection.
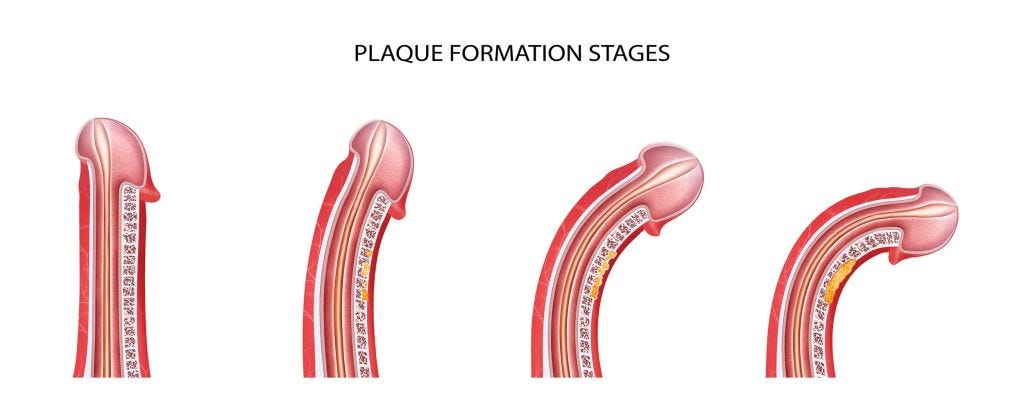
The exact cause of it is unknown, but it is thought to be due to a disordered wound healing process and, since 1828 has long been recognized to occur in association with Dupuytren’s contractures. Due to the sensitive nature of the condition, men are often reluctant to report it, and estimates vary greatly on how common it is (ranging from 0.3% to 16%).
Note: In addition to us hearing about this from our female patients, I have numerous friends who’ve confided with me they experience chronic discomfort from their husband having a slightly curved penis (which results in uneven pressure being applied to the vaginal wall), so I am inclined to believe a significant number of men are affected by the less severe stages of this disorder. As such, DMSO’s use here is something I really wish more men knew about.
Since the penis is more challenging to modify than the hands, many different approaches are used to address this collagen deposition, most of which have side effects and don’t always lead to satisfactory outcomes (and in most cases, the penis can never be completely straightened). However, DMSO was found to be effective, especially if used early in the disease process and applied for a prolonged period (e.g., a year).
Peyronie’s disease patients at the DMSO clinic in Portland receive topical application of DMSO directly in the penis, and Stanley Jacob reports relief in about 50 percent of the cases he treats. “We're not seeing rapid, significant improvement in curvature but the newer DMSO preparations we are employing are superior to DMSO water.”
Likewise, this is what Merck reported in a bulletin sent to their investigators:
Peyronie's disease—In a few patients so far treated, decreased size of the plaques and straightening of the penis has been noted.
In one of the few studies on DMSO and Peyronie’s disease, two Cleveland urologists, Lester Persky and Bruce H. Stewart, reported that of thirteen men with the condition who applied DMSO for 8-12 weeks, six were improved enough to resume reasonably normal intercourse. One patient showed a complete disappearance of the plaque caused by the disease.
In another 1967 study, four patients used 90% DMSO on the affected area several times daily for 2-3 months. Two patients responded with softening or disappearance of plaques and deformity was corrected in one.
In a 1980 Russian study (which used a slightly more complex treatment regimen that included rubbing 50-70% DMSO onto the affected area 2 times a day for a month), of 9 patients who started the protocol, 6 completed it (while 3 stopped for varying reasons) and of those who did it, 5 had a complete recovery while the 6th had a large improvement (no further progression and normalization of sexual function).
Additionally, a German and Polish study (both conducted in 1977) also used DMSO to treat Peyronie’s disease.1,2
While DMSO does not have a 100% cure rate for either of these conditions, it often works and unlike the other options is devoid of side effects. Because DMSO works best when used early and can be applied discreetly at home, it offers a powerful and accessible option for those dealing with these conditions—especially Peyronie's disease.
Lastly, other types of contractures can also be helped. For example, in this study of 20 rheumatoid arthritis patients with flexion contractures in various joints, DMSO (plus hydrocortisone) was found to increase joint flexion by 20-30 degrees, and after 30-40 days of post treatment follow up, there were no contractural relapses.
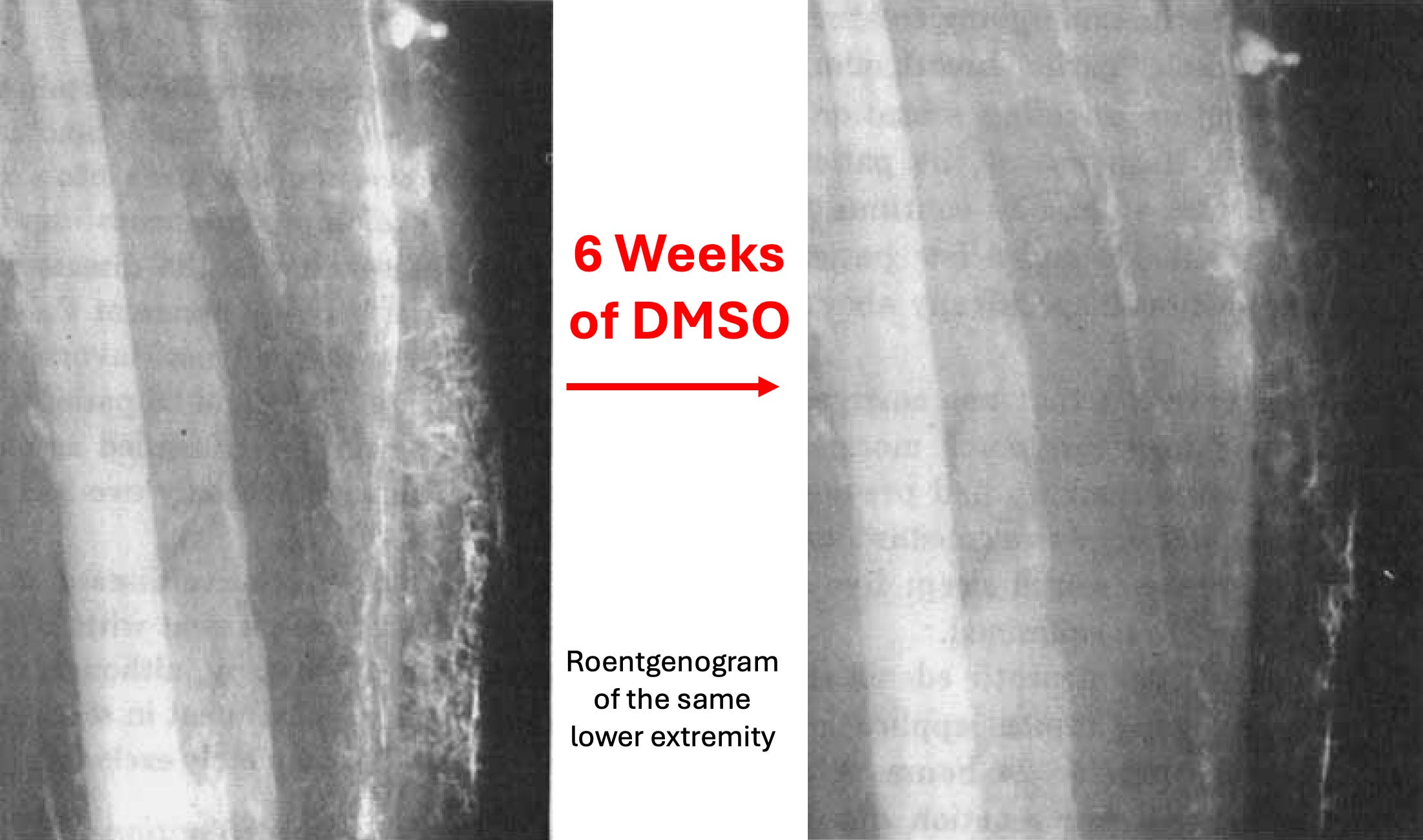
Fibrodysplasia Ossificans Progressiva
One of the most remarkable connective tissue disorders DMSO treats is fibrodysplasia ossificans progressiva (FOP), a rare genetic disorder (affecting 1 in 2 million people) where bone rather than connective tissue is created each time tissue heals, causing these people to gradually turn to human statues

FOP is classically considered to be impossible to cure since the extra bone can’t be removed as healing from the bone removal simply creates even more bone. FOP in short is one of those diseases where I just have always felt really sad thinking about what people who suffer from it go through:
Like Down Syndrome, non-profits have “worked” for decades to find a cure for FOP and come to accept nothing can be done for it but somehow are unaware of what DMSO did:
