Unmasking The Great Ozempic Scam
The GLP-1 saga epitomizes the unsustainable corruption within our medical system

Story at a Glance:
•In early 2023, a private conference with pharmaceutical industry leaders and investors highlighted anti-obesity and Alzheimer’s drugs as the next big money-makers and had the FDA head as its keynote speaker.
•Since then, the FDA has taken questionable steps to promote these drugs, particularly Ozempic, an anti-obesity medication. There's been a massive push to get everyone, including children, on Ozempic, using shockingly aggressive marketing tactics.
•This rush is eerily similar to the fen-phen craze, a temporary weight loss drug later pulled from the market for causing severe heart and lung issues.
•Worse, Ozempic comes with serious side effects, including paralyzing the digestive tract. This article will address the above controversy and explore the common causes of obesity, including those rarely discussed.
Most of the food in America comes from just a few crops like corn, wheat, soy, and canola, largely due to farming subsidies that force farmers to mass-produce these crops and sell them below cost. These cheap crops are then turned into the processed foods we eat every day. This is problematic because:
Health Issues—These foods are unhealthy and contribute to major health problems like diabetes and obesity.
Natural Aversion—Our bodies naturally resist these foods, making them hard to sell.
Addictive Additives—To make them more appealing, addictive substances are added. In the 1980s, Big Tobacco bought the processed food industry and, much like they did with cigarettes, focused on making these foods as addictive as possible.
Chronic Illness—The resulting health issues create lifelong customers for industries like Big Pharma.
For years, health activists have pushed for awareness of the importance of natural foods and the need to change farming subsidies to promote healthy eating. The current media climate, driven by skepticism of the COVID-19 response and the rise of independent media, has revealed the systematic failures in our food supply and allowed these long-cultivated ideas to begin bursting into public awareness.
