DMSO is a Miraculous Therapy for Chronic Pain and Musculoskeletal Injuries
The decades of evidence DMSO revolutionizes the practice of medicine

Story at a Glance:
•The standard approach for treating pain and musculoskeletal injuries typically involves giving NSAIDs (e.g., ibuprofen), and in more severe cases, opioids. Unfortunately, these drugs are extremely dangerous (e.g., each one kills tens of thousands of people each year), but nonetheless have remained the standard of care for decades.
•DMSO is a remarkably effective pain-killing agent, in many cases allowing individuals who’d been disabled for years by their pain (e.g., a failed spine surgery or severe arthritis—DMSO’s most popular use) to get their lives back. Furthermore, it can treat many types of pain other therapies do not work on (e.g., complex regional pain syndrome).
•DMSO is a highly effective therapy for healing wounds and creating healthy scars, making it particularly helpful for recovering from surgery.
•DMSO is incredibly effective for healing a wide range of acute and chronic musculoskeletal injuries (e.g., arthritis, headaches, neck and back strains, restless leg syndrome, sprained ankles, trigeminal neuralgia and numerous traumatic injuries). It typically has an 80-90% success rate and often has an instant and dramatic effect. This use was particularly popular with professional athletes, as it allowed many of them to quickly return to the field rather than be out for the rest of the season.
•In this article, I will review the scientific literature that explains how DMSO provides pain relief and healing, the vast body of evidence (comprising of thousands of patients) showing it indeed does, and our preferred DMSO home treatment protocols for pain, arthritis, and musculoskeletal injury (along with the best sources for procuring DMSO).
One of the curious facets of Western Medicine is that while money is always spent on “research,” whenever the occasional miracle drug comes out that works too well with a wide range of applications, it is inevitably consigned to the dustbin of history regardless of the data put forward for it.
In the first part of this series (which provides important context for this article), I listed the decades of evidence that demonstrates the simple (naturally occurring) chemical Dimethyl Sulfoxide (DMSO) is a remarkably safe drug that completely transforms the care of many challenging and insurmountable illnesses (e.g., strokes, severe head trauma, spinal cord injuries, amyloidosis, Down’s Syndrome and dementia).
Note: after publishing the first article, I received many correspondences from readers who said DMSO was life saving when they had a stroke, many more testimonials on Twitter, and a few stories where it was used to treat a pet’s stroke (e.g., this reader’s dog).
However, while each of these applications, particularly DMSO’s utility in strokes, would completely change medicine and how those lifelong illnesses affect our society (and were what drove many doctors to spend decades researching DMSO), none of that accounts for why DMSO took America by storm and campaigns were launched (that members of Congress eventually joined) to overturn the FDA’s embargo on DMSO.
Rather, it was because DMSO solved three of the most common problems in medicine:
•It quickly heals a wide variety of musculoskeletal injuries (e.g., those routinely experienced by professional athletes or a chronic back injury leading to partial disability).
•It effectively treats a variety of joint disorders (e.g., rheumatoid arthritis).
•It’s an extremely effective and very safe painkiller.
Because of this, it was miraculous for many with chronic pain and disability (e.g., from osteoarthritis or a failed spinal surgery), particularly since all other pain-killing medications have significant (and frequently lethal) side effects and worse still—often don’t even work.
Note: a key theme to consider throughout this article is the immense difference in toxicity between DMSO and its conventional alternatives (such as corticosteroids and gabapentin). For example, NSAIDS and opioids each kill tens of thousands of Americans each year, whereas in over 60 years of use by millions of people, DMSO has not been linked to a single death. Likewise, NSAIDS are the leading cause of drug induced hospital admissions (because they are toxic to the heart and small intestine and particularly toxic to kidneys and stomach), whereas a systematic review of all published DMSO studies found the side effects associated with DMSO (e.g., typically skin irritation or a garlic-like odor and occasionally nausea, vomiting or diarrhea ) were minor and transient. Likewise, it’s very easy to overdose on an NSAID or Opioid, whereas a meticulous human study found taking 90 days of DMSO at 3-30 times the standard dosage did not cause any toxicity and was well tolerated by the research subjects (whereas almost any other drug would be extremely dangerous at doses that high).
This program about DMSO on 60 Minutes, for example, provides a context to how impactful it was for many Americans:
Additionally, shortly after this segment aired, a March 24, 1980, congressional hearing was held on the merits of DMSO, which grilled the FDA on its decades of stonewalling DMSO (leading to the FDA promising to treat DMSO fairly at the hearing).
Sadly, despite the incredibly compelling testimony presented at the hearing, a subsequent Senate subcommittee hearing being held over the drug’s status with the FDA on July 31, 1980, the former governor of Alabama being treated with it and a champion of DMSO becoming the Secretary of Health and Human Services in 1985, the FDA never relented, and DMSO remains a forgotten side of medicine,
Note: the transcript of the Congressional hearing will be cited throughout this article.
In short, if DMSO were to become the standard of care due to its remarkably high success rate in treating a variety of common conditions, it would completely change the practice of medicine in the United States and likely knock many existing approaches out of business.
To illustrate, after I published the first article in this series, I received many emails like this:
Thank you for your email on DMSO. I had severe pain in my piriformis for over 2 months and couldn't walk, and tried everything without success. I work in orthopedics, and have tried multiple injections, etc. When I read your article, I remembered using DMSO in the past for athletic injuries. I found an old bottle of DMSO 99% pure that I bought at a "Feed and Seed" store, for horses, about 25 years ago, but never threw it out. I immediately applied it to the painful areas, and it really worked! — Harriet
Likewise, to show how versatile and frequent the uses for DMSO are, since publishing the first article, in addition to treating a few cases of knee osteoarthritis (an area where DMSO excels), I had a relative in another state recently deliver a child at home who 12 hours later was in significant pain and could barely go to the bathroom (even with assistance). I told her to take DMSO (which she had at home since I encourage all my relatives to keep it on hand in case someone has a stroke). Within minutes, she had regained her mobility, her painful abdomen began normalizing, and she was able to quickly get through what would have otherwise been (knowing her medical history) a challenging recovery. Furthermore, I also had a friend in another state contact me about complications from a hernia surgery a few days before (which DMSO also addressed).
Note: unless you’ve birthed a child, it’s quite difficult to truly appreciate just how challenging both childbirth and the recovery process can be. After I started working with chronic pain patients, I realized many of them were in an analogous situation as many of the people they interacted with simply did not have the context to grasp how just difficult every moment of their life was.
It is understandably a bit hard to believe that DMSO can actually do that, so I have put a lot of work into presenting the evidence that it indeed does (which is essentially why I have been publishing less new content recently).
Note: one of the most important precautions with DMSO is to not havee a toxic chemical on the skin (e.g., a pesticide, nicotine or mercury) which it can draw into the body once DMSO is applied there (hence why it’s generally advised to wash the skin beforehand). Additionally, there are some unresolved questions about using DMSO while pregnant that will be discussed in an upcoming article.
How DMSO Works
In the first part of this series, I provided a wealth of evidence that demonstrates a few key properties of DMSO, such as:
•It rapidly spreading throughout the body once it contacts the skin (or is ingested), and if mixed with anything, brings that into the body as well.
•It protecting cells from a variety of otherwise lethal stressors (e.g., burns, being frozen, losing their blood supply, radiation, and sonic shockwaves). This amongst other things allows it to be a miraculous therapeutic for otherwise crippling injuries of the central nervous system (e.g., strokes and spinal cord injuries).
•It is incredibly safe (with the primary side effects being a temporary concentration dependent irritation when it’s applied to the skin and in certain individuals, an unpleasant garlic like odor that lasts for a few hours, while the primary severe side effect is a 1/2000 chance of an allergic reaction.).
•It significantly increases blood circulation throughout the body and simultaneously removes edema and excess fluid from where it does not belong. This is particularly important for the joints, as their structure predisposes them to having a limited blood supply (especially when they are damaged and need that blood to heal).
These help explain how DMSO is almost universally applicable to a wide range of conditions—but simultaneously are only some of its remarkable properties. For instance, I believe its ability to rapidly heal injuries and eliminate pain results from being highly anti-inflammatory, restoring critical blood flow, being an effective muscle relaxant, protecting cells from death, and blocking the conduction of problematic pain signals.
If you take a step back for a moment, it’s extraordinary a single substance can do all of that at the same time—particularly since the drugs we have that only do one or two of those (e.g., NSAIDs, steroids, or opioids) are often quite dangerous.
Note: in addition to these mechanisms, I believe that DMSO’s other properties may also explain its analgesic effects. For example, pain is often due to a tight muscle or injured tissue, and since DMSO treats each of these, it can eliminate the “root cause” of pain.
However, I believe DMSO’s least appreciated effect arises from its ability to eliminate blood stasis in the body, as in many cases, chronic pain is due to insufficient blood reaching an area (e.g., DMSO has been recognized to address the pain associated with blood clots). This builds on an observation from Chinese Medicine that blood stasis can cause severe pain throughout the body (e.g., sharp piercing pains are often associated with blood stasis) and my observation that blood stasis is a key disease of the modern age (in large part due to vaccines altering the electrical dispersion within the body and creating micro clots throughout it).
How DMSO Treats Pain
Note: I harbor strong ethical issues with animal experimentation (discussed further here) but am nonetheless citing animal studies because it is important for this information to be known.
A few mechanisms have been identified to explain how DMSO treats pain (many of which also likely account for DMSO’s remarkable ability to heal musculoskeletal injuries).
Conduction Blocking
Many different nerves exist in the body. One group, known as the “small fibers” are responsible for transmitting specific sensations and (particularly the C fibers) are frequently linked to debilitating chronic pain syndromes (e.g., small fiber neuropathy, is characterized by sensations of pins-and-needles, pricks, tingling, and numbness alongside burning pain and electrical shocks).
Note: the five most common symptoms of COVID vaccine injuries, in order, are fatigue, post-exertional malaise, brain fog (discussed further here), small fiber neuropathy, and dysautonomia.
DMSO selectively blocks the conductions of these smaller fibers, thereby stopping the pain without causing significant damage to the rest of the body or the body developing a tolerance to it (rather DMSO typically becomes more effective with time).
Note: alpha-delta (Aδ) fibers are responsible for sensing shallow, quick and sharp pain, whereas C fibers (especially when repeatedly triggered) mediate stronger somatic signals involving temperature, sensual touch, and muscle and joint pain—in essence comprising many common facets of chronic pain.
This is supported by the following data:
•One study evaluated sural nerves within cats and found that 5% DMSO slowed the conduction and decreased the amplitude of nerve impulses within the C fibers, while higher doses (9%) blocked it (with the block being instantaneous at 15%), and that these effects disappeared once DMSO was washed off. Another study of cat radial nerves found that at lower concentrations, DMSO blocked the conduction of small nerve fibers (first C and then Aδ), while at high concentrations, it blocked the conduction of larger fibers (alpha-beta [Aβ] and alpha-gamma [Aγ])
Note: this blockade is thought to be in part due to DMSO decreasing the resting membrane potential by changing its permeability to chloride and potassium (e.g., by blocking the leak channels).
•Another study found 5-10% DMSO blocked the afterdischarges of C-fibers (a process associated with painful stimuli).
•DMSO has been observed to suppress NMDA and AMPA induced ion fluxes in neurons, each of which are receptors linked to chronic pain (e.g., NMDA is linked to central pain sensitization).
Note: I believe this property may in part account for why DMSO treats complex regional pain syndrome. Likewise it has been proposed to explain its utility in treating cancer pain.
•DMSO has also been observed to block sodium and calcium ions' entry into cells (likewise, many local anesthetics work by blocking sodium ion entry). This effect has also been proposed to explain how DMSO can help cancer pain.
Note: DMSO has also been reported to significantly enhance the potency of local anesthetics (which in turn has been demonstrated in this study and this study).
•In a human study, 50% DMSO was found to produce partial anesthesia (numbness) to pinpricking sensation, while a questionable reduction occurred with 20%, and no effect was observed with 10% DMSO.
•Isolated frog sciatic nerves immersed in 6% DMSO for 30 to 120 minutes developed a 40% decrease in conduction velocity. Normal conduction velocity returned after the nerves were washed for one hour in Ringer’s solution.
Superficial radial nerves were isolated from adult cats and immersed in 75% DMSO for 60 minutes. Nerve conduction was totally abolished in the smaller nerve fibers (thought to be important in pain perception), but was reversible if the DMSO was washed off immediately once nerve conduction disruption began. Another author found that immersion in 5% to 10% DMSO completely blocked conduction in small peripheral nerve fibers from cats.
Note: DMSO temporarily blocking neurologic transmission may also treat pain by resetting pain circuits (as other methods that do this are highly effective for many of the challenging conditions DMSO also treats).
Finally, DMSO has been shown to induce total anesthesia in animals when injected directly into the cerebrospinal fluid and to do so without causing any adverse reactions.
Choline Esterase Inhibition
The body has a variety of regulatory processes which in tandem allow it to maintain a steady internal state despite being exposed to numerous external stressors. One of them is to eliminate the neurotransmitters it produces so they do not excessively stimulate nerves. In turn, certain drugs (e.g., SSRI antidepressants) work by preventing this elimination, thereby raising the levels of a target neurotransmitter.
One of the key neurotransmitters in the body is acetylcholine, which serves a variety of functions such as being the primary neurotransmitter of the parasympathetic (rest and relax) branch of the autonomic nervous system. Acetylcholinesterase inhibitors raise acetylcholine within the body by preventing its breakdown enzyme from eliminating it. These drugs in turn have a variety of functions, such as increasing parasympathetic activity or improving memory, but likewise if used excessively can cause a dangerous overdose known as “cholinergic syndrome.”
Note: years ago I tried numerous memory aids for studying and found the most effective one was a natural acetylcholine esterase inhibitor (which also had the side effect of creating vivid and lucid dreams).
Decades of research (e.g., this 1966 study, this 1966 study, this 1975 study, this 1983 study, this 1991 study, and this recent 2017 study) have shown that DMSO is an acetylcholine esterase inhibitor (and that it increases the pre-synaptic release of acetylcholine). That property in turn is believed to account for DMSO lowering the threshold for the vagal nerve to fire and DMSO’s powerful ability to increase parasympathetic function in the body (e.g., DMSO increases the response of the smooth muscle of the stomach to both muscle and nerve stimulation) and also to help with improved memory and concentration (although that could also simply be from improved cerebral circulation).
However, unlike other acetylcholine esterase inhibitors, at high doses it hasn’t been observed to cause a cholinergic syndrome (which may be because while under 1% DMSO is an acetylcholine esterase inhibitor, over 10% blocks cholinergic transmission, or because it is a competitive rather than irreversible inhibitor, or as the previously cited studies show, because its inhibition is significantly weaker than the pharmaceutical drugs used as acetylcholine esterase inhibitors).
Note: one of the few adverse effects of IV DMSO is certain individuals experiencing a partial reduction of the heart rate, which is likely due to DMSO’s effects on the autonomic nervous system.
Furthermore, in addition to enhancing parasympathetic function, DMSO also blocks the inhibitory effects of the sympathetic nervous system, both of which counteract the sympathetic symptomatology commonly seen in autonomic disorders.
Note: this property may also contribute to DMSO’s pain-relieving effects as existing research shows acetylcholine esterase inhibitors reduce chronic pain.
Anti-inflammatory:
Many of my colleagues who used DMSO in practice primarily used it for inflammation. It was incredibly effective in this regard, and unlike the other dangerous options (e.g., steroids or NSAIDs), DMSO is very safe. Since inflammation is a key component of both pain and musculoskeletal injury (e.g., “chronic inflammatory pain” is well recognized), this property likely is key to DMSO’s utility in those conditions.
In the first part of this series, to help illustrate how DMSO can protect injured tissue from death (and allow non-healing brain or spinal cord tissue to heal), I provided the evidence (like this study) showing DMSO:
•Reduces pathologic inflammatory responses to tissue injury
•Reduces inflammatory cytokines.
•Reduces the production of inflammatory prostaglandins and increases the production of anti-inflammatory prostaglandins.
•Neutralizes (scavenges) free radicals, which are both a cause and result of chronic inflammation and a common cause of tissue injury, degenerative illness, and chronic pain.
In turn, numerous animal studies have shown shown DMSO prevents inflammatory stimuli from creating inflammation and tissue damage:
•In guinea pigs, locally applied DMSO was effective in inhibiting both the development of DNCB (an irritating chemical) induced contact dermatitis and local swelling.
•In rats, pressure necrosis was prevented by pretreatment of the skin with 70% DMSO, Carrageenin induced edema in their paws was reduced by topical but not oral administration of DMSO (as was zymosan-induced edema), DMSO prevented adjuvant-induced arthritis (and in another study attenuated adjuvant induced arthritis), topical DMSO inhibited traumatic edema induced by intrapedal injection of autologous blood in the leg of a rat, and DMSO prevented the formation of granuloma-pouches. DMSO (70%) also prevented contact dermatitis, allergic eczema, and calcification of the skin.
•In rabbits, DMSO counteracted the Shwartzman phenomenon by suppressing inflammation if administered prior to injecting an inflammatory bacterial lipopolysaccharide and reduced inflammation when injected into joints with croton oil induced arthritis.
•In horses, topical DMSO prevented the severe inflammatory reaction they typically experience from small doses of purified human gamma globulin they have been sensitized to (which leads to areas becoming so inflamed and edematous that the horses will not move their necks and frequently become necrotic).
Six horses with LPS induced synovitis in their mid-carpal joints received topical (90%) DMSO gel, and compared to controls were found to have a decrease in joint inflammation (e.g., less neutrophils present). Additionally, DMSO was found within both the joints and serum.
A rabbit study found that in rabbits with fractured hind legs, the daily application of DMSO reduced the eventual stiffness in their ankles by 41%.
Additionally, as shown later in this article, numerous studies show DMSO prevents tissue injury from chemotherapy drugs, which is likely due to its anti-inflammatory properties. Likewise, as I will also show later in the article, DMSO is highly effective at healing naturally occurring injuries in animals with an inflammatory component.
Note: a study which evaluated ultraviolet light’s ability to produce an inflammatory response that killed melanocytes in the skin found that DMSO caused an increased density of melanocytes, which again suggests DMSO facilitates a better recovery of the inflammatory response.
Muscle Relaxation
DMSO tends to relax skeletal muscle while simultaneously enhancing the contraction of other muscles (e.g., 3-6% DMSO enhanced the contraction of the heart and stomach).
DMSO applied topically to the skin of patients produces electromyographic evidence of muscle relaxation 1 hour after application, while another study found 50% DMSO prevented the contraction of frog skeletal muscles.
A 1966 study found that (as shown by electromyography) muscles in spasm will relax within 60 minutes of topical application. It also found that this relaxation could be used to treat headaches associated with cervical disease and complex regional pain syndrome.