A man in his thirties had had the disease for twenty years In 1964 Jacob started him on DMSO, and after a few months (of topical application) he had improved. When they had started out, a good deal of his body had calcified—he couldn't move any of his joints; he couldn't lie, or sit other than rigidly; he couldn't bend his neck or move his fingers. His knees, his hips, his ankles—all were rigid. But he could open and close his mouth; so he could eat, and, for the time, survive.
"We concentrated on his shoulders," Jacob told me, ' 'because I felt that if we could get a little motion in the upper part of his body, it would make him less of a vegetable. After a couple of months, he did recover some shoulder motion [and his pain significantly decreased].
Then, gradually, some of the calicifed soft tissue lumps became smaller and smaller.
"When the FDA halted studies in November 1965, the young man had regained much use of his fingers; he wrote, literally, hundreds of letters—to the FDA, the Congressmen, and to the President. The FDA sent him stereotyped letters. The President, who receives a lot of touching appeals every day, overlooked this one.
Additionally, one reader here knew one of those patients (who may have been the previously mentioned individual):
My Uncle Red (Walter Kummer) took DMSO as part of a study at OHSU [with Stanley Jacob] in the '80s... maybe even late '70s for treatment of FOP - Fibrodysplasia Ossificanas Progressiva....his muscles turned into bone. He was diagnosed when he was 11 or 13 years old and wasn't supposed to live past 15, then 20 and eventually the medical doctors gave up guessing his lifespan. When he started taking DMSO it was first topical then he ingested it. I was very young but I remember dark colored bottles of DMSO being on the counter. Uncle Red must have been in his late 40s or 50s by that time when OHSU had him in the study. I think it helped him live as long as he did. I think he was in his late 60s when he died in the early 90s. I have never forgotten those bottles and Uncle Red.
Likewise, I spoke to another person who knew a younger woman with FOP Stanley Jacob treated who greatly benefitted from DMSO.
Scleroderma
During the eight months I have been testing DMSO, 1) I have been able to walk and drive a car (I had been consigned to a wheelchair by doctors at the University of Michigan Medical Center); 2) my terrible swallowing problem due to a calcified esophagus, has improved al- though I still eat baby food meats; 3) I still have nine fingers left, free so far from amputation. I'm fighting for a change in drug evaluation to give thousands of other people a future of some promise.
Scleroderma is another horrible disorder, that despite decades of work still has a poor prognosis (e.g., patients with it are 3.5 times as likely to die as the general population, and the rheumatologists I know have very few patients with this condition because they eventually die whereas most rheumatologic can be indefinitely managed). While the cause of scleroderma remains unknown, it is characterized by a hardening and thickening of the skin (effectively compressing the body like saran wrap) due to an abnormal growth of connective tissue (e.g., collagen) which is thought to begin in the blood vessels, in time enters the muscles and joints, and eventually gets into the internal organs (which is typically where death occurs). Two of the major complications of this disease are poor peripheral circulation (frequently creating ulcers and often progressing to the point fingers and toes often need to be amputated) and poor mobility due to a stiffening of the body.
From the start, DMSO was observed by many researchers to be immensely helpful in treating scleroderma, and much of the most vocal protest the FDA got on their ban of DMSO came from the fact they refused to approve it for scleroderma despite extensive evidence supporting its use compiled by leading rheumatologists.
•An early study gave six scleroderma patients with ulcers on their fingers DMSO (initially at 50% but gradually raised to 100%). Five significantly improved (four had their ulcers begin to heal in one or two days and were completely healed in two weeks, while the fifth took six weeks). The final patient could not tolerate DMSO and left the study. While DMSO was initially painted on the affected areas, many patients found they had a better response covering large parts of their body with it or immersing their affected fingers in it for one minute every two hours. Additionally, this study determined that the collagen deposition under the skin decreased with DMSO treatment.