Because of this, MAHA has begun receiving mainstream attention to alert the public to many longstanding concerns we’ve had about processed foods (e.g., seed oils and artificial dyes) that previously were ignored, ridiculed and dismissed. Consider, for example, this remarkable segment Fox aired last year slightly before the 2024 election:
Pharmaceutical Sales
Every now and then, we get a clue about what goes on behind the scenes in the pharmaceutical industry (e.g., see this article and this article about the sociopathic sales-focused culture within Pfizer). One particularly telling instance was a presentation GSK gave their sales reps for Advair, which I believe is representative of the mentality of this industry:
In 2023, Kim Witczak, a pharmaceutical safety advocate, tipped me off about JP Morgan’s annual healthcare conference, a private invitation-only event described by JP Morgan as “the industry’s biggest gathering.” The 41st conference, from January 9-12, 2023, was the first event hosted in person since the pandemic started. Given this event's immense influence on the pharmaceutical sector (as it caters to large investors), it’s important to highlight a few things that were presented on the conference website:
First, consider how enthusiastically they endorsed the profitability of two new types of drugs:
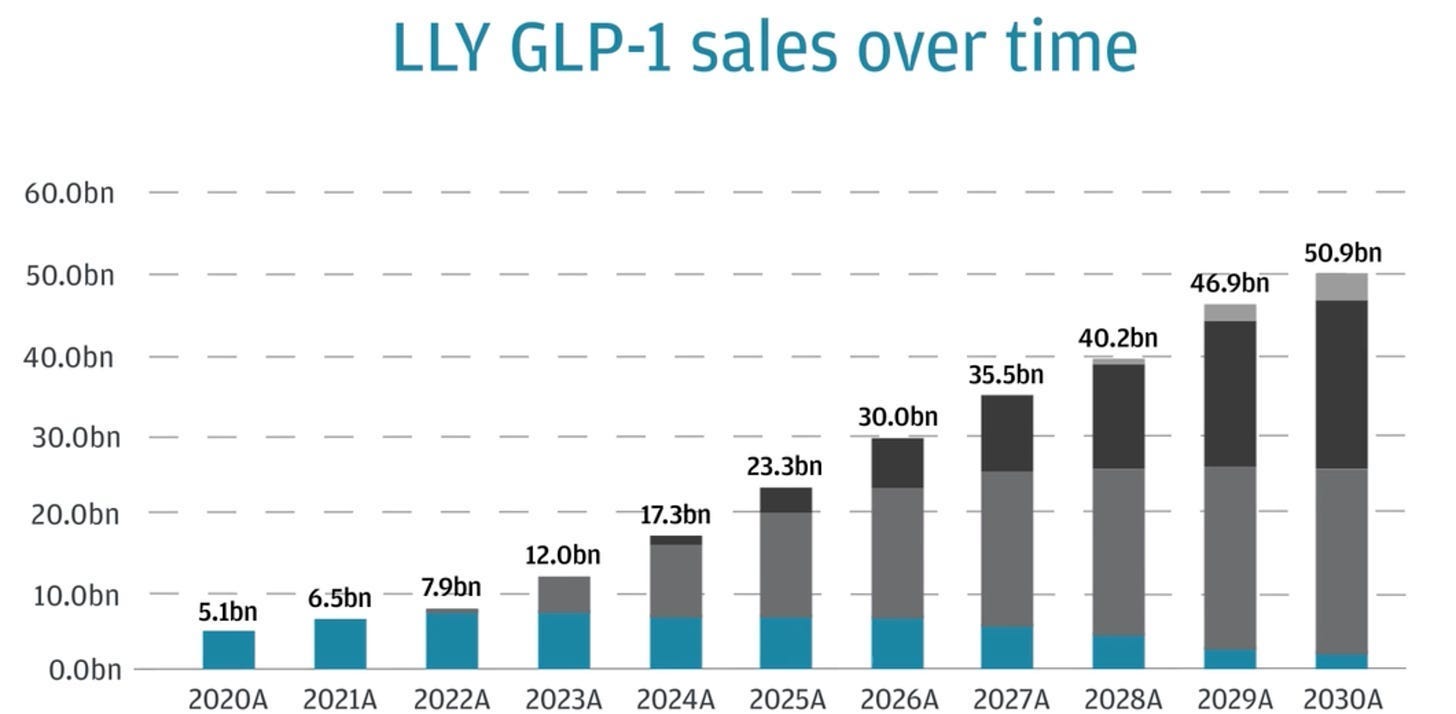
In that video, the most important part was Chase’s projections for this new industry:
Second, consider who the keynote speakers at Chase’s conference were:
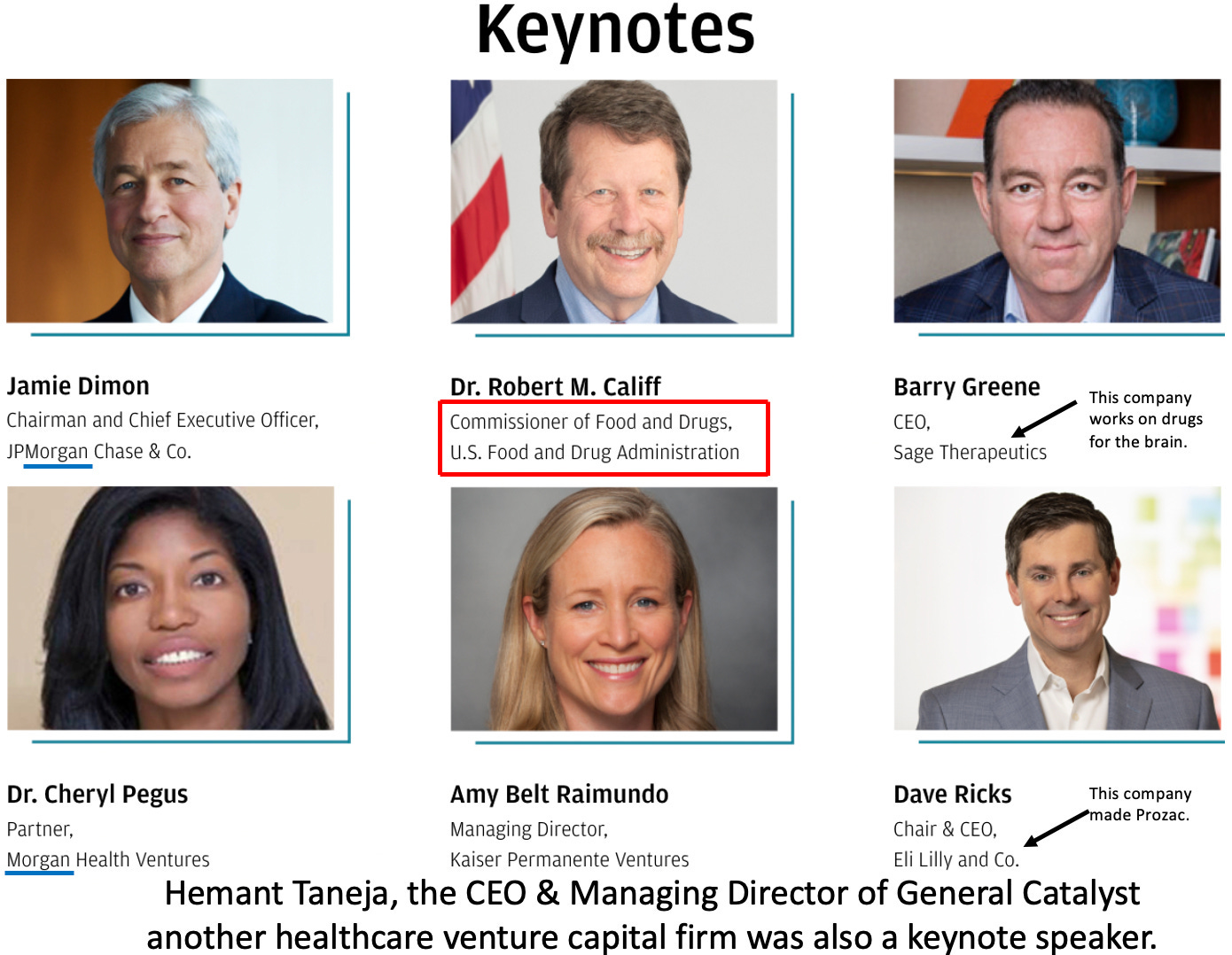
Note: after I originally publicized this conference, parts of it were deleted (e.g., one of the above videos and Califf being listed as the keynote speaker). Califf has long been an incredibly controversial FDA commissioner due to his immense pharmaceutical conflicts of interest.
To repeat—the head of the FDA was a keynote speaker to investors about the incredibly lucrative opportunity they could expect from these new drugs—implying that the FDA would do everything it could to push them through. As it so happened, to quote Witczak:
Interesting to also note, Califf was the keynote speaker on opening day and out of the blue, the FDA granted accelerated approval to the second controversial Biogen Alzheimer drug on Friday [three days before the conference] without an Advisory Committee. How great to be able to announce to the healthcare biotech industry that one of their new drugs was just granted accelerated approval.