As muscle tension is a frequent cause of pain and musculoskeletal disorders, this property likely accounts for some of its efficacy for those conditions.
Treating Pain with DMSO
As opioids are seen as the gold standard for pain control, there is very little awareness research has shown a comparable analgesic exists. To illustrate:
•A 1983 study using a common research metric (how mice respond to heat and tail flicks) found that DMSO produced an analgesic effect comparable in strength to morphine. However, this effect was assessed to be due to a different mechanism as an opioid receptor blocker (naloxone) did not affect DMSO’s ability to eliminate pain, DMSO did not produce any of the side effects seen with opioids, and DMSO’s effect lasted far longer (4-6 hours and in some cases over 24 hours—whereas in contrast morphine typically lasted less than 2 hours).
•A 2008 mouse study using similar tests also found that DMSO blocks pain.
•In a 2013 study of with morphine-induced thermal hyperalgesia, intraperitoneal 10% DMSO (5 mL/kg) reduced paw withdrawal thermal latency shortening by 6 and 10 days and lowered spinal cord dorsal horn TNF-α expression compared to controls.
However, unlike other analgesics (pain killers), DMSO has a variety of unique properties. These include:
•It treats a very wide range of pain conditions, including ones other analgesics can’t address. For example, case reports exist of DMSO treating phantom pain (pain outside the body where an amputated limb had previously existed).
•Rather than the body developing a resistance to it (which is what commonly happens with opioids), DMSO often becomes more effective at eliminating pain with subsequent doses, and in many cases, is needed less and less frequently (or not at all because the condition is resolved). Because of this, while acute pain rapidly responds to DMSO, chronic pain conditions often take 4-7 days of applications for DMSO to begin taking effect and 6-8 weeks for lasting relief to occur (e.g., to quote one patient “after twenty-four DMSO injections, I was completely pain-free”).
Note: DMSO has also been shown to treat post-amputation pain.
•In many cases, as is seen with other applications of DMSO, the effect is systemic (e.g., one study found 65% of patients experienced pain relief if DMSO was applied at the site of pain, whereas 61.5% experienced comparable relief when DMSO was applied somewhere further away in the body).
Additionally:
•DMSO (especially topical DMSO) tends to be more effective in treating pain above the waist, and is less likely to help the larger joints (e.g., the hips have the smallest response to DMSO). In turn, the pioneer of DMSO would typically use injections rather than topical applications for the hips and knees (although we’ve found the knees frequently respond to topical DMSO).
•In acute cases (e.g., an ankle sprain), DMSO is often applied every 2-3 hours, and in many cases, the broader an area that is covered with DMSO (and the more DMSO is used), the more effectively DMSO relieves pain.
•In chronic pain patients who do not respond to topical DMSO, a lower concentration of injectable DMSO often helps.
•Shingles (which will be discussed in a later part of this series) consistently has an excellent response to DMSO.
Cancer Pain
Many cancer patients experience severe pain (which increases as the cancer becomes terminal), and in 10-20% of cases, it does not respond to standard opioid management. In many cases however, it does to DMSO. For example:
•A study gave two older patients with cancer pain DMSO, one of whom had an excellent response to treatment and one who had a good response.
•Another study found that of 7 patients with metastatic cancer pain, DMSO gave 2 a full remission and 2 a partial remission.
•One of the most well known examples was Otis Bowen MD (a popular second term Indiana governor) who “illegally” used topical DMSO to treat his wife’s pain from terminal multiple myeloma and then publicly denounced the FDA’s absurd embargo on it at the AMA’s 1981 national meeting. Remarkably, a few years later, Bowen became Reagan’s Secretary of Health and Human Services, but even then, with this highly ethical doctor at the helm of the HSS, DMSO was unable to overcome the FDA’s prohibition of it.
Headaches
Tension headaches (e.g., those caused by muscular tension of the neck) and sinus headaches tend to respond to DMSO (with relief typically lasting 4-6 hours), whereas migraine and cluster headaches are less responsive to DMSO. For example, in addition to the previously mentioned study where DMSO was found to both relax the cervical musculature and alleviate tension headaches, these results were reported by two doctors:
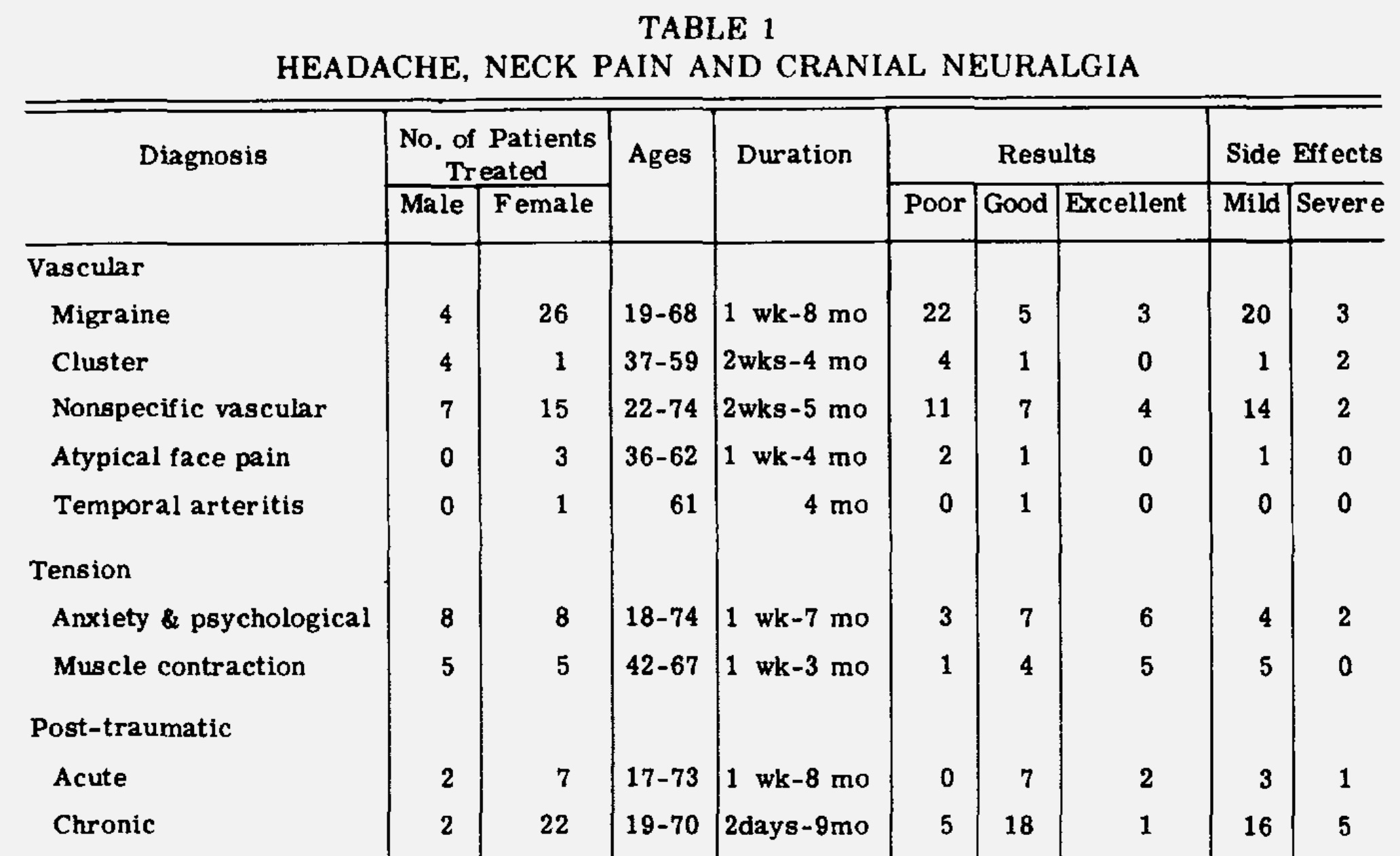
Note: many headaches are incorrectly categorized as migraine headaches. Additionally, migraine headaches typically only respond to DMSO if it’s applied during the early stages of the headache.
Many other headaches also respond to DMSO. For example, Stanley Jacob reported on 59 patients with headaches from a variety of causes, of whom over 75% responded to DMSO. This included 13 out of 17 patient with years of chronic neck pain from cervical arthritis that triggered headaches, (who then required a gradually decreasing DMSO dose), 4 out of 5 patients with sinus headaches improved from DMSO, 2 out of 2 patients with temporal arteritis (causing severe head pain) who fully recovered after DMSO and 26 out of 35 patients who’d had trigeminal neuralgia for more than a year with numerous failed treatments (13 of whom then had a full recovery).
Likewise, another study of 10 patients with headaches (from a variety of causes—the majority being frontal) found DMSO significantly helped all 10 (including in those who had had a headache for more than a day).
Finally, a study of 15 patients with tinnitus (another condition which responds to DMSO) included 11 who had concurrent headaches. For those 11, DMSO resulted in 7 having a complete recovery, 1 having less intense headaches, 2 only having occasional headaches and 1 having no response.
Note: there are numerous testimonials of individuals with years of headaches who experienced life-changing results from DMSO.
Fibromyalgia
Over the years, I have heard of quite a few cases of individuals with fibromyalgia having a massive improvement in their quality of life from DMSO (e.g., one can be found here) but simultaneously, I’ve also seen quite a few cases where it needed to done slowly for a sensitive patient (as otherwise the initial detoxification response was too much for the individual).
Note: this principle is also important to keep in mind when working with other “sensitive” patients (which is discussed further here).
While no formal literature has been published in this area, the leading pioneer of DMSO therapy (who I consider to be extremely honest) attested:
Over the last few years, we have been treating patients with fibromyalgia. Seventy percent of the patients have experienced benefit. No serious side effects have been encountered.
The properties of our regime contributing to benefit included free-radical scavenging, analgesia, anti-inflammation, softening of scar tissue, reduction of muscle spasm, and stimulation of healing.
Spinal Pain:
Many of the most profound benefits from DMSO are found in patients with spinal issues (e.g., spinal stenosis, a failed back surgery, surgical scars, severe arthritis, previous spinal cord injuries, or bulging discs), and numerous testimonies (e.g., many can be found in the Congressional hearing) exist of individuals who had been in years of crippling pain suddenly getting their lives back because of how effectively DMSO treated their pain and restored their mobility.
However, while I frequently read case reports of this, I have only located one which specifically evaluated this. In that 1968 study, 38 patients with lumbar and cervical disc problems received conventional (non-surgical) treatments and half also received DMSO—which was found to halve the treatment time they required.
Note: topically applied DMSO is often extremely helpful for herniated discs (and much safer than systemic steroids). Additionally, a few people found injecting DMSO mixed with lidocaine into the vertebral musculature was quite helpful for spinal pain.
Since studies are lacking in this area, I will instead share a few testimonies (most of which can be found within the previously mentioned Congressional Hearing).
Point blank, I myself am one of the individuals who I treated with DMSO for a slipped disc, and I can tell you point blank that it works better than anything else I have ever tried before or since DMSO therapy.
At 46, I was a deformed arthritic mass of pain from a childhood injury which shortened my left leg by healing with a short bend. Physicians thought I had been born with one leg shorter than the other; and this caused a severe curvature of the spine and, with age, arthritis.
Two hours after my first DMSO treatment, I felt a buzzing in my knee and my leg straightened—after 34 years. I then had treatments on my back. My spine is still curved, but nothing like it was. I am straight, my hips and shoulders lateral, not forward with an enlarged hip, and the lump of muscle doesn't show. I no longer have osteoarthritis in my knee and, at 51, I can drive a car long distances and teach a class in college. Before DMSO, I couldn't walk a block or ride 10 minutes in a car.
I, myself, have realized almost complete freedom from pain since being injected with DMSO by Dr. Stanley Jacob. My pain was due to scar tissue formed around the sciatic nerve as a result of two lumbar disc surgeries and would drop me by surprise to the ground—thus causing a constant need for pain medication and the use of a cane, for walking. After two (2) shots of DMSO I was able to quit using the cane, and after about six (6) shots of DMSO by Dr. Jacob I was able to stop using the pain medication. I now feel better than I have since before I got hurt, and owe it all to Dr. Jacob and DMSO.
Would you please use your influence to legalize DMSO? Our daughter broke her neck in an auto accident and for the first time in years pain free because of using DMSO.
I am writing regarding DMSO. I am 75 years old, veteran and an R.N. I have a service connected back, 5 operations, plus 2 after my discharge on my back. I feel that after my spinal fusion in 1950, that I had excellent results, but in the last few years have had arthritis through my entire spine.
My doctor finally told me that there was just nothing left for him to do, to try DMSO. He did not tell me how or where I could get it. Tried veterinarians but had no dog, yes, I had no dog, so I couldn’t get it. Finally found a kind gentleman who told me where I could get it.
Thanks to the Foundation in Portland, I was able to get it, and needless to say, I'm thankful. I won't say that it has cured any of my aching joints, but I’ve been able to stay on my feet, instead of in a wheelchair.
Note: I suspect a key reason DMSO is so effective for spinal pain is that spinal joints are relatively small, and DMSO has the most positive effects on smaller joints (e.g., the fingers).
Additionally, there are also many stories of quadriplegics who initially took DMSO to alleviate their chronic pain and then gradually regained motor function as a “side effect” of DMSO. In turn, there are many cases (listed here) of individuals overcoming lifelong paraplegia (including “hopeless” cases where their “miraculous” improvement could be traced to DMSO as it stopped once DMSO was withdrawn). This for example was a testimony of a mother whose child was saved from a lifetime of paralysis by DMSO:
During the last six months, have spent many hours in Dr. Jacob’s clinic with his beautiful and caring staff, watching miracle after miracle happen right in front of my eyes. I have seen people who have been totally paralyzed for twenty years or more being treated and starting to move. The wonder in their eyes indeed a sight to behold.
Complex Regional Pain Syndrome
Complex regional pain syndrome (CRPS), is a chronic pain condition that is characterized by also having autonomic and inflammatory involvement. Other than it frequently following a trauma (e.g., a surgery) and being linked to small fiber neuropathy, the causes of CRPS are still not well understood and management of this challenging condition typically consists of a plethora of pharmaceutical drugs targeting each symptom.
This is a shame as there are few unorthodox therapies which effectively treat CRPS, one of which is DMSO (which as mentioned before blocks pain from the small fibers). Sadly however (like the other CRPS treatment options) there is very little knowledge of DMSO’s unique applicability to the condition.
Note: complex regional pain syndrome was an adverse event associated with the HPV vaccine.
The supporting evidence is as follows:
•A 1985 study demonstrated that 50% DMSO reduced the inflammation associated with CRPS and improved symptoms associated with the condition.
•A 1994 study treated 13 CRPS patients (within 3 months of diagnosis) with 50% DMSO and found they had a significantly better recovery than the comparative treatment.
•A 1996 study of 32 patients with acute CRPS (e.g., heat, redness, pain, swelling, reduced range of motion) gave them 50% DMSO or placebo for 2 months, and a significant improvement was seen in the DMSO group.
•A 2003 study randomized 64 patients with CRPS to receive topical 50% DMSO and 67 patients to receive n-acetyl-cysteine (NAC) for 17 weeks to a year. This study found that DMSO was a cost effective therapy that produced good to excellent results for the patients, especially when their CRPS was associated with inflammatory symptoms and when it was done earlier in the illness.
•Another 2003 study of 146 patients also comparing 50% DMSO to NAC (over 24 months) found DMSO was effective, particularly for hot (inflammatory) CRPS.
•A 2012 study gave 29 patients (who had had CRPS for less than a year) 50% topical DMSO and found DMSO significantly reduced their pain (with results approaching a complete absence of pain), brought back the functionality of the affected limb and improved their quality of life.
•A 2012 study used a combination of treatments including 50% DMSO for CRPS and found this combination was effective for treating the condition.
•Another 2012 study gave topical DMSO 50% cream, applied 5 times daily for 1 month and then 3 times daily for a year, reduced pain in 29 patients with type 1 complex regional pain syndrome (CRPS). The visual analogue scale (VAS) score decreased by 3.09 points (from 7.6 to 4.6), indicating a shift from intense to moderate pain. Quality of life improved by 1.36 points on the Likert scale, with 89.7% of patients showing improvement. Limb function increased, with range of motion improving by 12.03 and strength by 3, achieving moderate overall function. Patients reported pain relief (51.7%) and reduced stiffness (34.5%).
•A 2016 study used a compound analgesic cream (CAC) containing ketamine 10%, pentoxifylline 6%, clonidine 0.2%, and DMSO 6-10% was evaluated in 13 CRPS patients. Nine patients (69%) reported reduced pain/symptoms (mean pain score decreased from 6.3 ± 1.9 to 4.4 ± 2.1). Six patients had sustained benefits after 2 months, with two achieving complete pain/symptom resolution (one with early CRPS-I, one with partial CRPS diagnosis). The CAC showed promise as part of multimodal therapy for CRPS, particularly for early cases, with potential to alleviate symptoms effectively.
•Finally, a 2005 review of the existing therapies for CRPS concluded 50% DMSO had evidence of efficacy and compared to the other treatment options, was the least likely to cause harm.
Additionally, to highlight that these benefits extend to neuropathic conditions besides CRPS, another study found that of 9 patients with peripheral neuritis segmental neuralgia, DMSO gave 6 a full remission and 2 a partial remission.
Surgical Pain
Since DMSO both accelerates wound healing and reduces pain, it is uniquely suited to post operative pain. Numerous studies support this. For example:
•A rat study found administering DMSO into a wound before closing it significantly reduced the subsequent pain and guarding the rats had, suggesting this approach could address a common complication of surgery.
•A 1967 study found that DMSO applied to the incision sites of thoracotomy (open chest surgery) patients in concentrations of 60% to 80% resulted in significant pain relief, and reduction of the opioids needed (which in turn led to fewer gastrointestinal complications). These patients as a group were able to cough more effectively, move more easily both in and out of bed, resume early motion of the arm and shoulder, and in general enjoy a more rapid and less complicated postoperative course.
•Another study gave 90% DMSO to 64 postpartum women with episiotomy pain and found that over half had pain relief and a reduction in swelling and that there was a significant improvement in mobility (with some patients who had left the hospital then requesting to resume DMSO to alleviate subsequent pain). The investigators ultimately concluded the risks (e.g., a burning sensation from the DMSO) did not outweigh the benefits of the therapy—something I suspect may in part have been due to them using too high a concentration of DMSO on a sensitive region of the body.
•Another study treated 37 post-surgical patients with chronic intractable pain syndromes and noted excellent relief in 32 of them.
Other Pain Studies
•In a 2024 randomized placebo-controlled trial, 62 patients with plantar fasciitis applied a topical solution of phytoterpenes with 15% DMSO, 1% limonene, and rosemary oil as penetration enhancers twice daily for 10 days. This caused an 85% or greater reduction in pain scores in 78.1% of patients whereas no improvement was seen in the placebo group.