Note: this study was initially inspired by the recognition that DMSO is very effective at treating pain, and scleroderma is often quite painful.
A follow up study reported the results of 42 patients with chronic scleroderma who had not responded to any previous treatment and often had significant organ involvement of the disease. DMSO was attempted and given at a dose they could tolerate (which ranged from 30-100% and often could be raised over time) and then either was just given to the affected part of the body, a significant part of it, the entire body, or in some cases by immersing the affected region in DMSO), and then after 2-3 weeks only administered to the hands, forearms, feet and occasionally the face. Additionally, 9 patients with circumscribed and interstitial calcinosis, tendon contractures, and capsular adhesions who had not responded to topical DMSO received 5-10ml of 1-5% DMSO injected subcutaneously once a day for four weeks.
In many cases, 1-2 years of therapy was needed to obtain a significant cutaneous improvement, and of the 42 patients 16 showed fair or poor response (e.g., 6 with late stage scleroderma died from their illness during the study) while 26 showed good or excellent improvement to DMSO. Of the 26 (62%) with a good response, most had to remain on it, but DMSO caused 3 to have a complete remission (and no longer need DMSO), while 9 who thought this had happened but later had to resume DMSO within four weeks because their symptoms (e.g., pain and stiffness) returned. Of the 19 patients with ulcers, the majority healed from topical DMSO, a few required immersion in DMSO, and it is unclear from the study what happened to the rest. There were also 2 patients with interstitial calcinosis that restricted joint motion and disappeared after DMSO.
Additionally, like the previous study, they determined that pathologic collagen deposits under the skin were being broken down and returned to their normal form, with collagen breakdown products increasing by approximately 50% in the urine— (whereas typically in scleroderma and other rheumatologic disorders that does not happen). This, in turn, is similar to how DMSO increases the urinary excretion of amyloid degradation products.
Note: if the FDA were at all reasonable, this study would have gotten approval to use DMSO to treat scleroderma, especially given the professional reputation of the rheumatologist who conducted the study.
In a final study, a Cleveland Clinic rheumatologist gave DMSO to 19 patients with systemic sclerosis and 3 with local sclerosis who’d had it for 1-20 years (averaging roughly 7 years) with a similar but more refined DMSO treatment protocol. This study had the most precise data, showing that DMSO softened the skin, improved joint motion and grip strength, and eliminated ulcers. Additionally, in this study, DMSO was only applied to one hand (so an untreated “control” would exist), but due to DMSO’s systemic absorption, the other hand also improved (although never more than the treated hand). In all cases, the effect of DMSO was temporary, so it had to be continued to sustain its benefits.
Note: a similar 1966 study concluded there was “no benefit” from DMSO because the changes observed in both the treated and untreated hand were similar (as the authors appeared to be unaware of the systemic effects of DMSO). I believe this issue characterizes the small number of other studies that found no benefit from DMSO in scleroderma (but I could not access the articles to confirm this).
Other data includes:
A study of 10 patients with scleroderma showed that their skin had greatly improved from DMSO to the point where the skin became supple and ulcers healed. That author then conducted a subsequent study on 20 patients, noting they “had increased mobility, rapid relief of pain and healing of persistent ulcers, arrest of the spread of cutaneous disease, regrowth of hair, and return of sensation and sweating.”
A study of 29 patients with systemic scleroderma that assessed blood flow (as scleroderma significantly impairs circulation) in the skin and muscles with a radioactive isotope. It found that 50% DMSO slightly improved it, increased it by 1.2 times when given with another agent, and by 6 times when given with 1% nicotinic acid. When the DMSO nicotinic acid combination was given, it also resolved their Raynaud’s syndrome, gross edema and hyperpigmentation of the skin. Additionally, when 50% DMSO was given with another agent, within a month it completely healed the ulcers on the fingers of 6 six patients it was tried on. Finally, the authors noted they’d used DMSO on roughly 2,500 rheumatologic patients (e.g., rheumatoid arthritic, scleroderma, amyloidosis) with excellent results.
Note: another paper detailed how DMSO causes a dilation of the blood vessels in the upper dermis of scleroderma patients. Additionally, in scleroderma, the ESR is elevated (which indicates blood cells are clumping together and disrupting the microcirculation), so since DMSO disperses clumped blood cells, this may also partly explain why it improves circulation in this illness.
A Russian study (I verified by translating) gave 30-90% DMSO 1-2 times a day to 52 women and 6 men with progressive scleroderma (that was often quite severe) for several months to 2 years. Within 1-2 months, significant improvement was observed in the skin and connective tissue, and in time, all ulcers disappeared. DMSO stopped the disease’s progression for all but 2 of them (96.6%), and clinical recovery occurred in 34 of the 40 with plaque scleroderma (while the remaining 6 improved but had to remain on DMSO). Linear scleroderma also responded to DMSO, but took much longer to regress. Of the 8 patients who had generalized scleroderma, 1 had a complete regression after 2 years, while the other 7 at the time of publication (after 2-3 months of treatment) had shown significant improvement in a wide range of areas. All 40 patients who completed the treatment course were monitored for up to 5 years, and no relapses occurred.
[Russian] patients commented on the suddenness with which the ugly old disabilities began to disappear and the rapidity of the healing process.
Many patients in that group have said they were happy to experience washing with DMSO," the scientists said. "It reportedly improved their well-being immediately, and they simply could not imagine life without DMSO. The results we have obtained have proved the high effectiveness of DMSO.
Another study found DMSO yielded good results for 3 out of 4 scleroderma patients.
Finally, when a Congressional Committee (unsuccessfully) pressured the FDA to legalize DMSO, as part of their case, they randomly surveyed 250 rheumatologists, of whom 68% responded, of whom 33% had used DMSO in their practice. Of them, 49% felt DMSO was effective (along with 23 more who did not have direct experience using it). Most of their uses were for musculoskeletal disorders, but many also reported using it for scleroderma. Sadly however, nowadays, it’s exceedingly rare for me to find rheumatologists who know much about DMSO.
Note: there are dozens of testimonials from scleroderma patients (e.g., at the committee hearing which I attached here) who experienced life-saving changes from DMSO and gave many heartfelt pleas to both the FDA and Congress for DMSO to be legalized for this condition. The most recent reference I could find to DMSO being used to treat scleroderma came from a 1998 Russian article.