Note: an even more controversial approval had proceeded it (where the FDA overrode its own panel to approve an expensive, dangerous, and ineffective Alzheimer’s drug which resulted in three of the experts on the panel resigning, with one stating it was “probably the worst drug approval decision in recent US history”). Shortly afterward, Califf’s FDA gave a glowing press release on their approval of the drug—but due to how unsafe and ineffective the drug was, even with the FDA’s endorsement, rather than become the next blockbuster drug, it abjectly failed in the market and is now being discontinued by the manufacturer. For those interested, I discussed the immense scandal with existing Alzheimer’s drugs and the suppression of proven (but un-patentable) treatments for the disease here.
Lastly, when Jimmy Dore discussed this article on his show, Calley Means shared that people who attended the Chase conference told him that when the profitability of the GLP-1 drugs was announced (e.g., 1600.00 per month per patient from the government), they were “clapping like seals” and that there was a “standing ovation when they talked about the obesity crisis and this drug.” I would argue this illustrates why allocating more money to a problem often is counterproductive to fixing it.
The Rise of Ozempic (semaglutide)
Once I saw this conference, given that it sets the course for the entire pharmaceutical industry, I was almost certain that Ozempic would soon be aggressively marketed, with the FDA backing the expansion of its use. This prediction quickly became a reality, with widespread promotion and endorsements of the drug, reminiscent of the start of the opioid crisis. Here for instance, are excerpts of two widely seen interviews by Casey and Calley Means describing the staggering corruption that has facilitated Ozempic’s rapid rise throughout America:
Sadly, the campaign has been so successful we’ve now seen shortages of Ozempic, driving people to seek alternatives.
The push to expand Ozempic's market has targeted various demographics, including:
African Americans: Ozempic’s manufacturer paid the NAACP to lobby for the drug, framing any opposition as perpetuating systemic racism.