•DMSO gel with Synthalen LP carbomer, applied externally, effectively reduced inflammation and pain with high stability and bioavailability.
•DMSO-gel (25%) applied twice daily significantly outperformed placebo in a study of 68 patients with vertebrogenic dorsalgia, reducing pain, muscle syndromes, and daily functioning disorders while improving spinal function, as assessed by questionnaires and examinations before and after treatment . Other studies have also shown DMSO treats vertebrogenic lumbar pain.1,2
•At the Orthopedics Department of Xi’an Red Cross Hospital in Shaanxi Province, a compound preparation containing dimethyl sulfoxide (DMSO) was used to treat muscle and joint pain in the lower back and limbs in 300 patients, a common condition among laborers. The treatment achieved favorable short-term results, with high efficacy, rapid onset, minimal side effects, and simple application, making it a commonly used therapy in the hospital’s outpatient clinic.
•In patients with Hand-Arm Vibration Syndrome (a condition caused by prolonged exposure to vibrating tools or machinery), topical DMSO reduced pain and inflammation, improved microcirculation, and provided anticoagulant and immunosuppressive effects when applied to the skin, often having a synergistic effect when combined with other drugs.
•DMSO in combination with metamizole treated pain syndrome in children with aseptic necrosis throughout the body.
•DMSO in combination with infrared irradiation and a halogen alkali (likely potassium iodide) was used to treat 121 patients with rheumatic pain.
•DMSO reduced tongue pain and inflammation in patients with glossalgia.
Wound Healing
Due to its properties, DMSO tends to accelerate wound healing, prevent wounds getting infected, eliminate pain, heal chronically non-healing wounds and prevent the formation of scar tissue or dissolve it once present (a property which may relate to its remarkable ability to eliminate amyloid aggregates throughout the body). Because of this, there are many accounts of individuals saying they’ve benefitted greatly from applying it immediately after wounds (typically around the wound rather than inside it).
Note: a reader who did his PhD in physical and organic chemistry shared that his research had shown DMSO could change the molecular bonding of atoms in its vicinity, which allows it to greatly accelerate biochemical reactions. Assuming this is true, it might help to explain why DMSO accelerates healing.
Ulcers
Note: as shown in the previous article (and for instance in this commenter’s experience), varicose veins and ulcers have an excellent response to DMSO.
A large study of chronic skin wounds (which in many cases had remained untreatable for years or were infected) found 95.04% had a complete recovery (e.g., no burn scars) following DMSO that was often quite rapid. The conditions treated were as follows:
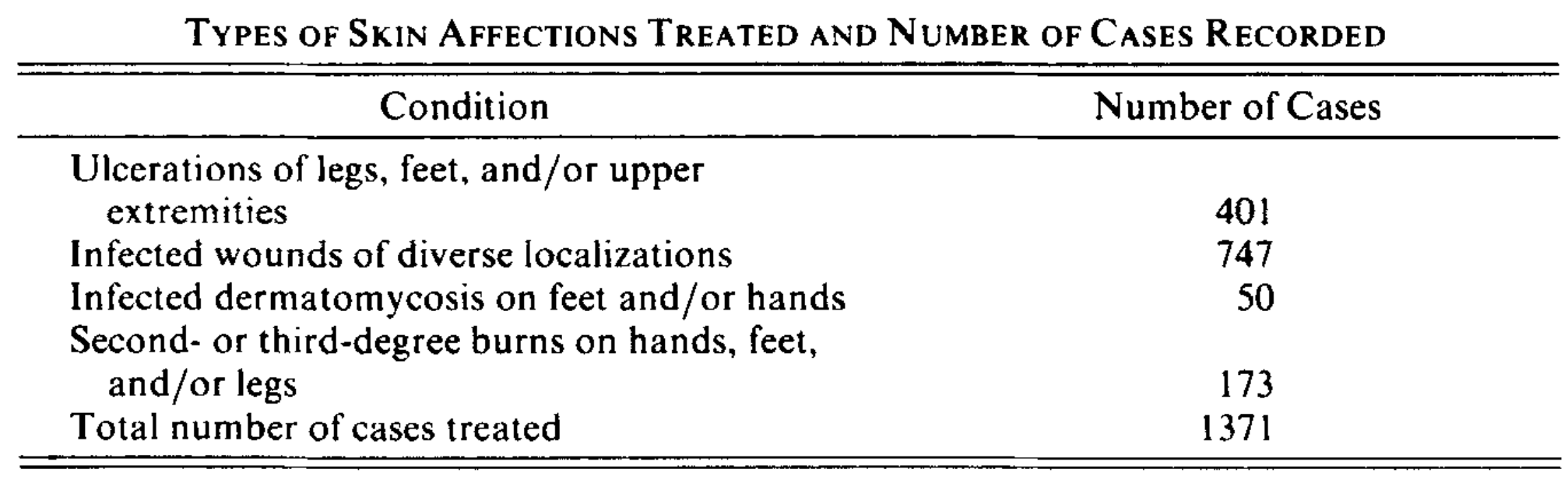
Note: the investigators reported that certain patients with deep wounds experienced some pain at the time of DMSO application. However, this pain only lasted a short time and did not prevent DMSO treatment. Most patients received immediate relief after DMSO, and in some cases, the pain completely stopped after the first treatment.
A systematic review examined the efficacy of topical DMSO on wound healing and noted that decubitus ulcers were the most frequently studied condition. Overall, the review found that DMSO was beneficial for wound healing and analgesia (and had low toxicity).
Note: this analysis included a 1985 study where 20 older diabetic patients with chronic (treatment resistant) perforating ulcers received DMSO and 14 had a complete recovery in 4-15 weeks of treatment (whereas in contrast only 2 of the 20 controls who received conventional treatment did), a double blind trial where DMSO was used as an adjunctive therapy for refractory duodenal ulcers and was found to increase the cure rate from 60% to 100%, and an unpublished trial where 39 elderly patients with first stage pressure ulcers received 5% DMSO for 36 months and had a very positive response to the treatment.
Additionally, since chemotherapy drugs are cytotoxic, a variety of common injuries occur with them, with one of the most common (an extravasation injury) occurring when the drug leaks out of blood vessels and injures the surrounding tissue (and skin). Extravasation injuries affect approximately 1% of chemotherapy patients (estimates range from 0.1%-6.0%), and create significant issues for patients. DMSO in turn, has successfully treated a variety of common chemotherapy injuries, particularly extravasations and ulcers (e.g., see this rat study, this rat study, this rat and pig study, this pig study, and this guinea pig study).
In humans, case reports exist of DMSO treating these injuries (e.g., see this report, this report of two cases, this report and this report), alongside larger datasets (e.g., here 4 out of 4 chemotherapy injuries responded to DMSO, here 8 out of 8 did, and here 74 out of 75 did). Finally, prospective clinical trials have also corroborated this (e.g., in this study 20 out of 20 patients responded to DMSO, while in this study 16 out of 20 did).
Finally, when used on open wounds in horses, DMSO was found to rapidly stimulate healthy granulation tissue, decrease excessive granulation tissue, and both eliminate existing infections in the wounds and prevent new infections.
Tissue Regeneration
DMSO has the unique property of accelerating the speed at which newts regenerate lost limbs by approximately 2-3 days (see this paper and this dissertation).
Note: newts are one of the only advanced organisms which can regenerate a lost limb.
Additionally, authors of a 1998 Russian paper stated that they are routinely applying DMSO into surgical wounds as it accelerates healing and provides general infection control. This in turn is congruent with the pain studies mentioned earlier in this article that show DMSO improves the healing of surgical wounds.
Scar Tissue and Adhesions
DMSO is often used to treat scars. This may be in part due to DMSO being observed to disrupt the links between collagen fibers
Note: Matrix metalloproteinases degrade the proteins that surround cells. While their function is essential, when excessive, they (especially MMP-9) are linked to a variety of disease states (e.g., organ fibrosis, cardiovascular disease, cancer, and rheumatoid arthritis) due to the healing process becoming disordered. DMSO in turn has been shown to attenuate excessive MMP-9 activity.
In rats, DMSO decreased experimentally induced intestinal adhesions (a common complication of abdominal surgeries) by 80%. Additionally, another study found DMSO inhibits fibroblastic proliferation in vitro.
Note: it has been observed that DMSO is much more likely to prevent adhesions if administered prior to surgery rather than after it.
In rabbits, when 70% DMSO was administered next to a wound incision (but not the incision site itself), 70% DMSO appeared to increase the development of wound tensile strength—which is important since a major issue in surgery is the incision sites dehiscing (ripping open) and because an early improvement of a scar’s tensile strength suggests the scar that ultimately forms will be stronger and healthier.
Another rabbit study applied DMSO immediately after surgically wounding their backs and found that after 7 days, their scar tissue was significantly stronger than that of untreated controls. Finally, a third rabbit study administered DMSO 4 weeks after an injury to their ears and found that DMSO prevented hypertrophic (excessive) scar formation.
Note: surgical scars take about 6 weeks to develop, and in most cases are around 80% as strong as the original tissue that preceded them. This again suggests that using DMSO would significantly improve longterm surgical outcomes.
Finally, DMSO is also sometimes used to repair keloid scars. For example, in one study of ten people with keloids, applying 50-80% DMSO a couple of times a day induced scar flattening with loosening of the collagen surrounding the fibrous bundles. Similarly, another study found DMSO eliminated subcutaneous fibrosis induced by radiation (through a gradual softening and reduction of it). A third study discussed using DMSO for the treatment radiation pneumonitis in lung cancer patients, and a fourth found DMSO could prevent radiation reactions in the skin while a fifth explored DMSO’s use in the overall treatment of local radiation complications.
Note: this author also found DMSO had a concentration dependent effect on the wound healing process.
Skin Flaps and Grafts
•Surgically created skin flaps are at an increased risk of dying due to poor blood perfusion. Numerous studies (e.g., this one, this one, this one, this one, this one, this one, this one, this one, this one, this one, this one, this one, this one, this one, this one and this one) have shown DMSO protects vulnerable skin flaps from death (including in a rat model of smokers and women receiving masectomies), which makes it a shame it is not used in fields that could greatly benefit from this innovation (e.g., plastic surgery).
Likewise, skin grafts, even from the same person, often fail. Fortunately, DMSO happens to address the common causes of skin graft failures. To illustrate, a Ukrainian plastic surgeon documented that in over 500 transplants that dressings moistened with 30% DMSO solution for 3-5 days enabled grafts to take and survive in badly burned patients and victims of elephantiasis (e.g., there was no skin necrosis, no inflammatory changes, no keloids, and no hypertrophic scars). Similarly, a study of 120 rabbits demonstrated the DMSO significantly improved the viability of a skin or cartilage graft.
Note: in rabbits, DMSO was shown to reduce tissue carbon dioxide levels, and when mixed with hydrogen peroxide, increase oxygen levels, but this effect was not seen in rats or pigs.
DMSO and Musculoskeletal Injuries
While DMSO is a remarkably effective painkiller and wound healing agent, by far its number one use was the treatment of musculoskeletal conditions, particularly those which created a functional immobility. In turn, many of the early adopters of DMSO went from skeptics to believers because of the rapid and dramatic improvements they saw from it (e.g., as they had patients with a debilitating bursitis in the shoulder recovering within minutes of receiving DMSO).
Due to its safety and dramatically better performance than the existing treatment options, DMSO rapidly took off around the country. Numerous pharmaceutical companies clamored for it (and invested millions in bringing it to market), and before long, many doctors were using it on thousands of patients with unbelievable results—results that were particularly unbelievable given how poorly the existing therapies worked.
Sadly however, as both the public and professional interest in DMSO was skyrocketing, the FDA decided it was unacceptable a drug they could not control was taking off around the country, and on November 10, 1965, issued a global research ban on it, causing almost every doctor who had been using it to stop out of fear of prosecution. This immediately created an underground market for DMSO, a flurry of complaints to and by elected officials over it (which eventually resulted in Congressional hearings) and an end to almost all DMSO research.
Note: the reason for the ban was completely unjustified as the existing evidence showed the FDA’s safety concern did not exist, and later was conclusively disproven by a large human toxicology study.
As a result, very little knowledge now exists of DMSO’s use in human musculoskeletal injuries other than it existing in a few products where it was combined with another agent (e.g., there are numerous FDA approved topical DMSO-Diclofenac [an NSAID] preparations), and it having the sole approval for treating interstitial cystitis (which will be discussed later in this series). Remarkably however, it is fully permitted in veterinary medicine (which led to a lot of Americans using DMSO that was “meant for horses”) where it is acknowledged to create the same benefits that were observed in humans.
Being fully aware something like that ban was being considered by the FDA, DMSO’s advocates decided a research symposium under the auspices of a prestigious organization needed to be held to head it off and throughout 1965, despite immense pressure from the FDA not to host it, the scientific community rallied behind them. The program gradually came together (in a manner far different from our modern scientific community):
The March 14, 15, and 16, 1966, symposium under the auspices of the New York Academy of Sciences was held in a large hall of New York's Waldorf Astoria Hotel. More than a thousand researchers came from all parts of the United States and from overseas. After the FDA had cracked down on DMSO, Jacob had written to every person who had submitted an abstract, he said that now that DMSO had been branded toxic and dangerous by the FDA the paper could be withdrawn. No one canceled.
Note: 82 papers were presented at this meeting which was attended by over 1000 researchers from across the world.
This timeline in turn explains how a wealth of compelling data emerged over a very brief period of time—and then just as suddenly stopped. Likewise, much of the research at this time was in the initial stages (e.g., it was produced by doctors who had switched to reviewing all of their charts from when DMSO had been used since they could no longer give it to patients) most of these studies were comprised of a wide range of musculoskeletal issues (those that their patients presented with) rather than being restricted to a single complaint. For this reason, I felt it was best to present most of them by sharing the key data tables of each study. Doing so in turn makes it clear DMSO consistently had an 80-90% success rate in treating thousands of musculoskeletal issues—something dramatically better than any of the options which existed then or that exist now…..60 years later.