Other Autoimmune Conditions
In the first two parts of this series (which can be read here and here), I provided numerous studies demonstrating DMSO’s ability to prevent or resolve experimentally induced inflammation (or tissue necrosis) and many others that mapped out its specific anti-inflammatory properties (e.g., it inhibits numerous inflammatory cytokines), and a wealth of data showing it was an effective treatment for rheumatoid arthritis.
Note: in the previous article, I forgot to mention that topical DMSO is often very helpful for insect and animal bites.
DMSO in turn, is well recognized for its anti-inflammatory actions, and some of my colleagues have used it for this purpose for years. Likewise, many authors have discussed its use in a variety of autoimmune disorders (e.g., this author discussed how DMSO can often be quite helpful for idiopathic thrombocytopenic purpura). In the section below, I will discuss its use in autoimmune conditions.
Note: chemoattractants are molecules that play a key role in the pathogenesis of autoimmune diseases by recruiting immune cells to affected tissues and when the chemoattractant system is dysregulated, it can contribute to immunopathology. DMSO has been found to prevent the recruited immune cells from sticking to the affected tissue, which in turn may also play a key role in how DMSO prevents immune disease.
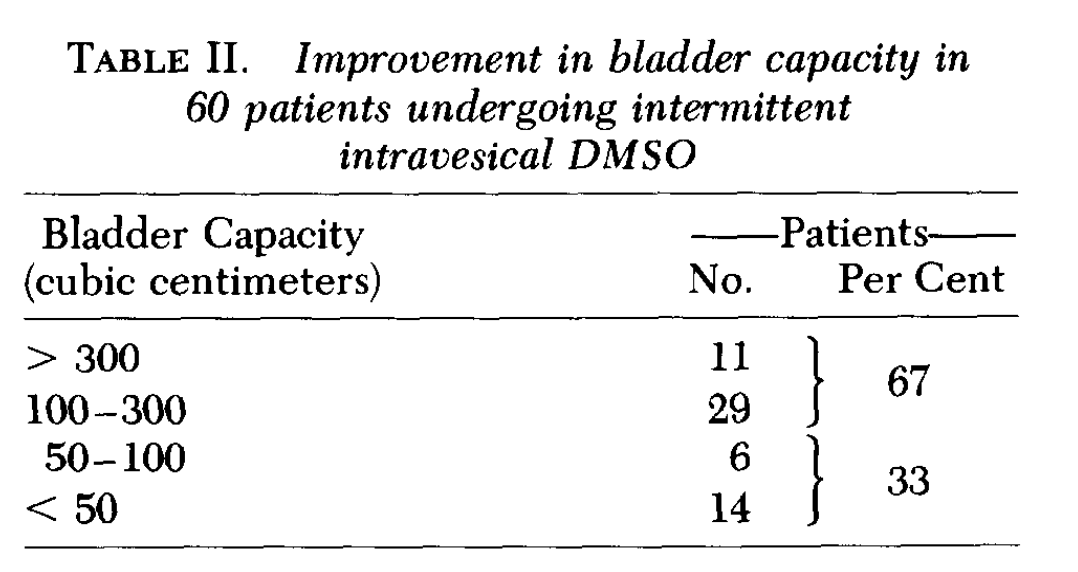
Interstitial Cystitis
Interstitial cystitis (also known as painful bladder syndrome) is defined as an unexplained irritation of the bladder wall that frequently is extremely painful (especially as the bladder fills) and often causes the patients to need to frequently urinate (e.g., up to 50 times one day—including at night), frequently causes bloody urine and in time can lead to scarring in the bladder which further reduce its maximum volume (hence making everything even worse).
Note: estimates on how common this disease (which is more common in women) vary, but they generally range from 0.87% - 17.3% as sometimes more or less stringent diagnostic criteria are used to diagnose it.
Remarkably, despite how common and debilitating this condition is (e.g., readers have emailed me about it), there still is no “good” way to deal with it, so various approaches are used that sometimes give varying degrees of symptomatic improvement.
Fortunately, the only medical condition DMSO (at 50%—sold as RIMSO-50) is approved to treat is interstitial cystitis (IC). This it got approved before the FDA decided to stonewall all DMSO approvals (e.g., for scleroderma). DMSO is thought to help IC by doing the following:
•It reduces bladder inflammation and pain (see this study, this study, this study, this study, and the studies I linked to here).
•It relaxes the bladder and pelvic detrusor muscles, and appears to address detrusor fibrosis is found in approximately 53% of IC patients (which are common issues in untreatable IC).
•It reduces bladder scar tissue by preventing collagen buildup inside the bladder.
•It reduces erosion and thinning of the bladder by reducing inflammation (e.g., see this and this study).
To illustrate:
A 38 year old lady in Las Vegas, Nevada, reported to the clinic with severe abdominal pain and blood in her urine. She needed to urinate approximately every 30 minutes, and she told the doctor that she was sure that she would be dead in a few months. She was sure that she had cancer. After a complete examination and tests this lady was informed that she did not have cancer. The problem was interstitial cystitis. She was treated with a bladder instillation of DMSO and told to drink one teaspoonful of DMSO twice a day in cranberry juice. This lady felt better almost immediately. Two months later her symptoms had completely disappeared. She had also complained about depression and aches and pains in various parts of her body. These were also gone, and she said she felt like a new woman.
Additionally, it’s quite safe (e.g., 100% DMSO put into the bladders of dogs for an hour each day produced no structural or functional changes to the bladder).
Similarly, since it is FDA-approved (and hence easy to research), a significant amount of evidence has accumulated over the years showing DMSO helps IC. That includes:
•A 1967 study that found DMSO was of great benefit for IC.
•A 1972 study of 21 patients that found 50% DMSO successfully controlled over half of the cases.
•A 1978 study (which can also be read here) of 213 patients with a variety of inflammatory conditions involving the lower genitourinary tract such as intractable IC, radiation cystitis, chronic prostatitis, and chronic female trigonitis who received intravesical (DMSO applied to the bladder through a catheter), most of whom were women and the majority of whom had a good response to DMSO. This study included 100 women with chronic classic interstitial cystitis (and 14 men with it) along with 31 women with atypical chronic cystitis.