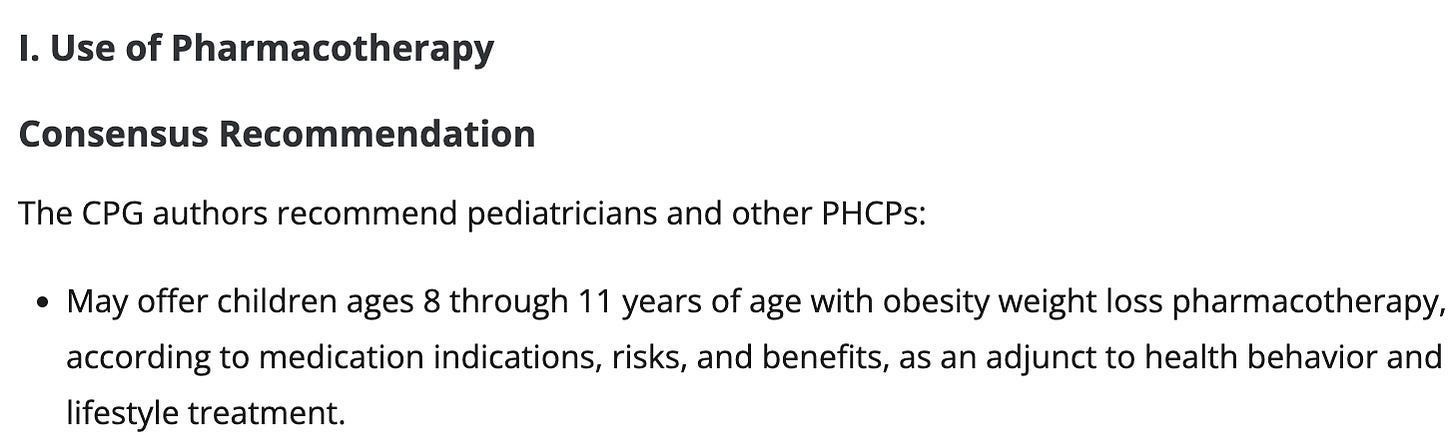
Children: The FDA approved semaglutide for obese children 12 and older just before the Chase conference despite concerns about long-term effects, and on the first day of the Chase conference, the American Academy of Pediatrics published authoritative guidelines for treating childhood obesity which strongly endorsed giving them the GLP-1’s:
The Elderly: One major obstacle to selling Ozempic is its high cost ($1,000-$1,500 per month), making it unaffordable without insurance. The Medicare Modernization Act of 2003 prohibits Medicare from covering weight loss drugs, but the industry has been lobbying to overturn this. Senator Cassidy, on behalf of an "obesity rights" coalition, (funded by Ozempic’s manufacturer), in turn, is attempting to advance a law through committee to allow Medicare Ozempic coverage, which could cost between $3.1 to $6 billion annually if passed.
This raises a critical question: Why was Medicare originally prohibited from covering obesity treatments?
The Rise and Fall of Fen-Phen
A recurring theme I've explored is how medical catastrophes often repeat because we forget the lessons from the past. The current rush for Ozempic is strikingly similar to the fen-phen disaster of the 1990s. Phentermine (introduced to the USA in 1959) and fenfluramine (introduced to the USA in 1973) were two marginally effective weight loss drugs that never caught on.
In 1979, a professor of clinical pharmacology and director of an FDA division for approving new drugs believed obesity needed to be treated as a medical (rather than lifestyle) disease and decided to see if they’d work better once combined. Fen-phen “worked,” and when his study was finally published 20 years later, it instantly became wildly popular.
As word spread, demand surged, turning many doctors' offices into pill mills catering to desperate patients. However, it wasn’t long before the drug was linked to severe heart valve damage and pulmonary hypertension, leading to its removal from the market and billions of dollars in legal settlements. Remarkably, once the dust had settled, the FDA official who pushed Fen-Phen onto the market admitted it never occurred to him to verify the drug combination was indeed safe.
What’s particularly alarming is that many of the issues we see today with Ozempic—aggressive marketing, off-label uses, and a focus on profit over patient safety—mirror the mistakes made with fen-phen. Back then, the FDA eventually stepped in to ban the drug after realizing the extent of the harm it caused, but this time around, the FDA instead is working with the industry to push these drugs.
The Risks and Benefits of Ozempic
Prior to the GLP-1s being marketed as anti-obesity drugs, many of my colleagues believed they were quite helpful for diabetes. Given that some of these colleagues were fairly conservative with which drugs they would use and excellent clinicians, I took their opinions into serious consideration. However, I also noticed that I was repeatedly seeing patients develop unusual gastrointestinal complications from the drugs (including one hospitalization of a distant relative), so I held to the perspective the drugs were too new for their risks to be fully appreciated.