Note: what I am alleging here is understandably difficult to believe. That was why I began this series by providing the wealth of evidence DMSO effectively treats “untreatable” brain and spinal cord injuries (e.g., strokes) and justifying the contention that millions could have been spared a lifetime of disability or paralysis if the FDA had not suppressed it (along with making a similar case for other incurable conditions DMSO treats like Down Syndrome and amyloidosis). Likewise, there are many other important facets to the DMSO story (e.g., exactly why the FDA did this or how DMSO treats other challenging disorders like tinnitus, macular degeneration, and scleroderma) I felt should not be presented until a clear and unambiguous case was made to how unconscionable the FDA’s conduct was in these first two articles
Human Musculoskeletal DMSO Studies
One of the first studies was published in 1965 and conducted by the researcher who courageously pioneered the adoption of DMSO throughout the United States:
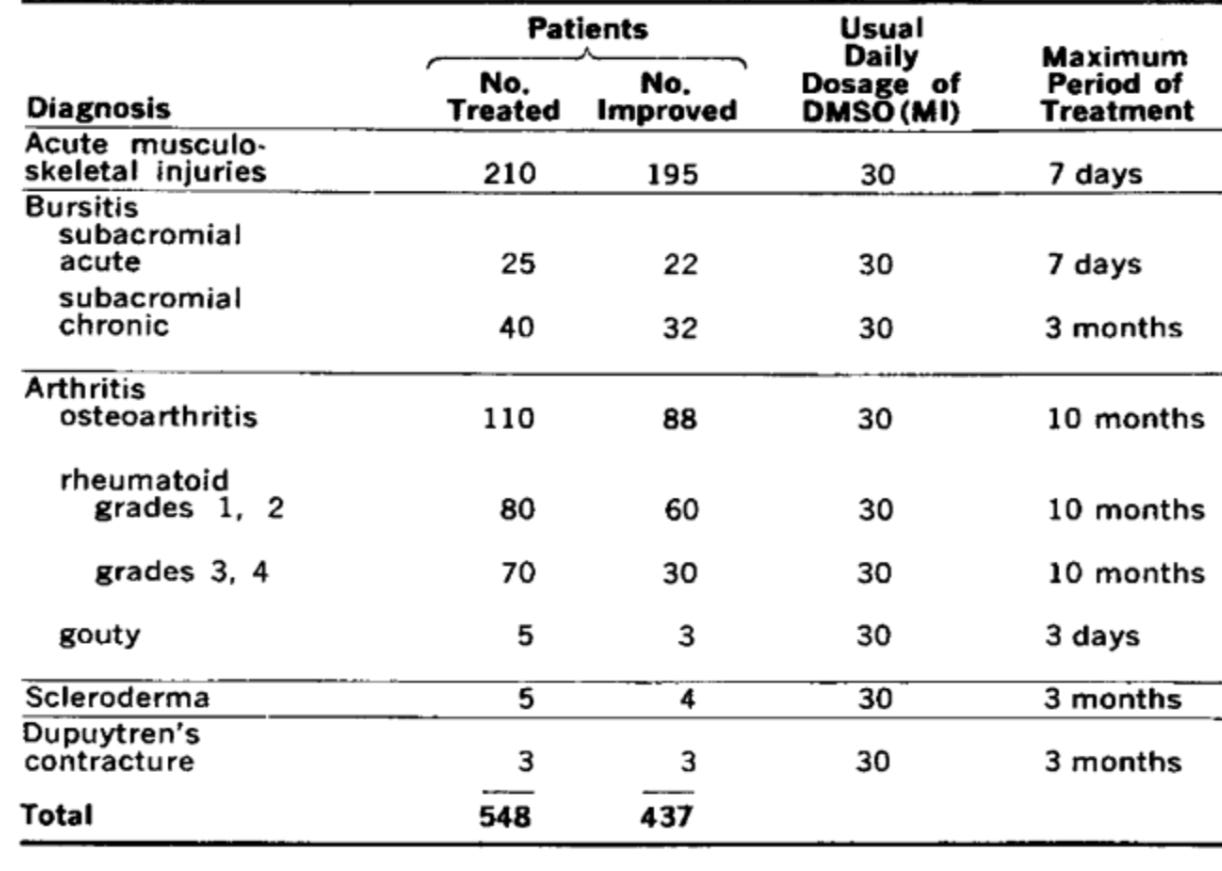
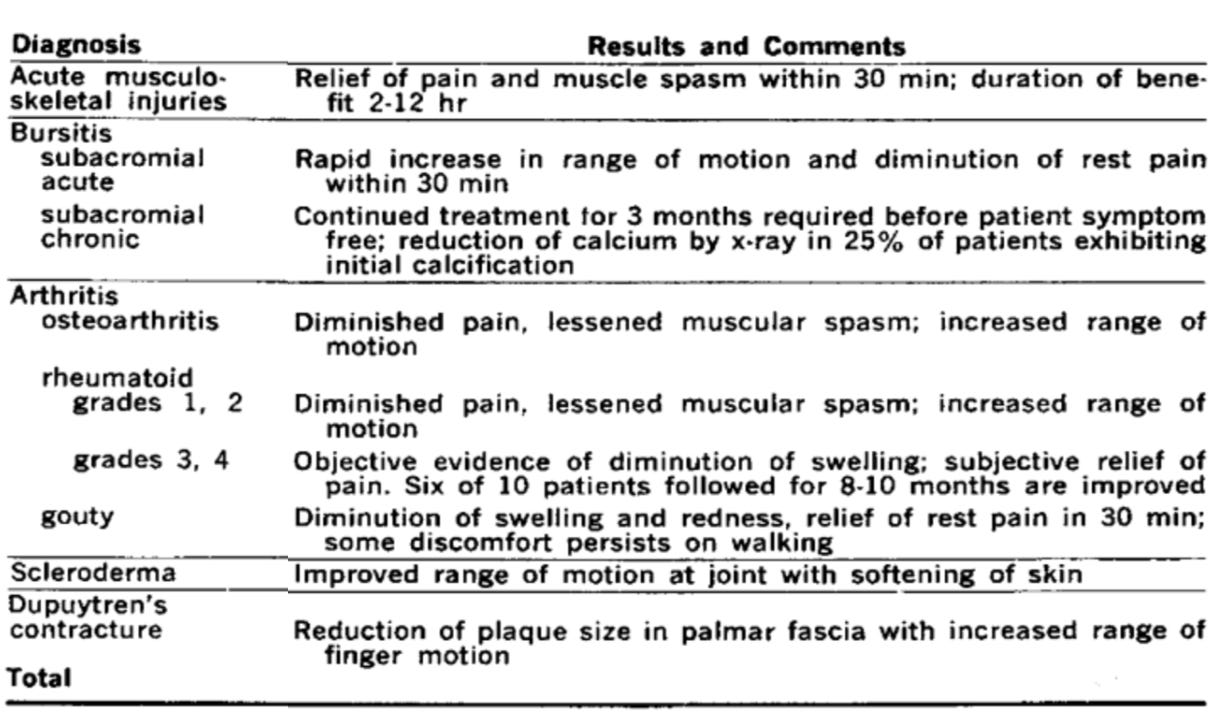
This in turn was followed by numerous 1967 studies. The largest of which found:
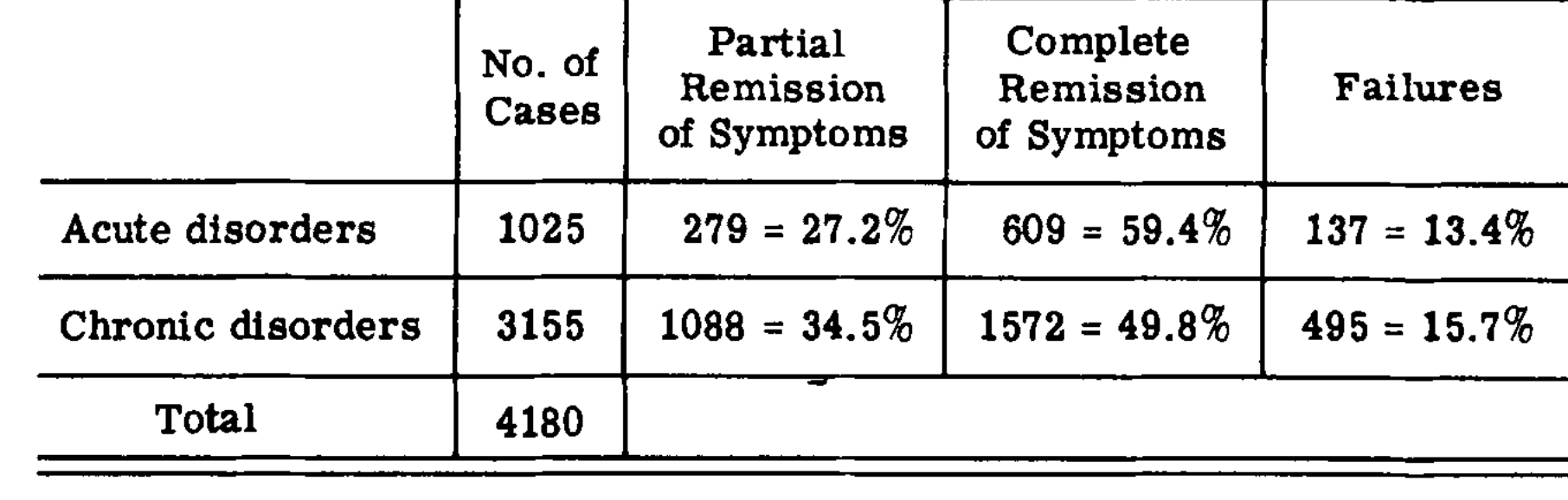
Some of those disorders included:
Note: this study also included x-ray images of painful calcifications at the trochanteric bursa, supraspinatus attachment and greater tuberosity disappearing from DMSO. However, while DMSO has often been observed to eliminate calcifications, other therapies (e.g., neural therapy) are sometimes also required to accomplish this.
In that study, many of the results were immediate and dramatic. For example, this was one bursitis patient:
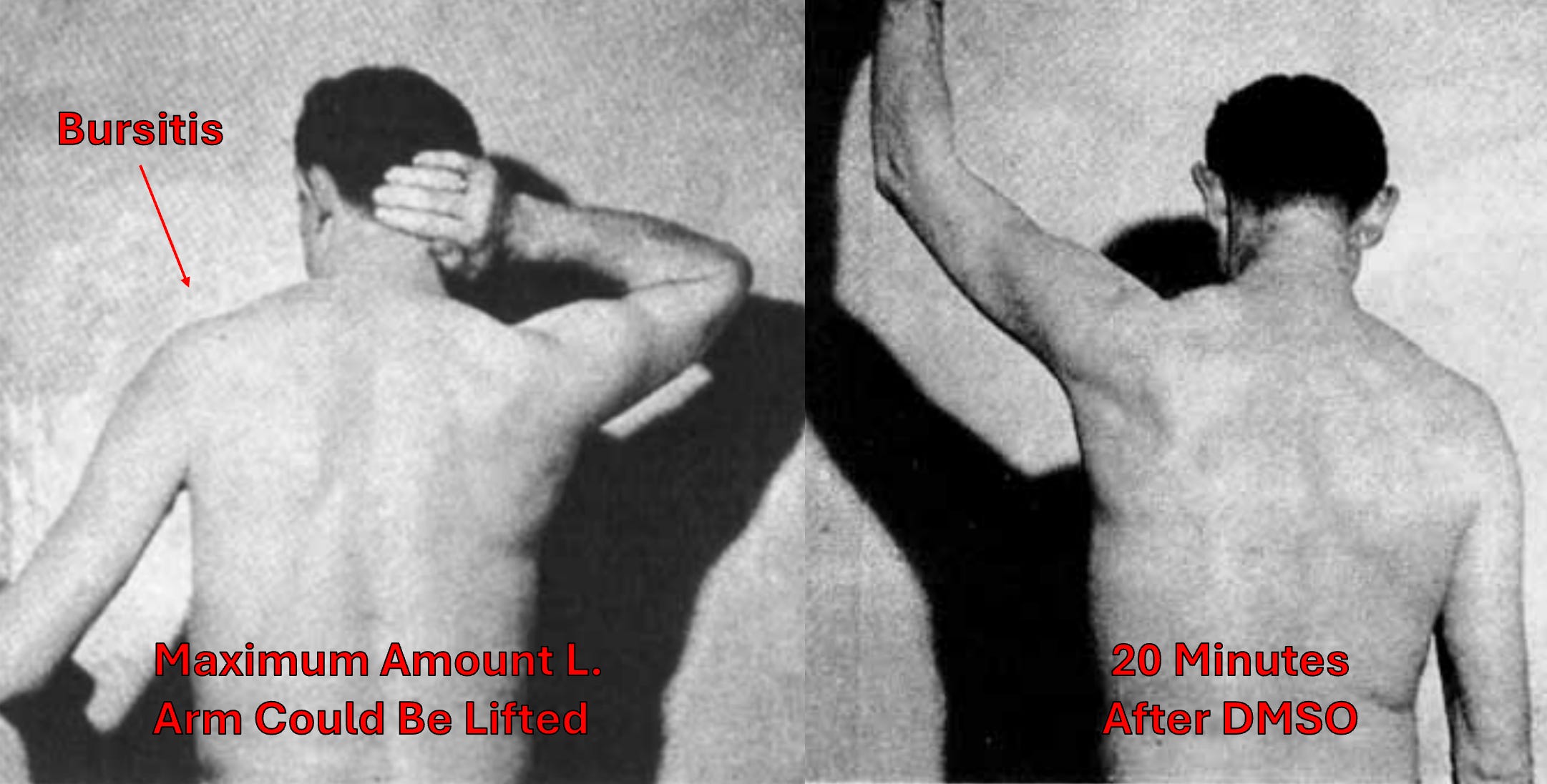
Note: in another 1964 study, 22 out of 25 patients with subacromial bursitis experienced a rapid improvement within 30 minutes of DMSO, while in chronic cases 32 of 40 patients improved, but in many cases 3 months of treatment were required for improvement. Additionally, in some patients, a reduction in calcium deposits was also noted.
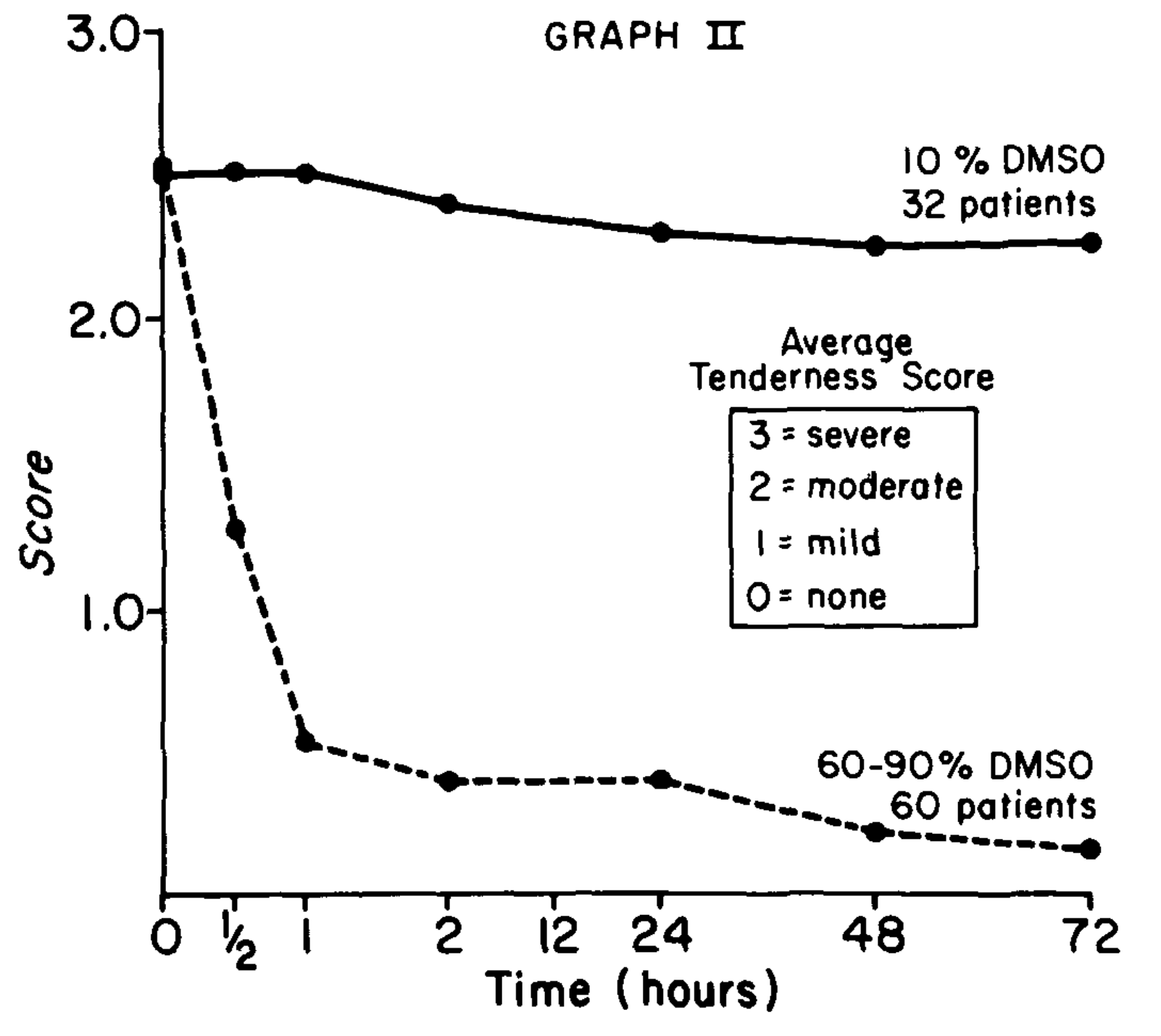
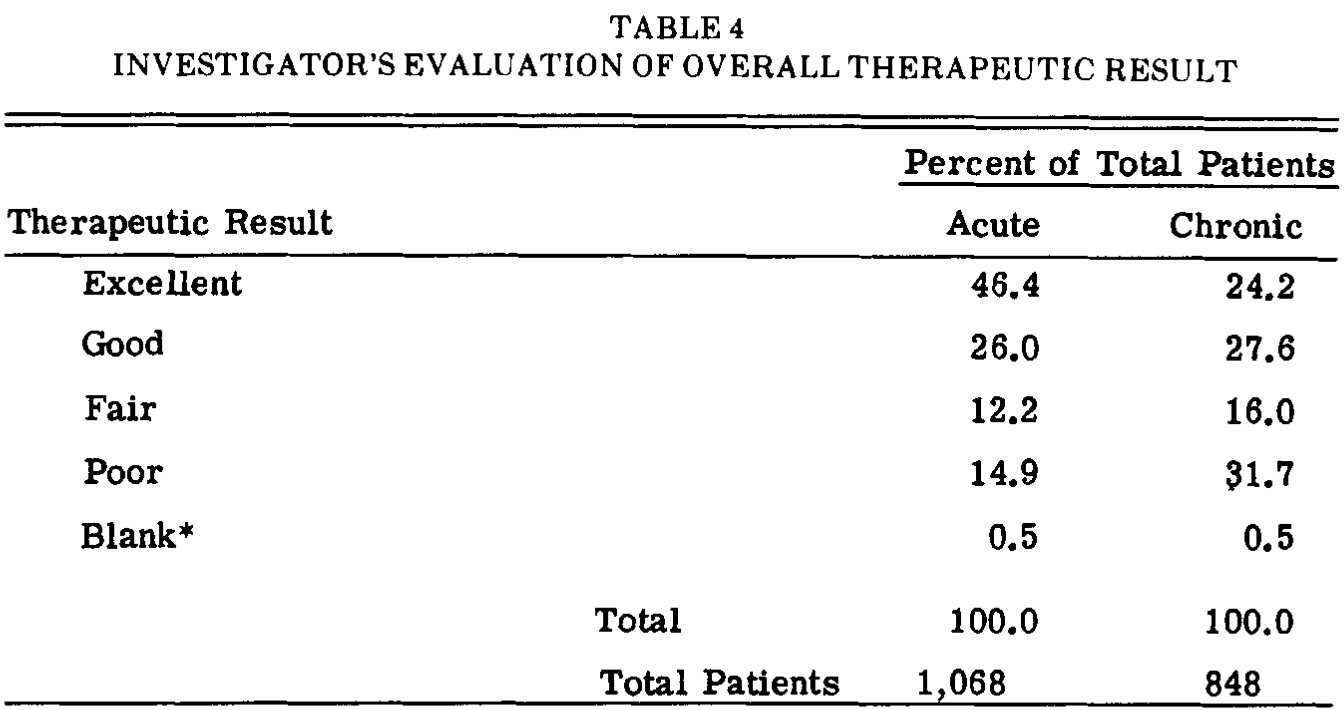
Another 1967 study found:
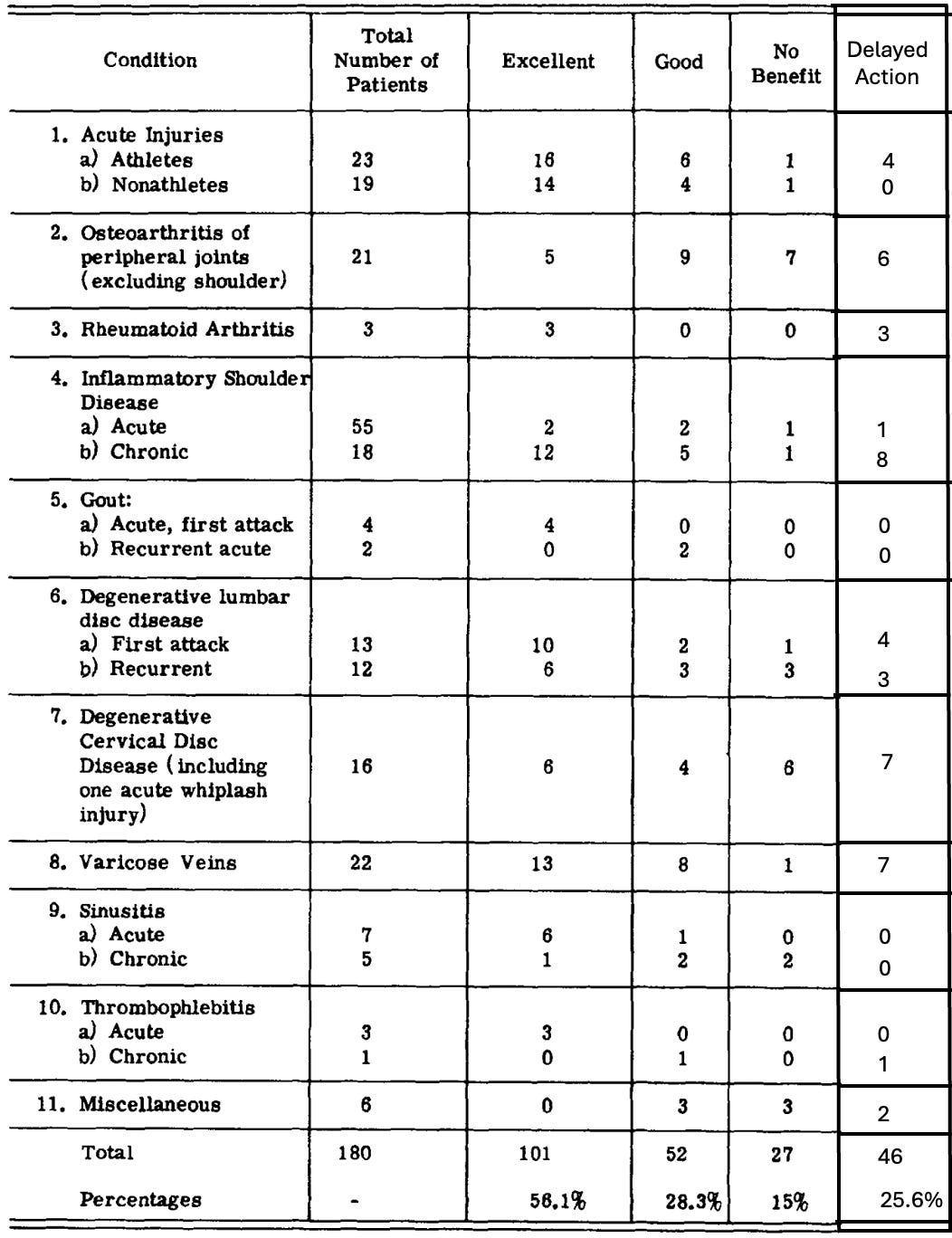
Note: a key point these researchers emphasized was 25.6% of their patients, particularly the chronic ones, had a delayed response to DMSO (which is important to recognize as in chronic conditions DMSO can initially appear to not be doing anything). These researchers hypothesized this may have been due to them giving DMSO 1-2 times a week rather than 1-2 times a day.