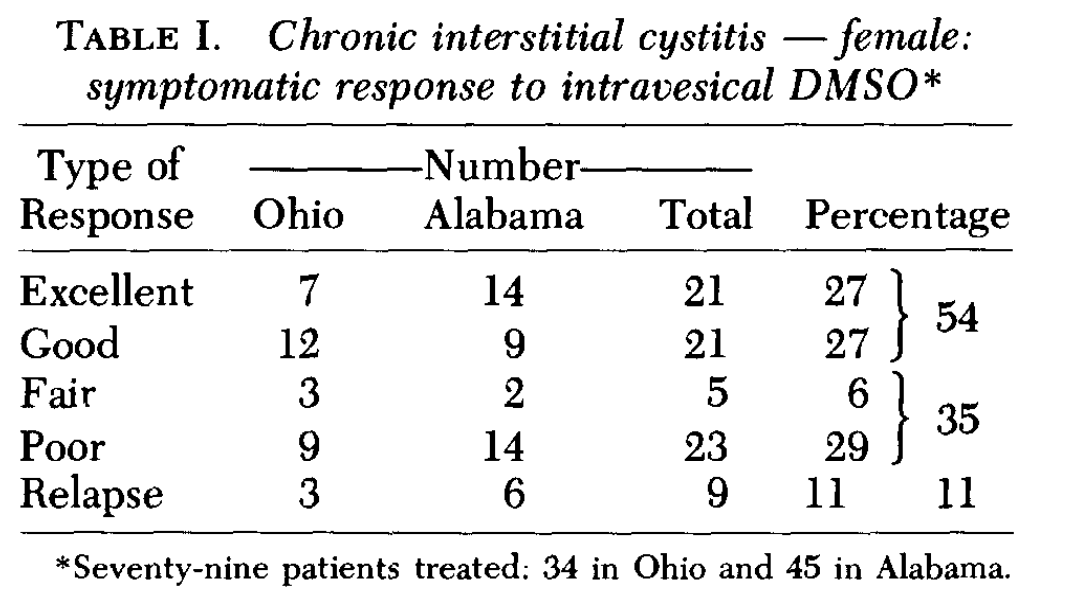
Additionally:
Of the 31 women with atypical IC, 13 had an excellent response, 10 a good response, 4 a fair response, and 4 a poor response. The visual appearance of the bladder improved in over 90% of the cases, but an improved bladder capacity over at least 100cc was only seen 20% of the time.
Of the 14 men with IC, 3 had an excellent response, 6 a good response, 4 had a transient improvement but ultimately required surgery, and at the time of publication, it was unclear if the last person would require surgery.
Of the 12 patients with radiation cystitis (e.g., from prostate cancer therapy) 50% had a positive response to it (3 “excellent,” 2 “good” and 1 “fair”).
Of the 35 patients with chronic prostatitis, 75% benefited significantly, with 12 having a “excellent” response, 14 a “good” response, and in 90% of cases, inflammation of the prostatic urethra improved.
Note that study was preceded by this 1976 study.
•A 1978 study of 17 IC patients (including one man) found DMSO treated symptoms in 12 patients (sometimes in a dramatic fashion) while 5 did not respond to it.
•A 1988 study of 33 IC patients (including 3 men), found 53% had a marked improvement after DMSO (compared to 18% of placebo) and 93% had an objective improvement (compared to 35% of placebo).
Additionally, as this 1993 study and this 2012 study show, cases of IC that do not respond to DMSO often respond if another agent (e.g., heparin, corticosteroids, hyaluronic acid or analgesics) is mixed with the DMSO. Likewise some successful IC studies found DMSO made another agent more effective (e.g., this 2008 RCT of 22 IC patients found intravesical DMSO plus oral amitriptyline was more effective than just amitriptyline for reducing urinary frequency, urgency, and bladder pain).
Lupus
I occasionally hear of DMSO being used to treat Lupus. For example, this author discusses how it greatly reduces the symptoms of Lupus and is more effective for the condition than steroids (which unlike DMSO are quite damaging if taken for a prolonged period).
The only publication I know of which evaluated DMSO’s effect on Lupus reported on two women with Lupus that was causing (pathologically confirmed) lupus interstitial cystitis and had not responded to prednisone. Both had a complete remission of their interstitial cystitis after intravesical DMSO.
Asthma
Numerous patients have found DMSO is quite helpful for asthma, often reducing the dose of the harmful medications they need to manage the condition, and in some cases eliminating the need for it. Typically, this is done with topical applications that sometimes mix in other agents which are beneficial in asthma. Additionally, DMSO can help with allergies and patients taking DMSO for other issues sometimes notice their allergies disappear.
While many others (e.g., this author) have shared anecdotal reports of DMSO helping asthma, I only know of one study (which was summarized in this book) that directly evaluated this. It gave 153 adults (84 men and 69 women) DMSO mixed with a bronchodilator, a steroid, and an antihistamine all administered by intramuscular injections of whom 43 of whom had frequent asthmatic crises (with asymptomatic periods) and 110 with more intense and frequent crises (despite receiving the standard therapies for asthma). The evaluations included all the standard pulmonary assessments, and it was found that the DMSO solution gave 37 (24.5%) an excellent result, 92 (60%) a good response, while 24 (15.5% had no change).
Note: many have observed DMSO increases the potency of cortisol (thereby allowing many patients who require cortisone for an autoimmune disorder to drop to a lower and less toxic dosage). Similarly, a variety of effective potent topical products that combine DMSO with cortisol have been created. Two studies have also corroborated this effect in cells. One found that mixing DMSO with a steroid made the steroid between 10 to 1000 times more potent in stabilizing lysozymes (assessed by how many enzymes the lysozymes leaked), while the other found DMSO greatly increased steroids ability to reduce the proliferation of fibroblasts. Additionally, another study found that in adrenal cells from newborn pigs, 3-5% DMSO stimulated their secretion of cortisol while 10% DMSO inhibited it.
Multiple Sclerosis
Numerous authors have reported dramatic results in Multiple Sclerosis (MS) patients. For example, a 29 year patient who was paralyzed from MS and trying to get access to dialysis (when very few units were available) saw Stanley Jacob, who decided to risk giving her DMSO orally (despite her kidney failure).
Her improvement was dramatic—as dramatic as any benefit I have ever seen ," Jacob told me. Her renal problem seemed to come under control. Then—after a few more weeks—she walked again.