After they started being used as weight loss agents (where their dose is much higher—0.5-1.0mg vs. 1.7-2.4mg—frequently being almost five times greater), we started noticing that we’d see more and more patients who should have never been prescribed the drug and are taking enough of it (often even overdosing) to drive themselves into cachexia. These patients are easy to identify as they don’t look normal and have a somewhat sick and somewhat anorexic appearance since they are starving themselves. This is best demonstrated by what has come to be known as the “Ozempic Face”

Note: many healthcare professionals are now noticing an epidemic of Ozempic facilitated eating disorders.
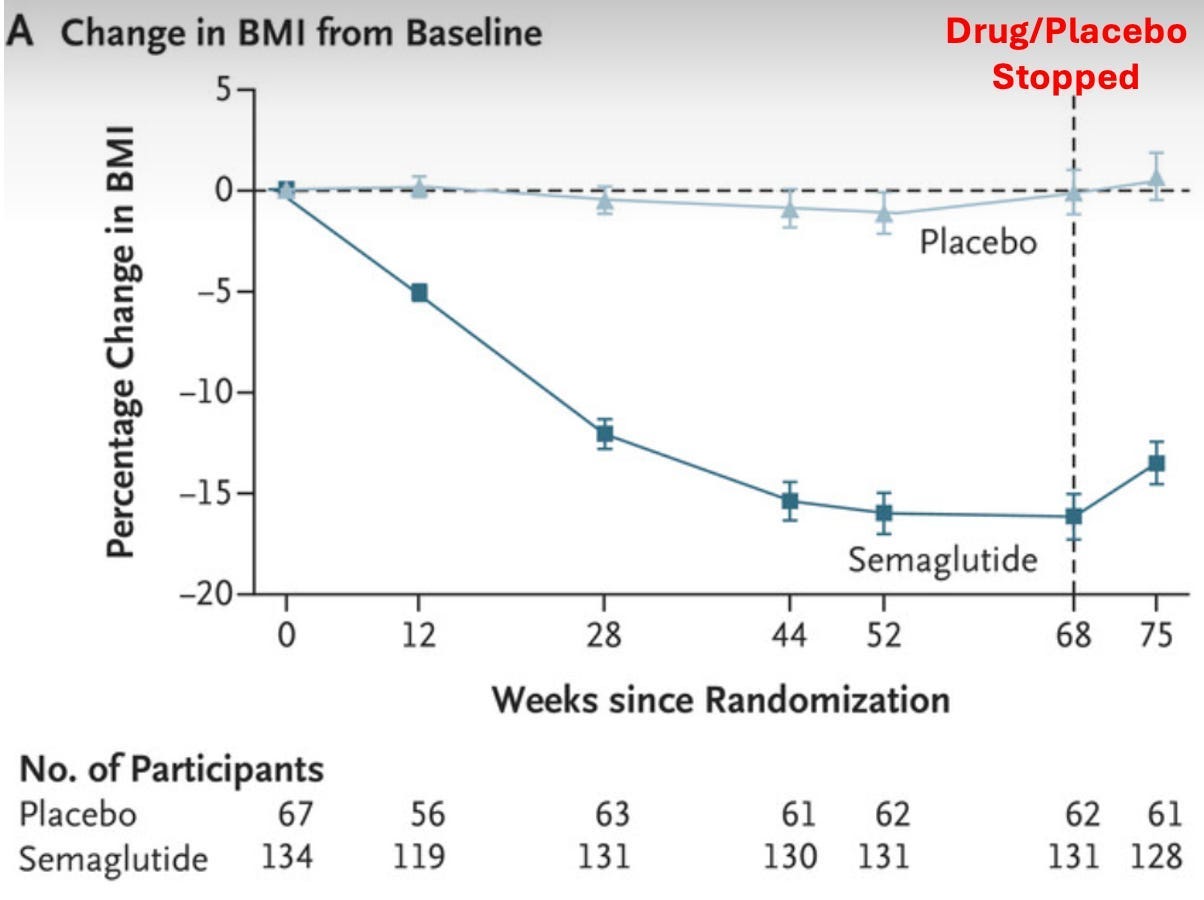
I then looked into the data on the GLP-1 drugs and noticed a curious pattern—just like fen-phen, the weight lost was rapidly regained once the drug was stopped. To illustrate, here are a few graphs from the pivotal trials of these drugs.