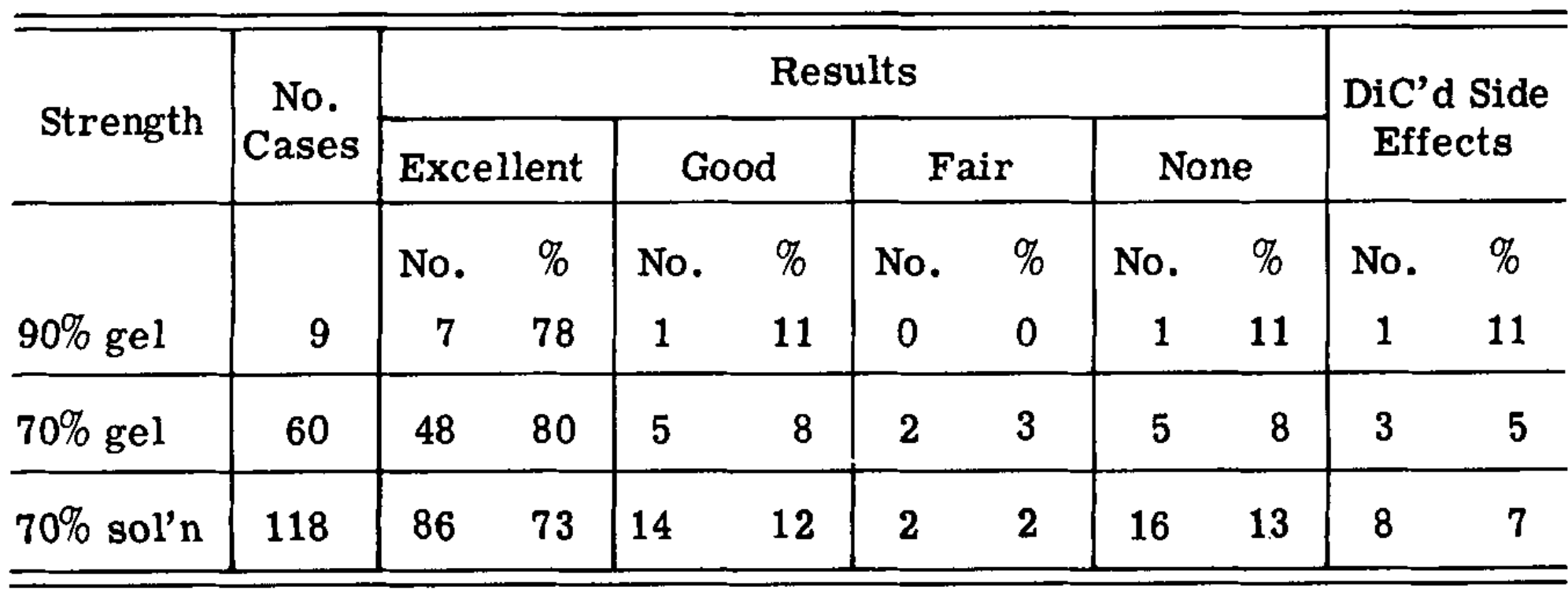
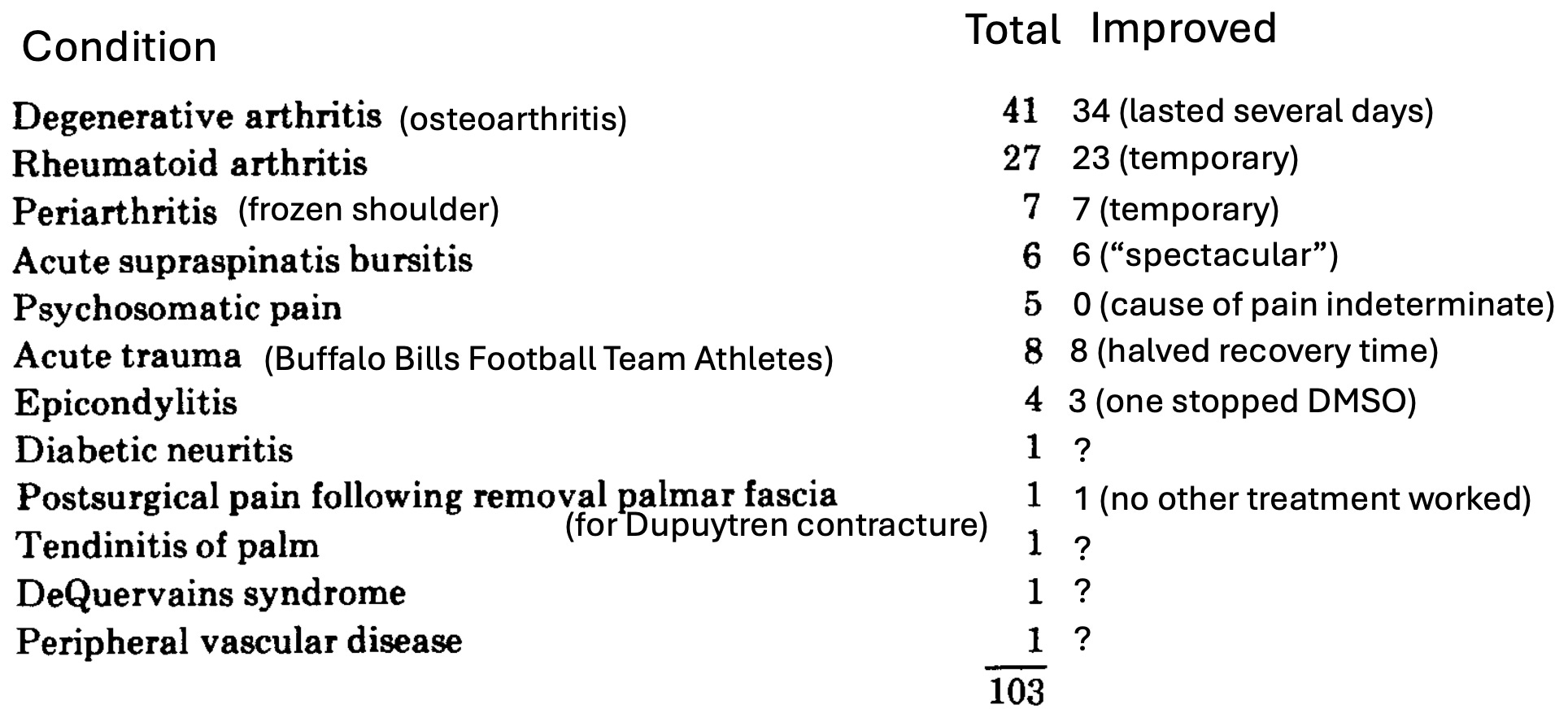
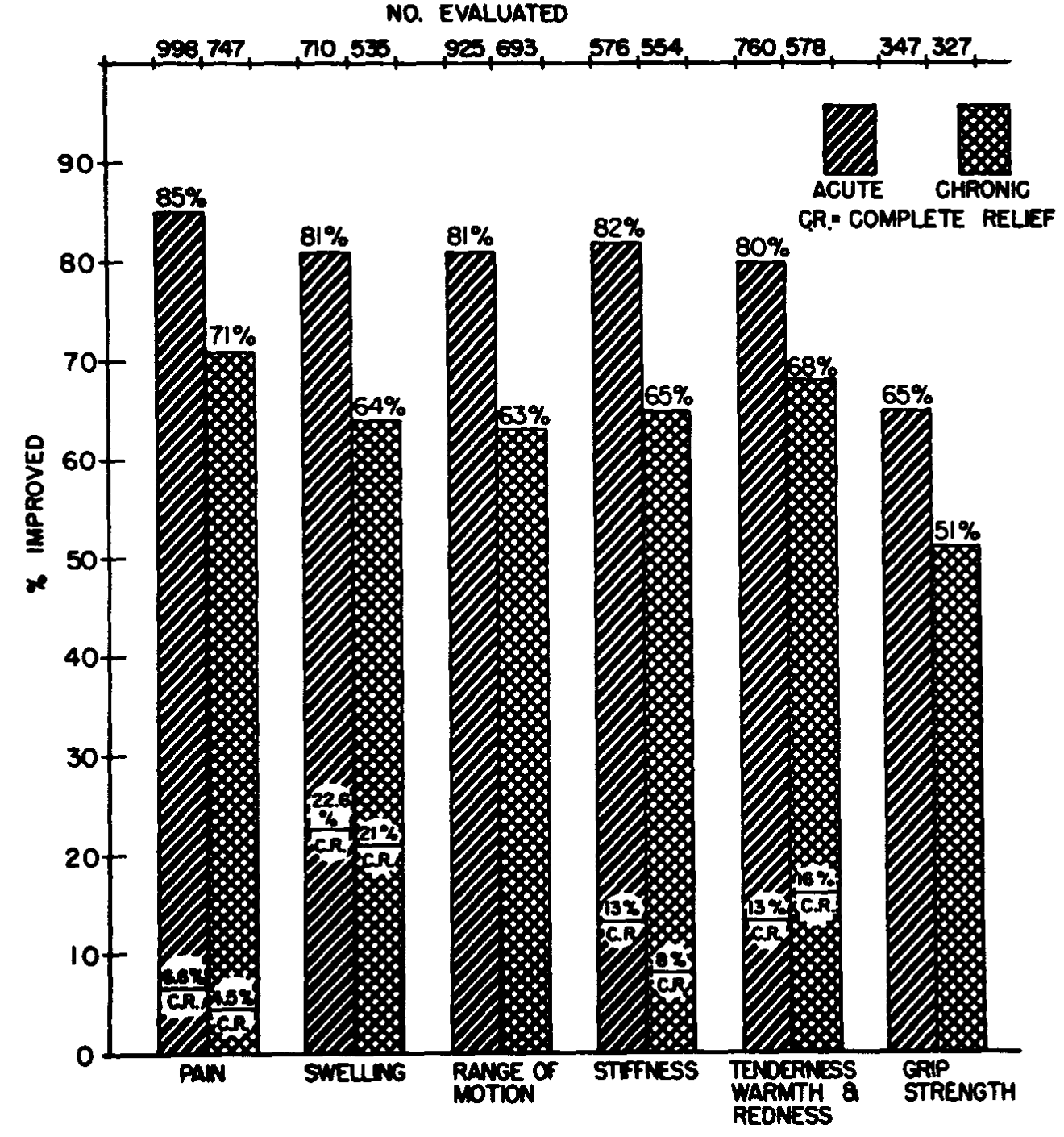
•Another 1967 study also had similar results:
•A 1967 blinded study for acute musculoskeletal disorders, using 10% DMSO gel as a “placebo” found:1,2
In that study, its author (a former president of the Aerospace Medical Association) remarked:
I am convinced that topical application of DMSO in the treatment of acute musculoskeletal conditions is a striking and significant therapeutic contribution. During the period of time I conducted clinical investigation with this medication, I practically discarded physical therapy as treatment for musculoskeletal problems because the rehabilitation of my patients was so prompt with DMSO. There was little or no necessity to prescribe narcotics and tranquilizers since pain was promptly mitigated following topical application of DMSO.
He then conducted a follow-up double-blind study (using either 80% or 10% DMSO gel) on patients with sprains, strains, bursitis, or tendinitis. The study found that the active treatment had significantly better results than the placebo and significantly reduced the time patients lost from work.
Note: a 1969 study treated rheumatoid arthritis with 10% DMSO and found no benefit from that dose.
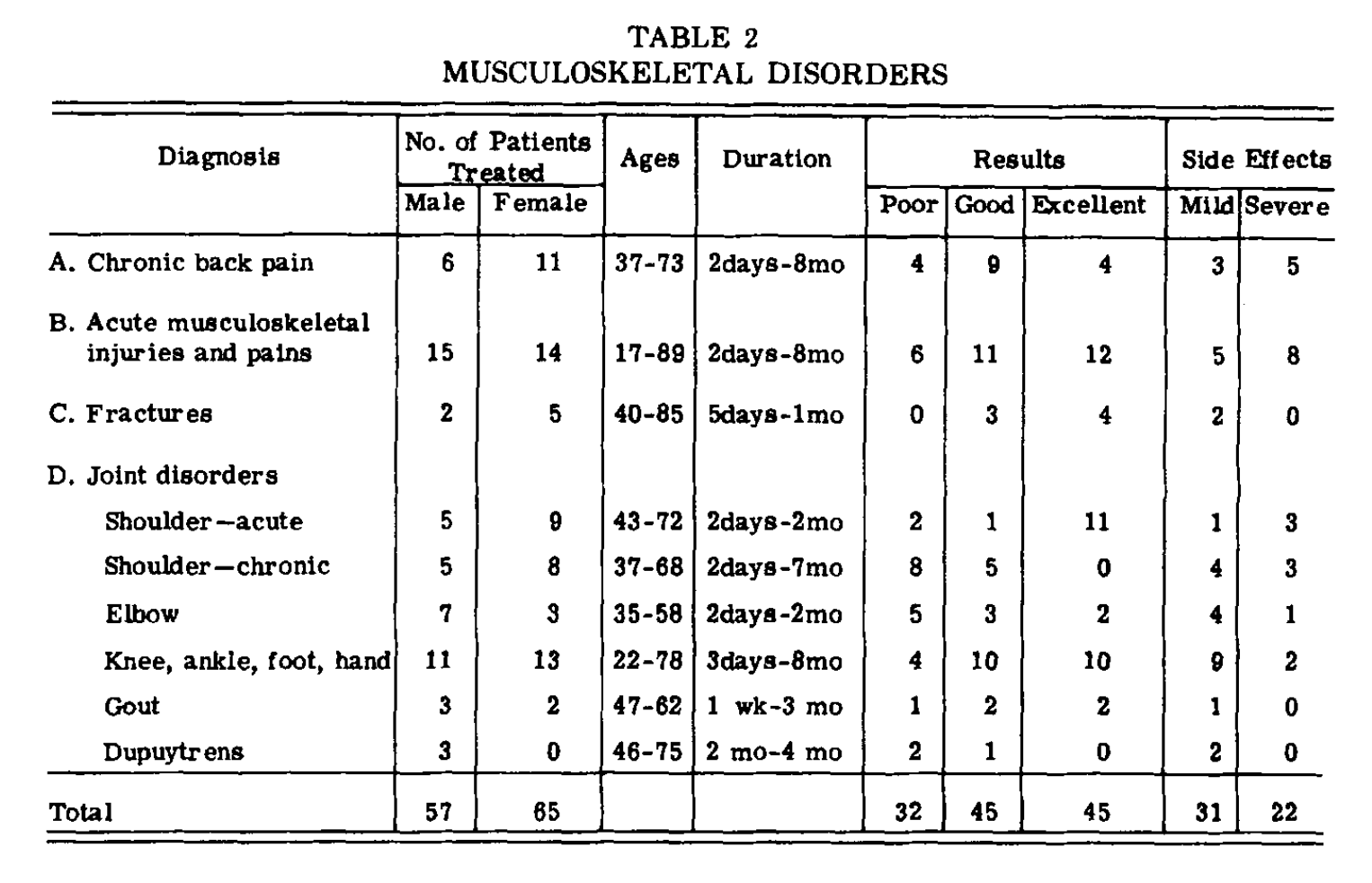
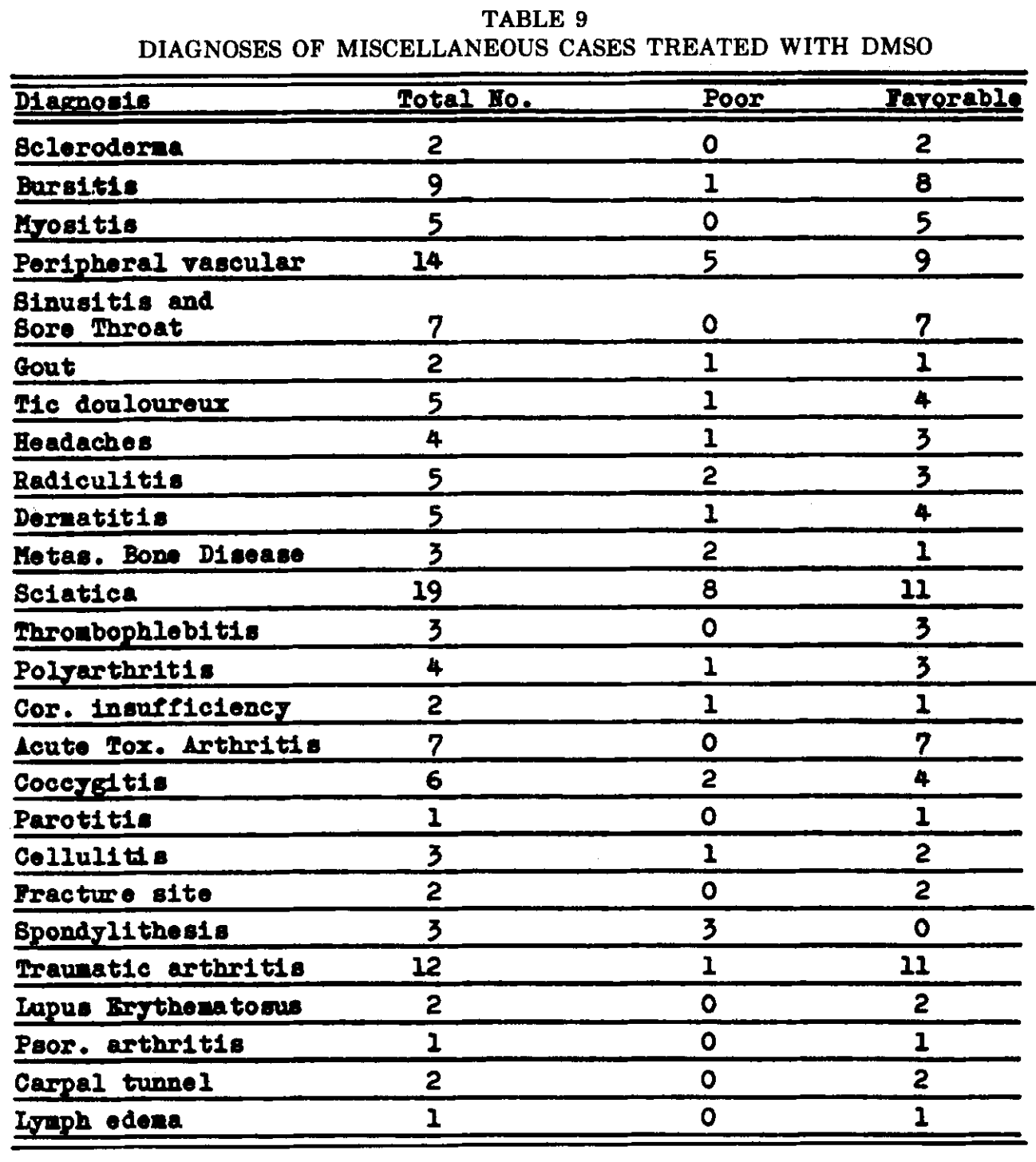
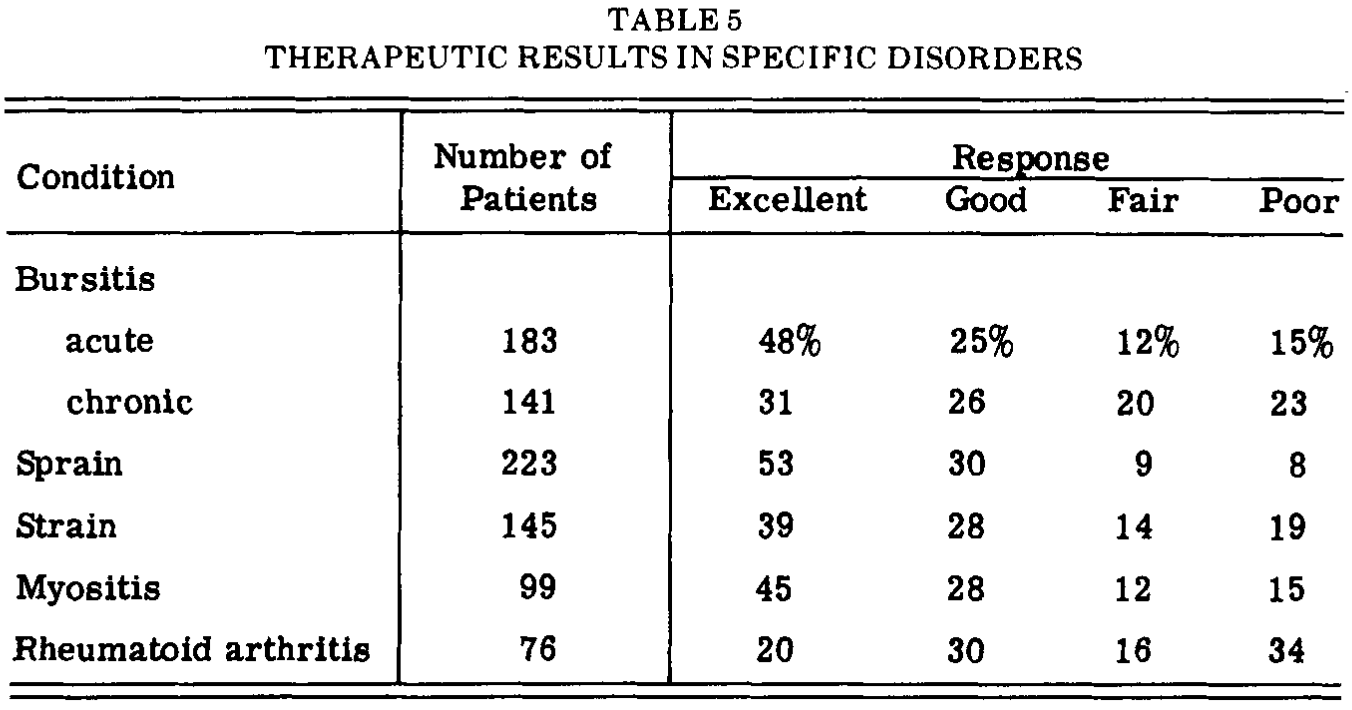
•Another 1967 study found:
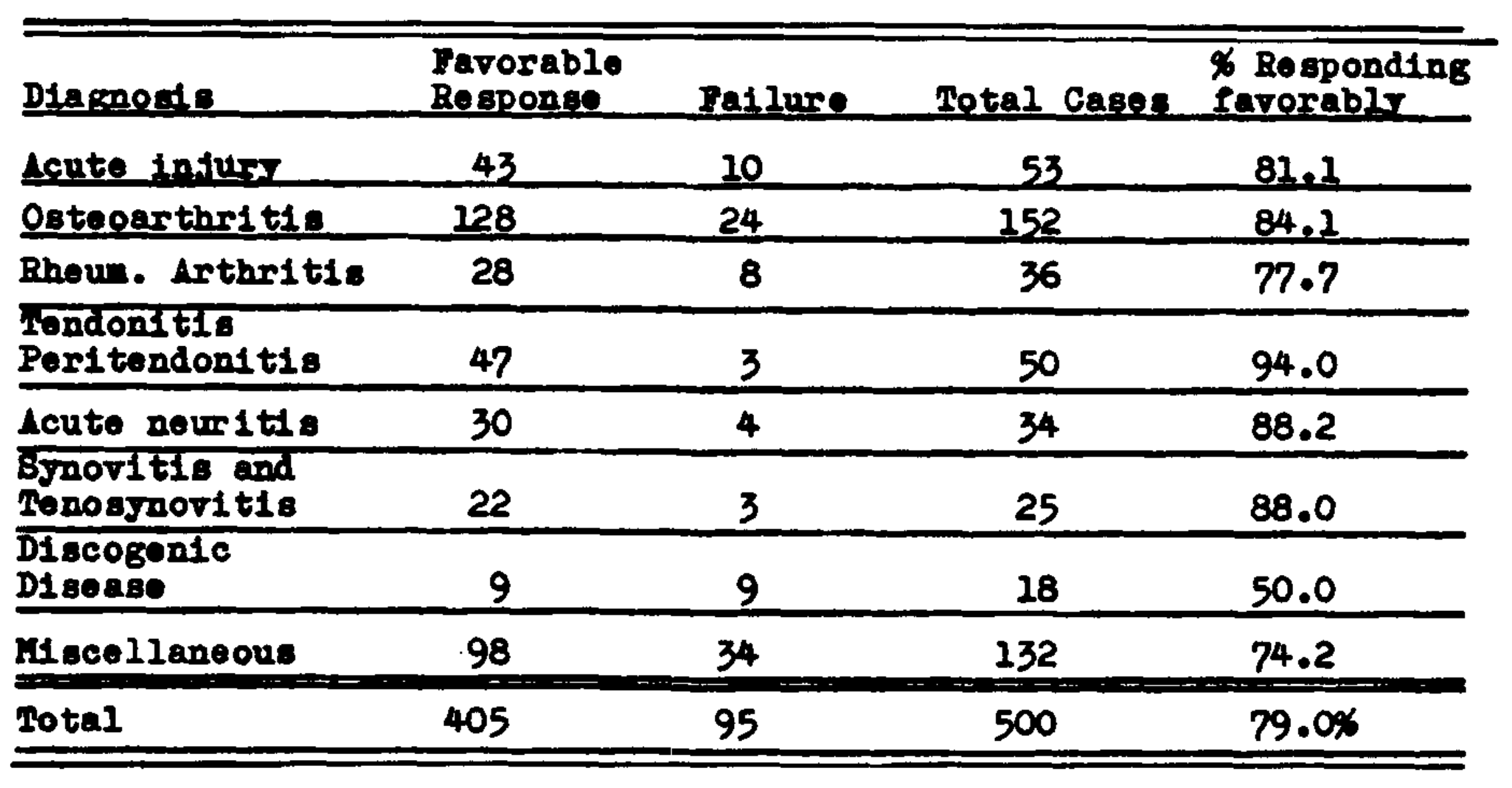
The miscellaneous cases were as follows:
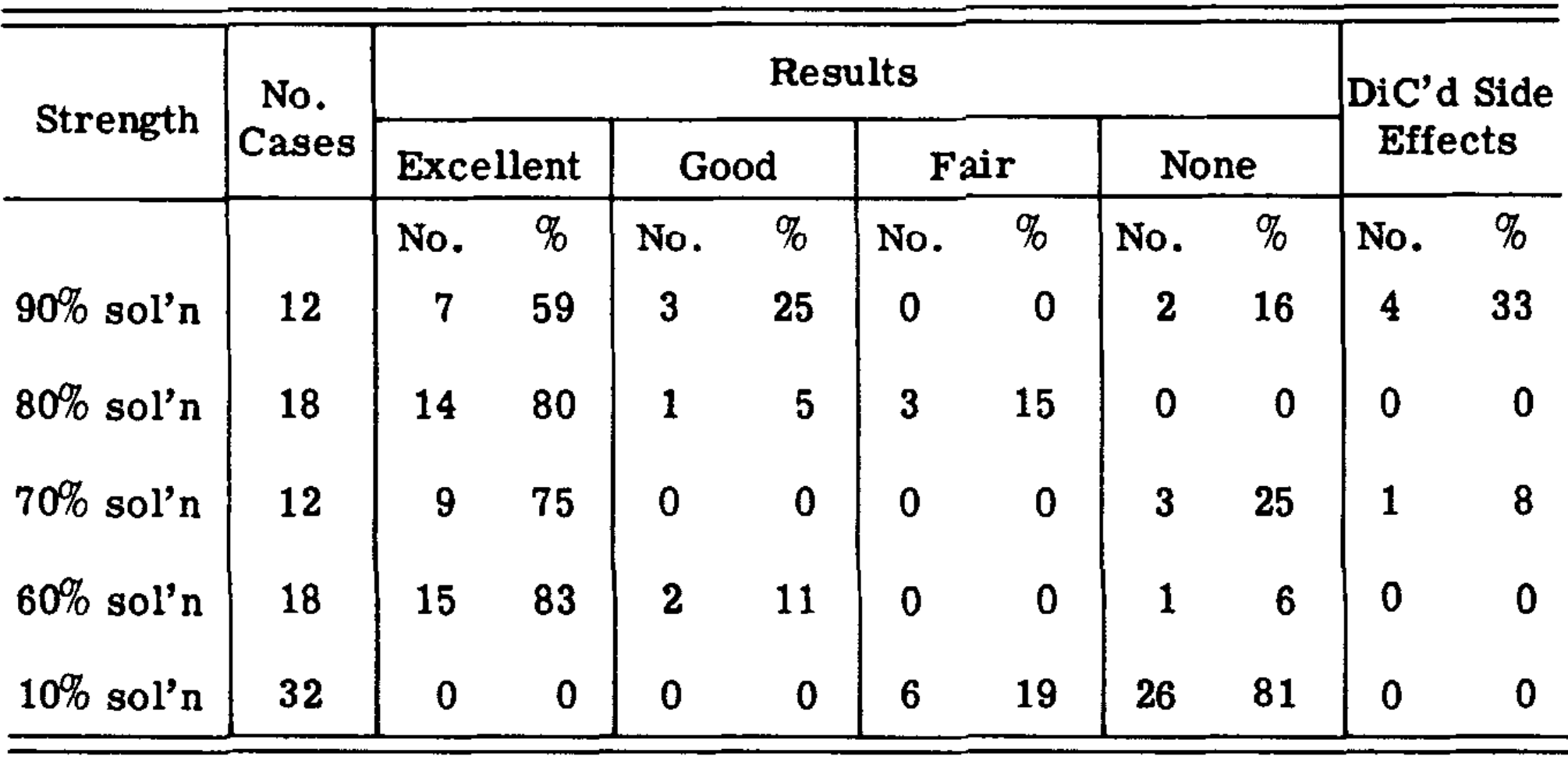
•Another 1967 study found:
Note: another study gave PT and 70% DMSO to 7 people with frozen shoulders, 4 of whom had excellent pain relief and improved motion. Other investigators also found that frozen shoulders respond to DMSO but can require anywhere from 5 to 24 applications (and sometimes more).