"Now, six years after her first DMSO treatment, she still has wobbly knees. But she walks. She drives her car. She takes care of her two children and her husband. But she is going downhill. I wish we could help her again, but we just don't seem able to. Despite this, however, I am not convinced that DMSO alone is useful in multiple sclerosis.
Likewise, another author shared the case of a California woman who was confined to bed, typically was in the fetal position, and was living at a convalescent hospital as she was expected to die within a few months. She was then given DMSO through multiple routes (e.g., injectable, oral and topical).
Shortly after treatment started, this lady complained that the treatment was causing pain in her legs. Prior to treatment she had very little feeling in her legs so even this pain was considered to be positive. Slightly over a year after treatment was started, this lady was able to move her legs. She later was able to feed herself. Improvement continued until this lady was moved to another state to be closer to some members of her family who thought the same treatment would be available in her new location.
The only study I know of that evaluated DMSO for MS was conducted on 34 patients in Russia in 1984. Overall, the investigators felt DMSO had a very positive result for MS, with the best results seen in patients who had remitting MS, while the results were more inconsistent in patients with rapidly progressive MS. The investigators assessed this was due to DMSO causing remyelination, a reduction in edema, and improved communication between nerve cells alongside DMSO having a positive effect on immunity and antiallergic and reparative action on the injured tissues.
Lastly, when myelin is broken apart by the immune system, phospholipids within the debris that can cause blood clotting become exposed and compromise the critical blood supply nerves rely upon, providing a secondary mechanism to explain the neurodegeneration seen in MS. Existing anticoagulants do not target this clotting pathway, but a very interesting Russian study determined that DMSO inhibited the blood clotting triggered by myelin in a dose-dependent manner.
Note: there was also a reported case of Stanley Jacob treating a patient with ALS which resulted in “some instant, overnight and slightly delayed wonders of therapy,” and this user reported she saw it visibly improve the condition. In our own experience IV DMSO is one of the only things which can treat ALS (typically it halts the progression of the disease).
Uveitis
One study induced uveitis (inflammation of the middle layer of the eye) in dogs, and found that subsequently giving DMSO decreased intraocular pressure and fibrin production—suggesting DMSO has therapeutic value in this condition.
Note: another study used DMSO to treat endogenous iridocyclitis (inflammation of the vascular layer of the eye).
Inflammatory Bowel Diseases
Quite a few of my colleagues believe the most important use of DMSO is that it is profoundly anti-inflammatory (but safe), and that it is particularly useful for inflammatory bowel disorders—especially when done early in the illness. Likewise, many DMSO authors report the same.
Note: others believe DMSO’s best use is healing brain tissue (e.g., after a stroke).
The only study I know that directly evaluated this question (and can be read here) took patients with recurrent attacks of proctosigmoidal ulcerative colitis that was not prevented by 2mg prophylactic sulfasalazine and then gave them 500mg sulfasalazine and 10 mg of prednisolone four times a day, and a 20mg prednisolone enema at night. After two weeks passed, 45 (51%) were free of symptoms, and 45 were given DMSO while 46 were given allopurinol (in addition to the existing regiment), resulting in 84% being free of symptoms. After two weeks, they were then put on 2mg of sulfasalazine alone each day, or it with either allopurinol or DMSO. After a year, 25% of those on sulfasalazine had a relapse, while 5% of those who also received allopurinol and 5% of those who also received DMSO relapsed. Additionally, the data showed DMSO significantly reduced the ESR over 2 weeks (by 77% compared to 37% with the standard approach), the (high) white blood cell count (by 65% vs. 41%) and raised the low albumin (by 9% vs. 7.8%). While all of that is a bit confusing to follow, it essentially says that DMSO, when compared to standard therapies, improved ulcerative colitis and prevented its recurrence.
Additionally, while not a study, I thought this passage by Pat McGrady should be included:
At 12:50 p.m., February 5, 1968, E. Rottenberg of the Ozothine Laboratories, Hauts-de-Seine, France, [unsuccessfully] applied for a patent for DMSO 'for treatment of all irritating conditions of the alimentary canal.’
He cited as support for his application these examples:
Acute gastritis—Twenty-eight patients unable to work went back to their labors following five to eight days of treatment, rid of such symptoms as nausea, vomiting, pain, gastric heaviness; their stomach secretions became normal and so did their general condition. One year later, twenty-one were still free of symptoms, working and off their diets. During this time about ten had undergone treatment again for about fifteen days.
Chronic gastritis—Thirteen patients on assorted treatments all relapsed on stopping treatment. On DMSO by mouth for one to two months, symptoms cleared up and all of them went back to work. At the end of a year, all of them remained improved, although some had resumed treatment two or three times.
Peptic Ulcer—Five patients were completely cured of recent peptic ulcers with oral DMSO, without recurrence during the following year.Enterocolitis—Six patients with abdominal pain for several months and with diarrhea, emaciated and asthenic, began to improve after eight days on oral DMSO, and all were back at work in two months, pain-free and in good shape.
Mucomembranous colitis—Three patients were "cured" after three weeks of oral DMSO.
When the DMSO is combined with star anise, the appetite improves, the application stated.
Myasthenia Gravis
In order for skeletal muscles to fire, they need to receive acetylcholine from the nerve that directs them. In myasthenia gravis (MG) the body forms antibodies to the muscle's acetylcholine receptors (AChRs), and as they are destroyed, the muscles need more and more acetylcholine to be sent by the nerves to activate. In turn, MG is managed by various immune suppressing medications, filtering the AChR antibodies out of the blood and acetylcholine esterase inhibitors (which boost acetylcholine levels). Since DMSO both reduces harmful immune activity and is also an acetylcholine esterase inhibitor, there is a rational basis for using it to treat MG.
That possibility was initially discovered (accidentally) in 1980, when two researchers tested a variety of agents for their ability to reduce AChR antibodies, and realized that the DMSO being used as a vehicle for the various agents they were testing was independently reducing those antibodies. They then found giving rats daily intraperitoneal injections of 1 mL DMSO for two weeks resulted in a 52% decrease in AChR antibodies (but not total IgG levels) that were observed for an additional six weeks after treatment was terminated.
Note: after this discovery, the researchers expressed their eagerness to test DMSO in humans with MG (the New York Times even covered it).