•A 1994 blinded study gave 157 patients with acute tendinopathies (e.g., tennis elbow) 10% DMSO gel or a placebo ointment three times a day for 14 days within 3 days of symptoms starting. Pain of movement under loading and the mobility of the joints were significantly improved after, respectively, 3 and 7 days of treatment with DMSO, as compared with placebo. After 14 days on DMSO, a further improvement was observed, and 44% of the patients were pain-free (placebo 9%).
Note: DMSO has also been found to be effective for carpal tunnel syndrome (and other hand issues like trigger fingers), but while I know many people who’ve observed this (such as this author) to my knowledge no formal studies have been conducted on this application. For those struggling with carpal tunnel syndrome, I discussed our approaches to the disorder here.
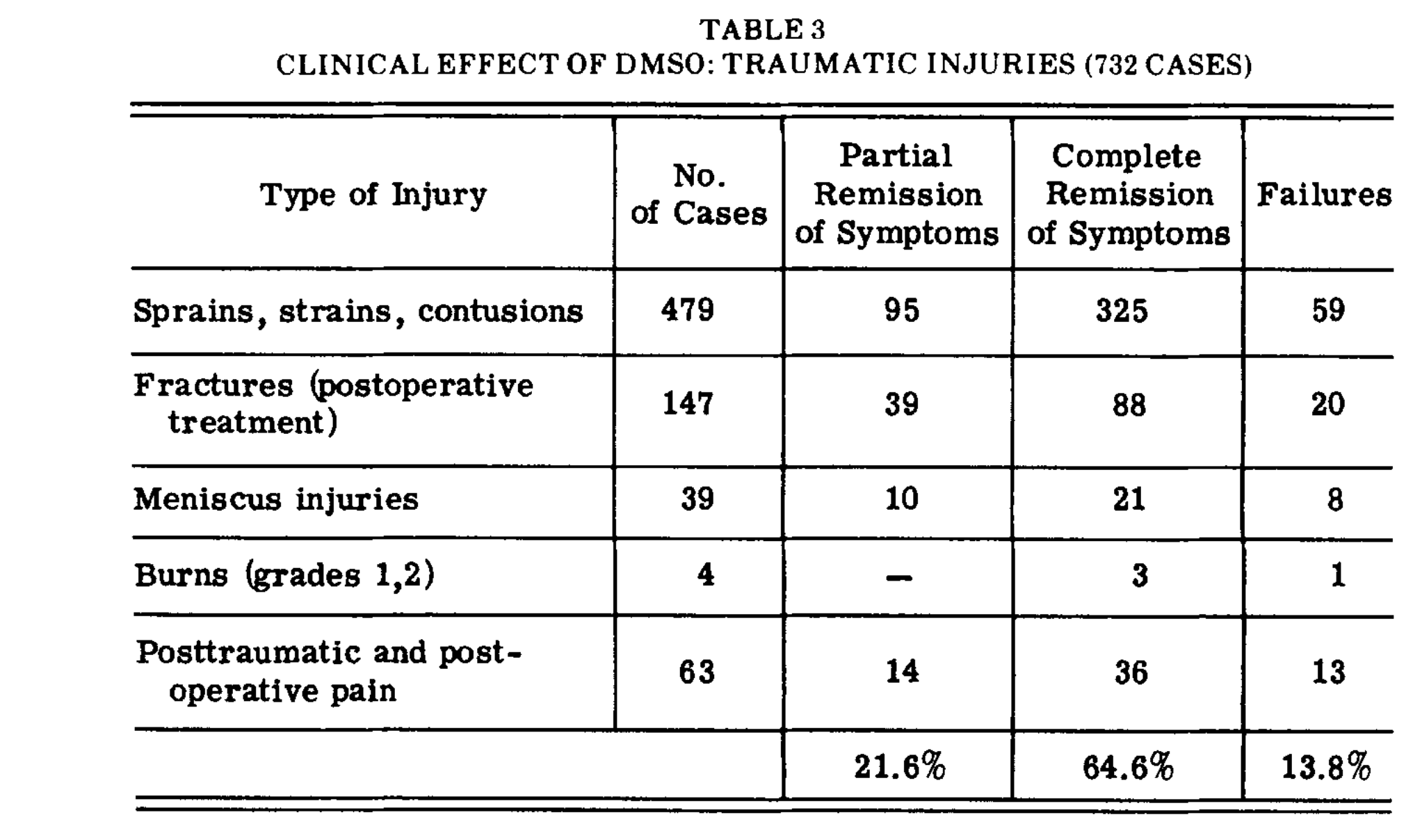
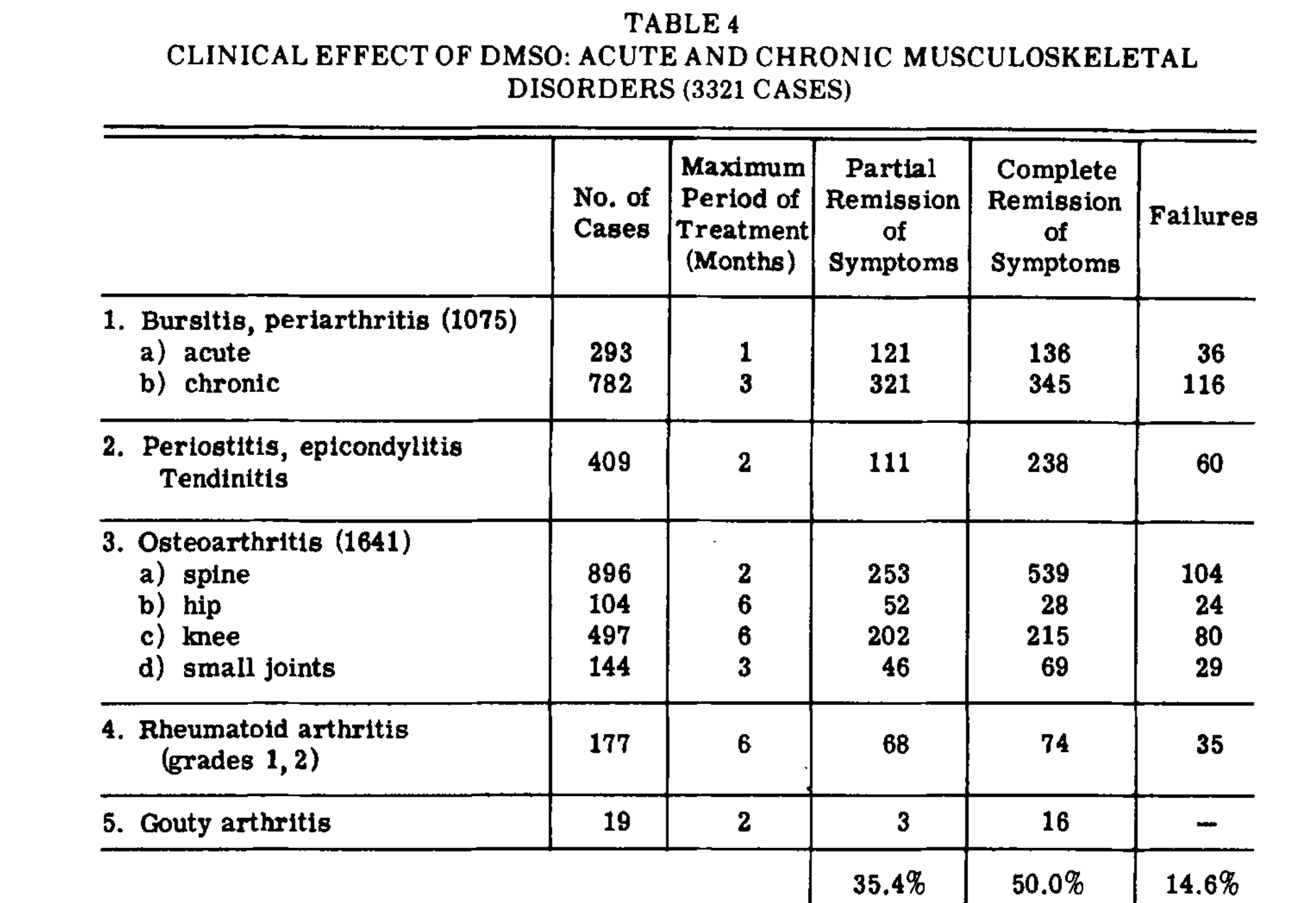
•Finally, a 1967 analysis of 76 researcher’s studies using topically applied (90%) DMSO for musculoskeletal conditions on 1900 patients found 72% improved. Specifically:
To quote the authors:
It is difficult to declare that a drug has efficacy on the basis of uncontrolled studies in a heterogeneous group of diseases. However, from these data and from discussions with many of our investigators, we feel that DMSO is a unique and effective agent for the treatment of many acute musculoskeletal disorders. Beneficial results are unpredictable, but they occur frequently and are sometimes dramatic, particularly in acute conditions, which require low doses and short treatment periods. In chronic conditions, improvement occurs at a lower rate and is less dramatic. The usual dose was only 0.1-0.2 ml/ kg/day.
Additionally:
•A 2021 study found DMSO combined with ginsenosides, particularly CK, exhibited significant therapeutic effects on rheumatoid arthritis. In cell studies, it potently inhibited the proliferation of LPS-induced RAW264.7 macrophages and TNF-α-induced HUVEC endothelial cells, while promoting their apoptosis, thus reducing inflammation and pannus formation. In collagen-induced arthritis mice, CK substantially alleviated joint swelling, redness, and functional impairment, preserved joint structure, and reduced proinflammatory cytokines TNF-α and IL-6. Additionally, CK modulated the immune response by increasing CD8+ T cells and decreasing activated CD4+ T cells and M1-macrophages, with low toxicity to major organs, positioning it as a promising candidate for RA treatment.
•In a RCT of 112 patients with osteoarthritis, 25% DMSO gel significantly reduced pain compared to placebo, reducing pain during daily activities, at rest, and under pressure.
•A 2017 study found DMSO combined with Perftoran (a tissue oxygenating agent), when injected into the joint space was found to treat bone marrow swelling of the femoral head.
Finally, at a symposium on DMSO, data on 9,521 patients were presented which showed DMSO was effective therapy in a wide variety of acute traumatic conditions, in acute and chronic subacromial bursitis, ostecarthritis, gouty arthritis, and in some patients with rheumatoid arthritis (along with other conditions such as early Dupuytren’s contracture).
Note: in addition to two of the previously mentioned studies showing the majority of patients with gout responded to DMSO, a later 1981 study also found DMSO was superior to indomethacin in the treatment of gout.
Rheumatoid Arthritis Studies
In the above results, one of the conditions which consistently improved was rheumatoid arthritis (RA). Since RA remains a common but challenging condition and a significant area of research, studies were conducted that focused on RA, all of which found significant benefit from DMSO. They are as follows:
•A 1983 study of 70 adults with RA and 35 children with juvenile arthritis:

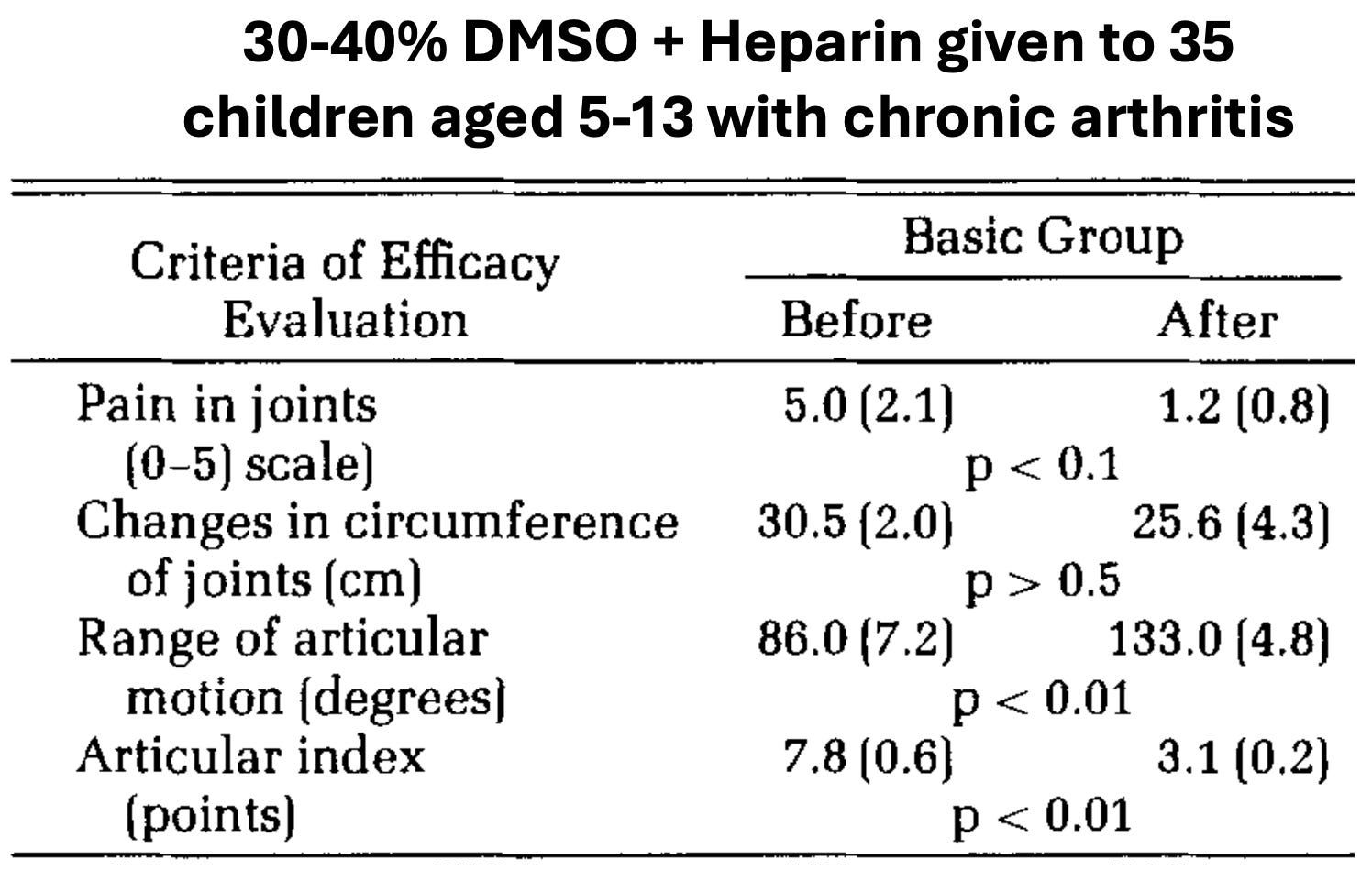
Additionally, 20 patients with flexion contractures received topical DMSO mixed with hydrocortisone, and after 5-6 applications, the range of joint motion increased by 15-20 degrees, and after 10-12, 95% had it increased by 20-30 degrees (with no relapses a month later).
•A 1965 study of 150 patients with RA treated for 10 months several times daily with 60% to 90% DMSO found diminished pain and increased range of motion were noted in 75% of milder cases and 44% of more severe cases.
•A 1967 study of 318 patients with RA who received 90% topical DMSO, 50% topical DMSO, or placebo found that DMSO had a much greater benefit that placebo. Depending on the dose, the following occurred in the 248 who were available for analysis:
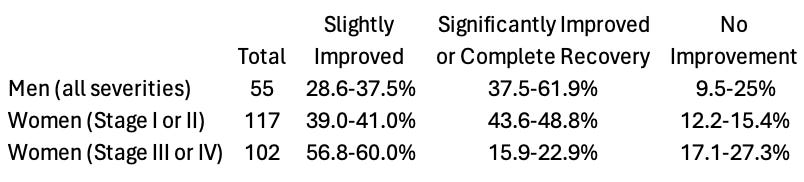
With the following specific improvements being observed:
Note: grip strength was found to have a 13.60—14.72mmHg improvement.
•A 1967 study which included 177 patients with early RA found DMSO caused a complete remission in 74, a partial remission in 68, and 35 did not respond to treatment.
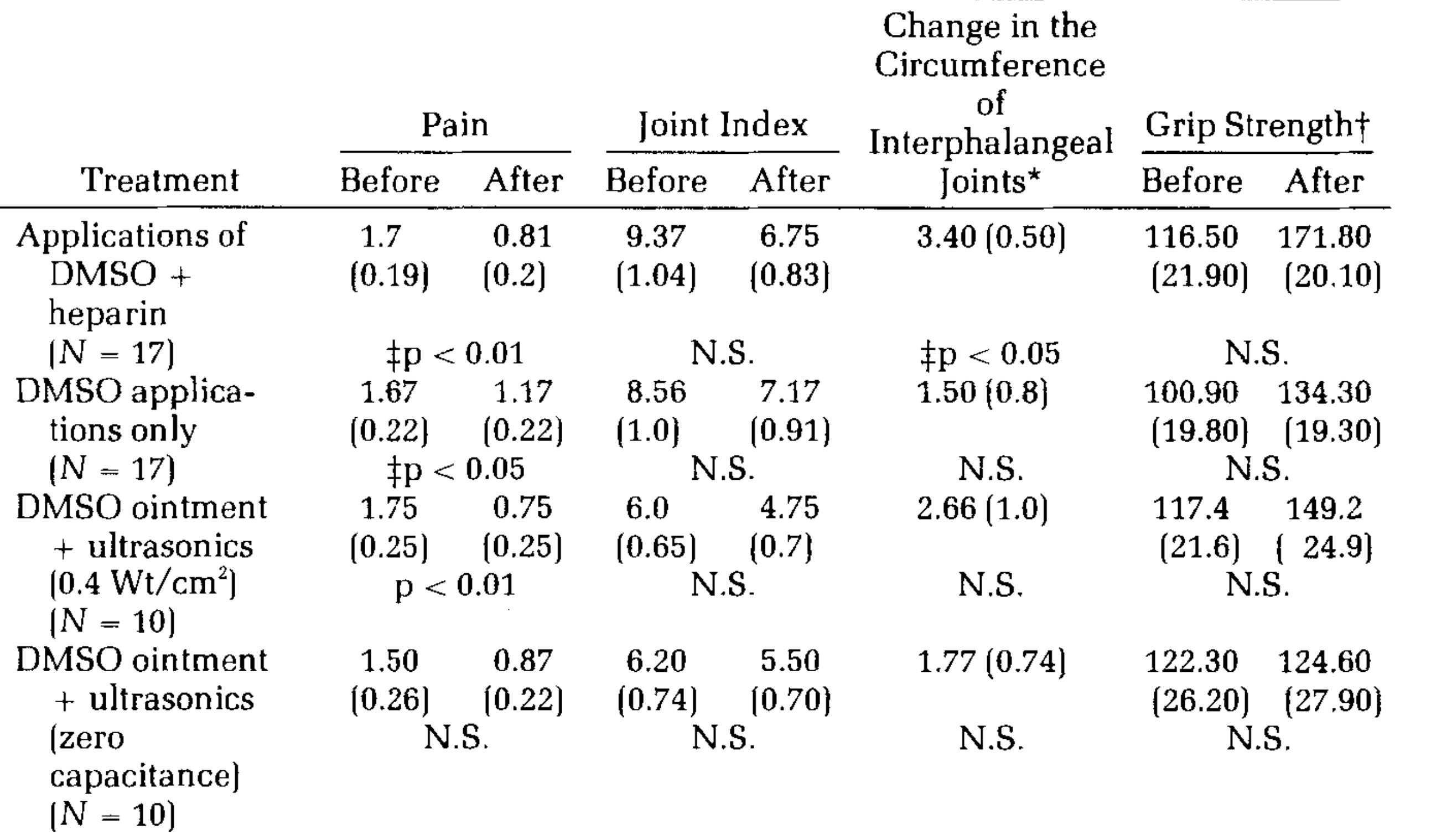
•A 1968 study gave 85% DMSO alone or in combination with hydrocortisone, procaine, or “edan” to 76 patients with rheumatic diseases, inflammation of the nerve roots or spinal disc problems (whereas controls received 1% DMSO). DMSO was observed to improve symptoms as early as an hour after treatment (with the greatest improvement happening after 3 hours) and in some cases the pain disappeared completely. In all cases, DMSO was superior to conventional therapy and was more efficacious when combined with the other therapies. Finally, within 1 week of treatment, improvement was seen in 5 out of 8 rheumatoid patients, 17 of 20 patients with inflamed nerve roots and 8 out of 10 with disc pain.
•A 1979 study treated 343 arthritic patients (320 with RA and 23 with deforming arthritis). Of them, 145 received 50-70% DMSO (applied topically to site of joint inflammation), 85 received DMSO plus analgin (a pain killer and antispasmodic), 50 received DMSO plus heparin, and 25 received DMSO plus sodium salicylate (a compound similar to aspirin), and additionally, some of the more challenging cases also received cortisone injections. In the DMSO only group, 64% had significant improvement, 19% had insignificant improvement, 15% had no benefit and 2% worsened. When DMSO was used in combination with the other therapies, it enhanced their efficacy and lowered their required dose. No issues arose from combining it with the other therapies and only 3.2% of the 343 patients had adverse effects (which were primarily skin irritation).
•A 1988 study treated 75 RA patients with a variety of therapies, and found that DMSO significantly improved a variety of parameters of the condition.
•A 1989 study injected 20% DMSO plus hydrocortisone into the knees of 25 children (aged 4-15 years) with juvenile rheumatoid arthritis and found all signs of inflammation subsided, the joint function was restored and there were no untoward reactions.
•A 2009 study found DMSO, delivered via electrophoresis, reduced joint pain and inflammation in children with juvenile rheumatoid arthritis
•A 1991 study found DMSO in conjunction with copper ions (generated by electrical currents) was a safe and effective treatment for RA.
Note: another Russian study found that DMSO combined with Dopan (a form of dopamine) was an effective RA treatment (which has some basis as dopamine agonists have shown promise for treating RA).
•This book discussed a Brazilian study (I could not locate) where 15 RA patients and 15 OA patients received an IVs of DMSO (5ml), a B-complex, vitamin C and magnesium sulfate 2 times a week for 5 weeks and then once a month for 18 months. This caused an immediate 66% decrease in free radical production (and a longterm 52% reduction), and created a lasting clinical improvement in over 85% of the patients with OA and 77% of the patients with rheumatoid arthritis.
Note: DMSO has also been used in combination with decimeter-wave and mud therapy to treat OA.
•Finally, 1998 and 2000 cow studies found that if aseptic arthritis was induced in a joint (by injecting turpentine oil) and then treated each day with DMSO, if on days 2 and 7, the joint was injected with healthy sinovial fluid from the same cow, recovery was enhanced.
To put this into context, consider the story of Patricia McClenathan, a 39-year old New Yorker who had been receiving treatment for the last six years from rheumatologists for spondylitis (inflammation of the spinal joints) that left her with deep pain, a loss of mobility, and a variety of severe side effects from the drugs and procedures she had received that could only reduce her pain. As time went on, her condition continued to worsen (e.g., her discs ruptured) she become bed bound and fell into a deep depression. A relative then suggested DMSO (as DMSO had recently been legalized in Florida) and having no other options, she flew to Florida for daily IV DMSO sessions, and by the third day experienced a profound improvement (and a complete improvement on day 5).
Since taking DMSO, I am now a functioning person where previously I had not been, spending much of the time in bed accomplishing nothing. I can do most normal things now by relying on DMSO. At this time [January 7, 1981], I take no painkillers or muscle relaxants [both used quite heavily before] and find for this reason I can cope with everything very well. I am finally physically, mentally, and emotionally much better and attribute this to DMSO. I feel that the problems the DMSO has caused are by far outweighed by the new life it has given me—a life other than just surviving in constant pain. Again, I thank you.
Likewise, consider Ruth Lewis:
When I entered the doctor's office for DMSO treatment, I was unable to put both feet on the ground. After two-and-a-half weeks of IV DMSO treatment I walked out of that office without any help whatsoever—no cane—no support at all. I had not been able to close my right hand completely for over a year. It even kept me awake at night with severe pain. But after the IV, topical, and oral DMSO treatment, I can now close my hand tightly. The arthritis has not returned.
I cannot put into words what this drug has done for me. I highly recommend it. I saw many people come and go during my clinic stay; all walked out well.
Or this testimony sent to the Congressional Committee from a woman who shocked her Orthopedist after DMSO regenerated a “rotted” femur (which had previously caused the orthopedist to believe there was nothing that could be done for her as it made a hip replacement surgery impossible):
I was one of the people who was suffering needlessly and spending large sums of money on useless medical treatment when I was introduced to DMSO 16 years ago. I had severe bursitis in my right shoulder, painful arthritis in my right knee from an old injury, and a degenerative left hip joint. Sleep and rest were something I had not known for many weeks when a friend who had been an arthritic invalid, gave me about 2 tablespoons of DMSO. I applied this to my shoulder twice one evening and fell into a 12 hour restful sleep. I awakened cured!
Countless stories like this exist (which, due to length considerations I did not list), and in many cases encapsulate the “excellent” responses to DMSO many of the previous researchers listed (and discussed in their articles). That in short is why there was so much public and professional pushback against the FDA’s prohibition of DMSO.