A follow-up rat study then found DMSO suppressed anti-AChR antibody levels by an average of 53%–76%, with the effect being similar regardless of whether DMSO was given orally, rectally, or intraperitoneally. Additionally, DMSO treatment was observed to suppress the anti-AChR antibody response in rats to a weak primary antigenic stimulus.
Sadly, no human studies have ever been performed for DMSO with MG. However, patients and integrative healthcare providers sometimes do it and report success from doing so (along with again cautioning that if cortisone is being used, DMSO will significantly increase its effect on the body).
Note: this research inspired a 1982 study to determine if DMSO suppressed thyroid autoantibodies (which were experimentally induced in rats). It did, and also was found to increase the ratio of IgM to IgG plaque forming cells (which suggested a true immunoregulatory effect). In turn, some patients report that DMSO benefits autoimmune thyroiditis.
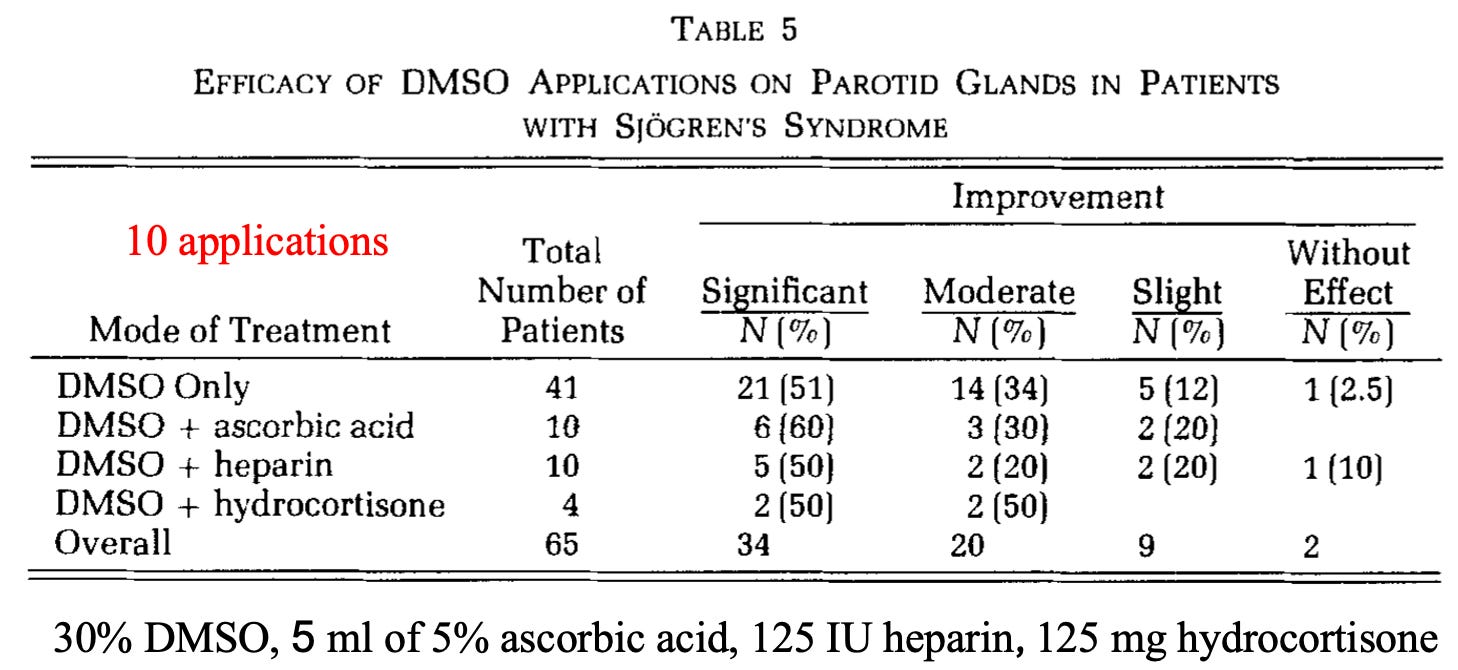
Sjogren's syndrome
Sjogren's syndrome (autoimmunity of the parotid gland) results in a loss of saliva and the mouth becoming very dry. Since it is a very difficult condition to treat, this table within a larger study caught my eye:
Pleomorphism and Autoimmunity
Over the years, I’ve seen many accepted mechanisms of action for pharmaceutical drugs later be discarded (e.g., the chemical imbalance theory of depression was pseudoscience from the start, and it is now becoming accepted antidepressants don’t work by raising brain serotonin levels—which if anything actually increases the risk of suicide).
One of DMSO’s widely recognized properties is it causes cancerous cells to revert to being normal. In researching that (which will be covered later in this series), I came across a fascinating study that tested cancer patients for pleomorphic bacteria (something many previous pioneers of successful but suppressed alternative cancer therapies like Rife and Naessens also believed caused many cancers) and found those bacteria were present. It then tested all 27 isolated organisms and found that 12.5-25% DMSO caused an almost complete inhibition of their growth (without affecting intact red blood cells).
The pleomorphic model of bacteria (discussed further here) essentially states that bacteria can significantly change their morphology (to the point they are almost unrecognizable from their original form), that these changes are often done in response to their environment, and that some forms are relatively harmless to the body, while others cause disease. In turn, since things that kill bacteria often transform them into ones that are more pathogenic, a longtime belief within certain schools of natural medicine is that the goal should be to change the terrain of the body to encourage a benign morphology of bacteria rather than trying to kill them all off.
Note: some of these schools also believe this applies to viruses and fungi, and that, in some cases, they can transform from one type to another (e.g., a bacteria becoming fungal).
A large group of modern researchers studied this subject for decades (e.g., hundreds of research studies they conducted are summarized in this wonderful textbook by Lida Mattman). Five of their key observations were:
•Antibiotics will often fail to kill every bacteria present and then trigger those that survive to enter a primitive survival state known as a “cell wall deficient” (CWD) form resembling a mycoplasma. This process in turn, was most commonly triggered by antibiotics that attack bacterial cell walls (which characterizes many commonly used antibiotics).
•CWD bacteria are very hard to detect (most standard microbial methods will determine that no organisms are there when CWDs are present).
•When conditions are more optimal for survival, CWD organisms can revert to the active form and cause an infection that had been eliminated with antibiotics to suddenly and inexplicably recur (which, for example, we frequently see with urinary tract infections).