I can actually swear and take an oath that relieved all my pains through my legs and has helped me maintain my job. am a waitress and all my work depends on my feet feeling good. This drug should be available. I can’t understand why people have to suffer, when we all can live and work a normal life with this drug available. It's not fair for parts of Europe and Greece, etc., to have it only. The average person can’t take the time or expense to travel where its legal to get DMSO. Please help get the FDA to legalize it.
Lastly, many patients find taking DMSO allows them to significantly lower the doses of their existing arthritis medicines (which is often quite helpful as their toxicity worsens with increasing doses).
Note: many patients with arthritis also experience positive results from MSM (DMSO’s primary breakdown product in the body) or soaking in sulfur containing hot springs.
Sports Injuries
What I like about DMSO is that you don’t have to interrupt your training every time you get a minor pull or sprain. It doesn’t pump you up like certain pills. It’s simply a very useful thing to use for simple athletic injuries. Some people have told me that you shouldn't use it because it might mask the pain of a serious injury, but a good athlete knows his body well. Even when I’m using DMSO, I know when I can push and when I can’t. —Al Oerter, a discus thrower and the first American to win 4 consecutive Olympic gold medals.
One of the greatest challenges professional athletes face are sports injuries which prevent them from returning to the field, particularly since many sports injuries are a product of micro-injuries building up until a critical point is passed (e.g., from adhesions and scars in the soft tissue). In turn, since DMSO both heals micro-injuries and rapidly treats traumatic injury (returning them to full functionality), DMSO was rapidly adopted by professional athletes once they realized what it could do for their careers (and being off the field was often devastating to their careers). In turn, due to the voice their position afforded them, a few professional athletes (e.g., Atlanta Falcons Quarterback June Jones—who now is a coach) became some of the most impactful advocates for DMSO (e.g., Jones stated in Congressional testimony that “veterinary” DMSO was widely used but athletes were afraid of publicly discussing it).
Likewise, in 2013, a Dallas Cowboys Lineman stated:
You get it [from] the veterinarian and it goes right to the bloodstream. It’s an ointment that’s like anti-inflammatory. You put it on your skin and you put it on a muscle, and I guarantee you, in about 30 minutes you’d feel it. It wasn’t on the list [of banned substances]…we used DMSO and people knew it. Everyone knew about it.
Furthermore, in his riveting testimony, Jones provided cases that left the Congressmen in disbelief, such as a teammate with a bone chip and a torn ligament (which would require months of recovery and hence end their season) taking DMSO immediately after the injury and 7 or 8 days later returning to the field (with the bone chip remaining but no longer causing issues).
Likewise, at that Congressional hearing, the former team physician for the Oakland Raiders testified that he’d used 70% topical DMSO on a careful and controlled basis for his players 20-30 times a year for 5 years. From this, he observed that DMSO was the most beneficial when given in the first 3 to 4 days of an acute injury where a muscle or joint had severe swelling, particularly of the extremities, especially the ankle, elbow, hands, or wrist. Overall, he stated that DMSO provided good to excellent results 70-80% of the time (e.g., through reduced pain and swelling) and the players felt they were able to return to play 50-75% faster than they had from similar injuries in the past. Conversely, they did not find DMSO was helpful for chronic injuries, but this may have been due to it not being used long enough for the effects to kick in.
Note: he also emphasized that DMSO would transform the field of occupational medicine. I fully agree with his assessment, especially given just how frequently Worker’s Comp fails to help its patients.
Similarly, podiatrist Lowell Scott Weil (who was the physician for both the Chicago Bears and the United States Olympic gymnastics team) uses DMSO on a regular basis (particularly injured gymnasts). After 12 years of using it, he shared, he’d seen it rapidly heal injuries (e.g., he had a gymnast who suffered an ankle sprain expected to end her season, but instead her rapid recovery allowed her to make the US Olympic team, and a Football player who tore his hamstring but was able to rapidly return to the field). Overall, he had a 60% treatment success rate and saw the best response to DMSO for tendinitis, myositis, and post-injury situations such as muscle pulls, ankle sprains, strains, and tears of the soft tissue (and conversely the only side effects he had were skin irritation). Additionally, he also used it for arthritic patients (especially rheumatoid arthritis) with many having dramatic relief.
Many other compelling anecdotes exist. For example, this book discusses the experience of an Oregon State track coach and early adopter of DMSO who had many amazing stories of DMSO treating hamstring and achilles tendon injuries such as an athlete being able to return to the field at full capacity 3 days after a normally disqualifying hamstring injury and the story of a blind long distance runner who was able to run due to DMSO fixing musculoskeletal injuries and (according to the author) then played a pivotal role in opening the sport to women.
Note: a major problem in certain sports like football is repeated concussions (which are now recognized to put them at risk for cognitive impairment and dementia later in life). As discussed in the first part of this series, DMSO is immensely helpful for mitigating the effects of concussions.
In addition to these anecdotes and studies of DMSO’s utility in other musculoskeletal injuries, research also directly corroborates its value in sports medicine.
•A 1965 study treated 47 injured athletes from a wide range of sports (e.g., tennis, diving, or wrestling) by applying 90% DMSO applied to the injured areas 3 times a day initially and then after 2 days, twice a day. The group was comprised of 30 acute injuries (e.g., sprains, strains, dislocations, serious cuts) 7 syndromes that follow long immobilization for broken bones, and 10 chronic conditions (e.g., tennis elbow) resulting from repetitive "microtraumas." The acute traumas were observed to rapidly resolve, sometimes "so spectacularly as to compel us to urge our patients to observe greatest caution in order to avoid further damage to a joint," while the chronic conditions and syndromes also responded rapidly and those athletes were often able to quickly return to the field. These results and the lack of observed adverse events led the investigators to argue DMSO urgently needed to become the standard of care in sports medicine.
•A 1967 paper discussed 8 players of the Buffalo Bills Football Team who were treated with DMSO for injuries during the 1964 season and in each case, the player returned to full duty 50% sooner than he would with other forms of therapy. These injuries included severe muscular contraction of the adduction thigh muscles, acutely strained sternomastoid muscle, acute sprain of sternoclavicular joint and another with acute sprain of medial collateral ligaments of the knee.
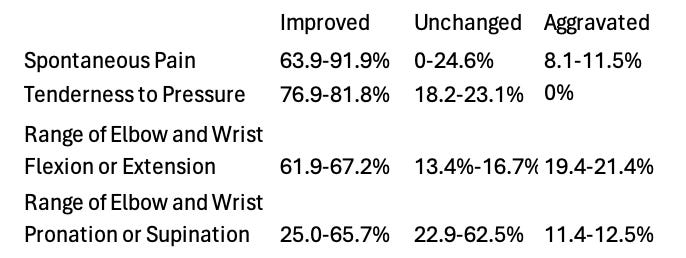
•A study of 78 patients (mostly athletes) with overstrained tendons received Dolobene gel (15% DMSO, dexpanthenol and heparin) for 2-3 weeks, with over 50% having a significant improvement of symptoms and those improvements including a 94% improvement in pain, a 55% improvement of swelling, 95% improvement of redness and 92% improvement of warmth.
•A study gave Dolobene gel to 30 athletes with soft tissue injuries of the upper and lower extremities twice daily for 4 weeks. There were 4 athletes with contusion of the shoulder, 8 with distortion and contusion of the knee joint, 8 with muscle, tendon and ligament lesions, and 10 with distortion of the ankle joint. Following DMSO, 10 had an excellent response (improvement), 5 had a excellent to good response, 10 had a good response and 5 had a moderate response. Specifically, pain, inflammation, swelling, reabsorption of hematomas, tenderness and recovery time were assessed.
•A study gave Dolobene gel and ultrasound to 15 subjects who had received a blunt tissue trauma (without fracture) to the lower extremity within the last 24 hours. Compared to 15 placebos, the treatment resulted in a faster relief of pain, reduction of edema, and recovery of mobility.
•A 1966 study of 28 professional baseball players found that giving them DMSO after injuries caused their downtime be one third of what was observed by the treating physician in the previous year with 42 players.
Note: While not quite the same as getting tackled, I’ve also come across cases of individuals taking DMSO immediately after getting hit by a car while crossing the street (which caused injuries but no fractures) and immediately fully recovering.
Additionally, a veterinary practice using 90% DMSO reported that in 10 dogs with ruptures of the ACL (anterior cruciate ligament), after surgical repair, DMSO halved their recovery time with edema disappearing promptly and much less analgesia or sedation being required. Additionally, they cited the cases of:
•A large German shepherd that was run over by a truck (sustaining multiple fractures of the femur and tibia, with extensive tissue bruising), where DMSO facilitated a rapid post surgical recovery.
•Two cases where the swelling and sensitivity around prosthetic implants was markedly reduced by DMSO.
•A racing greyhound who sustained severe tendinitis above the tarsal joint (an injury where they are rarely are able to retain their former speed) who received DMSO after 60 days of non-recovery, rapidly improved, and after a few months won two races and before long established two new track records.
Horse Studies
As DMSO is widely used in veterinary medicine, a wealth of research shows it treats musculoskeletal conditions (and likewise it is approved to treat those conditions). As there are too many too list, in the spirit of the FDA’s war against ivermectin, I wanted to share a few horse ones:
In horses, after over 50 cases of bursitis or synovitis were treated with DMSO, in almost 90% of cases, there was at least “some improvement” and often a “complete return to normal,” in 65 cases of osteoarthritis and periostitis, 60% had a clinical improvement, in 20 cases of metacarpal periostitis (“bucked shin’’), 90% had a “quick relief,” and in 22 cases of tendinitis (bowed tendon), there was a therapeutic response superior to any existing therapy.
Likewise, another team of researchers found 90% of horses with bursitis or synovitis (totaling 50 horses) improved from DMSO (with many fully recovering), out of 65 horses with osteoarthritis and periostitis (involving the carpus and the fetlock joints), 60% improved with DMSO (many of whom had not responded to other treatments for months), including quick relief 90% of those with bucked shin (an otherwise challenging condition) that was sustained if followed by a period of rest. Additionally, 22 cases of tendonitis (bowed tendon) improved with DMSO, and 14 traumatic injuries (involving subcutaneous edema and hemorrhage) had a remarkable response to treatment.
Thirteen horses had two of their tibiotarsal joints injected with LPS to induce inflammation in them and DMSO (unlike the other interventions tried) was found to reduce the inflammation in their joints.
Other Datasets
The following datasets also deserve mention:
1. On September 8, Merck Sharp & Dohme Laboratories sent out to all investigators under their auspices an advisory memorandum on the emerging role of DMSO in experimental medicine. It stated based on their data from 4000 patients (who had taken DMSO for up to a month) that DMSO was safe and had shown merit for many of ailments including many of the conditions discussed here. For those conditions listed here, it stated:
•Acute Inflammatory or Traumatic Situations—Some pain relief usually occurs within one hour. At 2 hours the pain is usually reduced by at least 50%. Continue for 3 to 7 days to assure that the condition does not recur.
•Chronic Conditions—Response has usually been slower and the pain relief from a single or a few applications may be transient. A significant response may not be obtained until after 4 to 12 weeks of daily administration.
•Acute bursitis—Merck’s largest clinical trials were for this and in the majority of patients, decreased pain and increased range of motion was observed in about 30 to 60 minutes, lasts for lasts 2 to 6 hours, and typically is less severe once in returns.
•Acute low back strains—In the majority of patients decreased pain and increased range of motion has been observed in 30-60 minutes and in some cases a spectacular improvement in pain in observed.
•Acute injuries (e.g., strains, sprains, contusions, athletic injuries, industrial injuries and other traumatic situations)—These typically responded quite dramatically to DMSO. However, since DMSO has masked a few fractures, x-ray diagnosis was advised in most cases.
•Acute neck strains (whiplash)—Wide area of application has given good results.
•Osteoarthritis—DMSO applied to osteoarthritis of the knees has produced a favorable response after 4 to 6 weeks of daily administration. Transient relief may occur before this time. Increased mobility and general ability to walk and perform tasks without pain has been remarkable in some cases.
•Rheumatoid arthritis—DMSO seems less effective here than in certain other diseases. Grades 3 and 4 responded only partially after prolonged administration.
•Neuralgias and pain syndromes—A wide variety of pain syndromes have responded to DMSO. In tic douloureux or trigeminal neuralgia, some but not all patients have obtained benefit. Treatment must be long-term. The pain relief may not be permanent. Herpes Zoster has responded most favorably.
•Gout—There have been a few cases of dramatic relief of pain and general improvement.
•Surgery—After thoracotomies, cholecystectomies and hemorrhoidectomies, 5 to 15 cc. dose 3-4 times/day, results have been very good.
2. Podiatrist Morton Walker was selected as a clinical investigator for Merck and using an innovative technique to drive topically applied DMSO into the target treatment area (which to my knowledge no one else has utilized) and found DMSO:
•Was highly effective for acute bunions (and the bursitis they caused) but not effective for the chronic bunions which followed the acute stage.
•Temporarily (typically few a few days) eliminated the pain from hammertoes, ingrown toenails, hard corns and soft corns.
•Eliminated the pain while followed the removal of many foot skin conditions (e.g., after a shaving).
•Is very helpful in the management of overgrown (club) toenails. For example, applying DMSO mixed with olive oil or castor oil makes it much easier to remove them and prevent them from regrowing.
Note: DMSO when combined in low doses with 5-fluorouracil has been found to be highly effective for treating psoriatic nails (onychodystrophy), which otherwise is a challenging condition to treat.
•Was excellent for arithritis of the foot and ankle, particularly the toes.
•Is often very helpful for Morton’s neuromas, dancer’s foot (sesamoiditis) and heel spurs.
•Could help in the treatment of flat feet (by removing inflammation and helping to heal damaged ligaments and muscles).
•When combined with an antifungal agent (which DMSO brings into the skin) is very helpful for fungal infections of the feet and toe nails.
Note: research has subsequently confirmed Walker's discovery. However it is important to remember that nails are one of the only tissues DMSO cannot effectively penetrate so DMSO must also be applied to the surrounding skin.
•Is very helpful for sprain ankles.
Note: this is one of the most common things DMSO is used for (as it works). Because of how rapidly it removes pain and inflammation, many worry the individual no longer guarding the ankle will predispose it to further injury (and hence strongly urge the patient to remain cautious with how they walk after the treatment), but in real life, a re-injury occurring is not reported to be an issue.
•Soaking in 50% DMSO effectively eliminates foot odor—however this is not always helpful since taking DMSO can cause its characteristic side effect (a garlicy odor).
Sadly however, after Morton Walker had tested DMSO on 124 people with excellent results, the FDA banned all research into DMSO and Merck immediately confiscated his records (which were subsequently never published).
Note: another author reported he finds 60-75% DMSO is very helpful for blisters and calluses, as it both softens the skin and dries the blisters out and 75% topical DMSO will gradually shrink Baker’s cysts (which form in the knees).
3. Clinical studies done for Syntex Laboratories in the early 1960s by Dr. Arthur Steinberg showed that chronic arthritis patients given topical DMSO applications four times daily experienced pain relief in about 84 percent of cases, and also demonstrated increased mobility and decreased swelling in the inflamed joint. Steinberg found that when DMSO therapy was discontinued, the swelling returned. His study also showed that rheumatoid arthritis patients experienced subjective pain relief from DMSO about 77 percent of the time, and, like Drs. John and Laudahn, he reported that several patients got relief from a combination of DMSO with a reduced dosage of their normal medication.
4. Since the FDA had essentially ended DMSO research in the country with their 1965 ban, the 1980 House Select Committee decide to conduct more “research” by sending a survey to 250 randomly selected American Veterinarian, another 250 Rheumatologists and 110 physicians of professional athletic teams.
Of the 134 veterinarians who responded (54% of those surveyed), 94 (70%) said they had used DMSO in practice and of them 85 (90%) believed it to be effective in reducing inflammation, pain or other arthritic symptoms in animals while 75 (80%) believed from their experience in animals that DMSO would be safe and effective for humans.
Some of the main uses for which the veterinarians used DMSO were: tendonitis, lameness, bruises, arthritic joints, acute inflammation and swelling, chronic inflammation in ear canal, edema, sprains, strains, mastitus, laminitus, splints and other leg injuries in horses, cattle and dogs, intravenously for head injuries in dogs, to relieve spinal pressure due to ruptured interverbral discs and as a carrier for other medications.
Note:
Of the rheumatologists, 169 (68%) responded and of them, the majority felt more carefully controlled studies of DMSO were warranted, 33 (20%) had used or prescribed DMSO in their practice and of those 33, 49% felt the drug was effective in reducing inflammation, pain or other arthritic symptoms (along with another 23 who felt the same but had no direct experience with the drug) and 12 (36%) felt the drug should be legalized.
Those who had used DMSO in their practices reported using it for the following conditions: arthritis (including osteoarthritis, rheumatoid arthritis and degenerative arthritis of the spine), bursitis, scleroderma, tendonitis, fibrositis, gout, sprains, skin ulcers, painful muscles, cervical syndrome and epicondylitis.
Of the 39 team physicians who responded, 7 had used DMSO (for conditions such as inflammation of joints, sprains, swelling, tendonitis, bursitis, muscle bruises and contusions, and gout), and 5 more (who did not use DMSO themselves) had seen it used in sports medicine. Of those 12, 10 found DMSO effective in reducing inflammation, pain or other arthritic symptoms. Additionally, most of the 39 believed further study on DMSO was warranted.
While I can’t list all of the correspondences they received, I did want to quote this one:
DEAR CONGRESSMAN PEPPER: I have had considerable clinical experience with DMSO utilized as an external liniment to various painful joints and other areas of the body. In the past, I have treated over two hundred patients with DMSO products made by Syntex Laboratories.
Most of these patients were benefitted. None of the patients experienced any serious injury to their health. One man did break out with a rash and some pus which resembled impetigo, but this cleared promptly when the liniment was stopped.
I would strongly recommend that this drug be made available to the medical profession, at least in liniment form, because of its effectiveness in relieving muscular and joint pains.
Sincerely yours,
ALBERT A. Wilson, M.D., P.A.
Note: my essential goal with this series (and why I’ve put so much time into it) has been to provide a public record everyone else can use as a reference to advance the use of DMSO (much in the same way I’ve done with other critical forgotten sides of medicine like ultraviolet blood irradiation). In turn, while I’ve done my best to compile the pertinent data, it’s certain I missed quite a bit of it, so if you know of any (especially if you have copies of the actual studies I only provided citations for), please send them my way so I can incorporate them into this.
Dosing and Topically Applying DMSO
My hope is that this article and the previous one make a strong case for how miraculous DMSO is and how egregious it is that the FDA kept it from America for decades, and why I felt it was so important to bring awareness to this subject.
In the final part of this article, I will discuss the established protocols for applying topical DMSO for many of the conditions here (including our preferred methods), key precautions to be aware of, tricks we’ve found for using it, and our preferred sources for obtaining it.