•Once present, CWD bacteria will often enter cells and cause chronic inflammation because the immune system will attack cells with the CWD bacteria.
•Many different unexplained autoimmune disorders (e.g., sarcoidosis) have characteristic CWD bacteria present that can be repeatedly identified from their inflamed tissue (the textbook cites an exhaustive amount of data substantiating this).
•While standard antibiotics are ineffective in treating CWD infections, non-standard ones (e.g., erythromycin or minocycline) often are, but the sensitivity to those antibiotics is highly variable depending on the causative organism.
In practice, we find 10-15% of chronic illnesses (including blood clots and cancers) have a pleomorphic etiology, but rather than try to eliminate those organisms with antibiotics (which always have side effects), we instead give signaling products derived from healthy bacteria that cause the pathologic bacteria to transform into a non-harmful form, which in those applicable cases, frequently yields remarkable results (e.g., this approach is very useful for lupus and many cancers). Likewise, I believe this model explains a longstanding belief within natural medicine that giving antibiotics for an acute infection often transforms it into a chronic illness down the road.
Note: ultraviolet blood irradiation is also quite effective at eliminating these organisms and the diseases they cause. For example, a case report discussed a cohort of 5 family members who had a variety of chronic diseases (e.g., Crohn's disease, asthma, complex regional pain syndrome, hypothyroidism, type 1 diabetes mellitus, and lymphangiomatosis) and found that 4 had a MAP (mycobacterium paratuberculosis) infection. Two patients received antibiotics and UVBI, and then experienced a resolution of their autoimmune symptoms.
As it so happens, many of the most commonly used rheumatologic drugs also function as antibiotics (e.g., see this study, this study, and this study). For example, the most commonly used drug in rheumatology (methotrexate) works by blocking the enzyme that converts folate into the active form which is needed for DNA synthesis, and likewise, two commonly used antibiotics (sulfamethoxazole and trimethoprim—typically sold in the combination bactrim) work by blocking the folate converting enzymes in bacterial cells. In turn, when bactrim is given in conjunction with methotrexate, the combination is often much more toxic to patients than either is alone.
In the case of methotrexate, my suspicion there might be another mechanism at work for the drug began early in my training when I learned that it worked by blocking folic acid production but that “the side effects of methotrexate can be prevented by giving supplemental folic acid” (which essentially defeats the stated point of the drug) and once I learned about the pleomorphic model of autoimmunity, I hence suspected it had antimicrobial effects on those organisms. As the previously mentioned studies show, it does, but it is typically considered to be a poor antibiotic because it has poor bacterial permeability (difficulty entering them). However, unlike normal bacteria, cell-wall deficient bacteria lack a cell well and hence are much more permeable.
Likewise, over the years, many have observed using non-standard antibiotics (particularly minocycline) can provide dramatic improvement for autoimmune conditions like rheumatoid arthritis or ALS. Still, since none of them ever worked consistently, they never became standard of care. That said, many forgotten trials exist, such as this Lancet publication showing minocycline frequently helped early-stage scleroderma.
Note: on Sept. 29, 1998, the National Enquirer had an article titled: "Deadly Disease That Turns People To Stone Cured By Simple Antibiotic." I have been trying to find a copy of it (as Mattman referenced it in her Scleroderma chapter, but the title seems to describe fibrodysplasia ossificans progressiva).
In the case of both interstitial cystitis and scleroderma, many suspected they might have a bacteria component, but since they could not be isolated with conventional methods, the cause of these illnesses remains “unknown.” However:
•A study of bladder biopsies from interstitial cystitis patients (using methods that can detect CWD organisms) was able to identify a gram-negative organism (not found in controls) they described as “the forms contain nucleic acids and resemble cell wall-deficient bacteria in gross morphology; however, their swirled myelin-like ultrastructure is unusual and suggests a heretofore unclassified microbe.” Later, another study was able to also identify these organisms in the blood of interstitial cystitis patients and determined that it was highly resistant to antimicrobials (e.g., it could replicate in 5% phenol and was not inhibited by chloromycetin or streptomycin).
Note: numerous studies have shown interstitial cystitis makes someone 2-5 times as likely to develop bladder cancer, a cancer which is often treated with the (live) tuberculosis vaccine. As tuberculosis is a mycoplasma, I have often wondered if this therapy works by stimulating the immune system to eliminate a related CWD in the bladder.
•In the case of scleroderma, one researcher has consistently found acid-fast pleomorphic organism in the tissues of Scleroderma patients.1,2,3,4,5,6,7 Likewise, Mattman was able to consistently culture a pleomorphic organism from the blood of those patients.
In short, I suspect that beyond DMSO being anti-inflammatory, a key reason why it helps so many autoimmune conditions is because it effectively inhibits the growth of pleomorphic bacteria. Unfortunately, in some conditions (e.g., scleroderma), this also requires it to be consumed for life as rather than eliminate the bacteria it only inhibits their growth.
Note: I also suspect one of the reasons the COVID-19 vaccines cause a variety of autoimmune conditions is because the immune suppression they create allows already existing CWD infections to grow out of control. Likewise, a case can be made the childhood vaccines trigger this process either through immune suppression or by the adjuvants they contain triggering bacteria to change to their CWD forms.
Presently, I feel more comfortable suggesting this model for IC than scleroderma, as we have found two specific therapies aimed at correcting the pleomorphic balance of the bladder are very helpful for IC, whereas scleroderma patients are so much rarer, there hasn’t been the opportunity to adequately explore this hypothesis there. Likewise, one of the only other things that really helps IC is avoiding the dietary triggers for it, and within the terrain theory model, a large focus is always given to eating foods that encourage a healthy morphology of the bacteria present within the body.
DMSO Protocols
One of the things that’s very challenging about using DMSO is that there is a significant amount of variation in what each individual will best respond to. Because of this, in the first and second parts of this series, I attempted to provide a very detailed explanation that could try to account for each possibility. From the feedback I have gotten, I’ve realized that it is also necessary to make a more straightforward set of instructions for using DMSO that is more accessible.
In the final part of this article, I will share that guidance along with everything else you need to know about DMSO (e.g., where to get it) and more specific approaches for some of the conditions discussed in this article along with the topics I am planning to cover in the rest of this series.