First, using the full (2.4mg) dose of Wegovy (which like Ozempic is another name for semaglutide) each week, inadvertently shows that most of the participants could not stay on the drugs for a prolonged period:
Second, when given to children, they began regaining their lost weight once they stopped the drug:
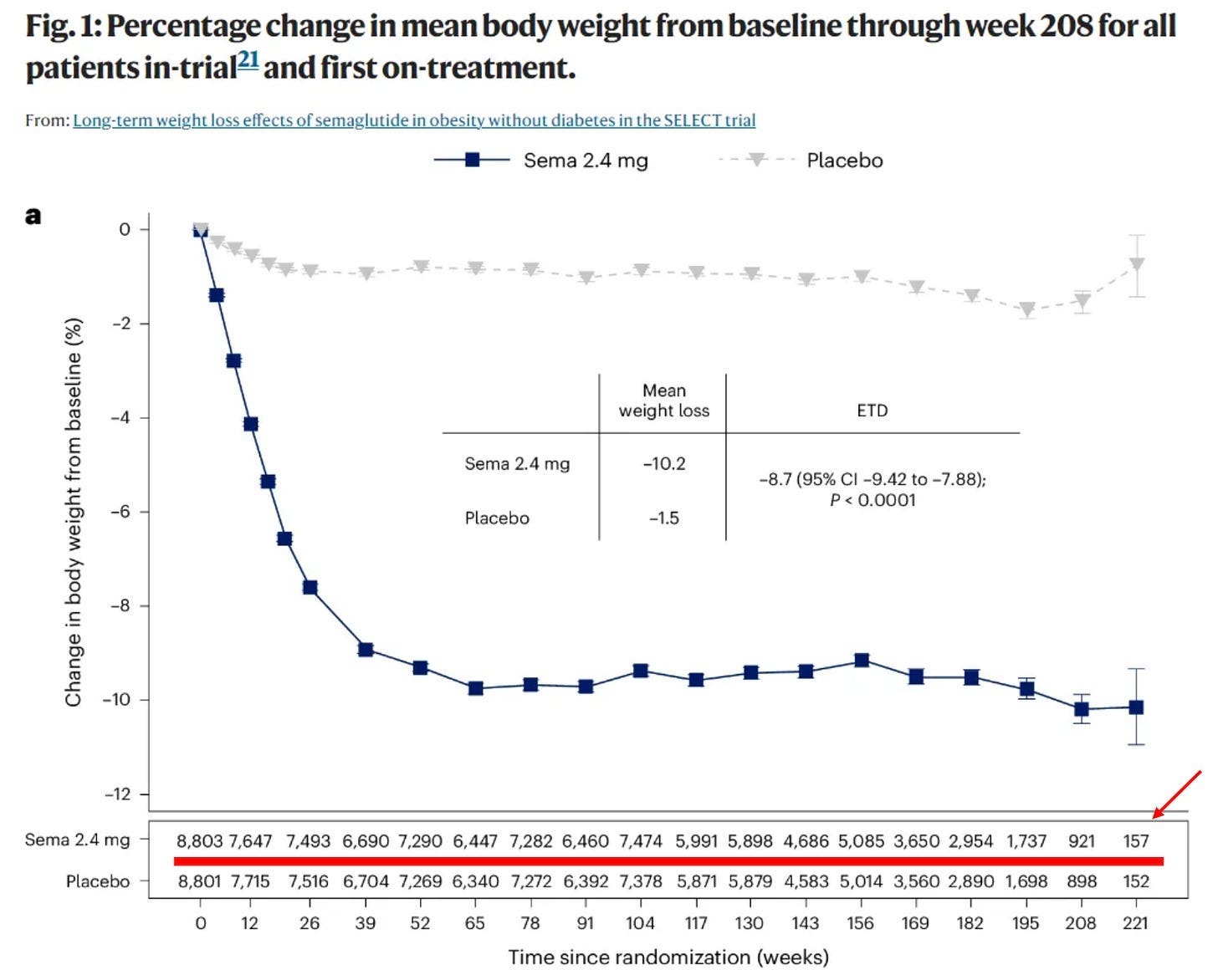
Third, when the effects of withdrawing the drug were tested, the lost weight was clearly shown to return (alongside a gradual decline in the number of people who could stay on the drug):
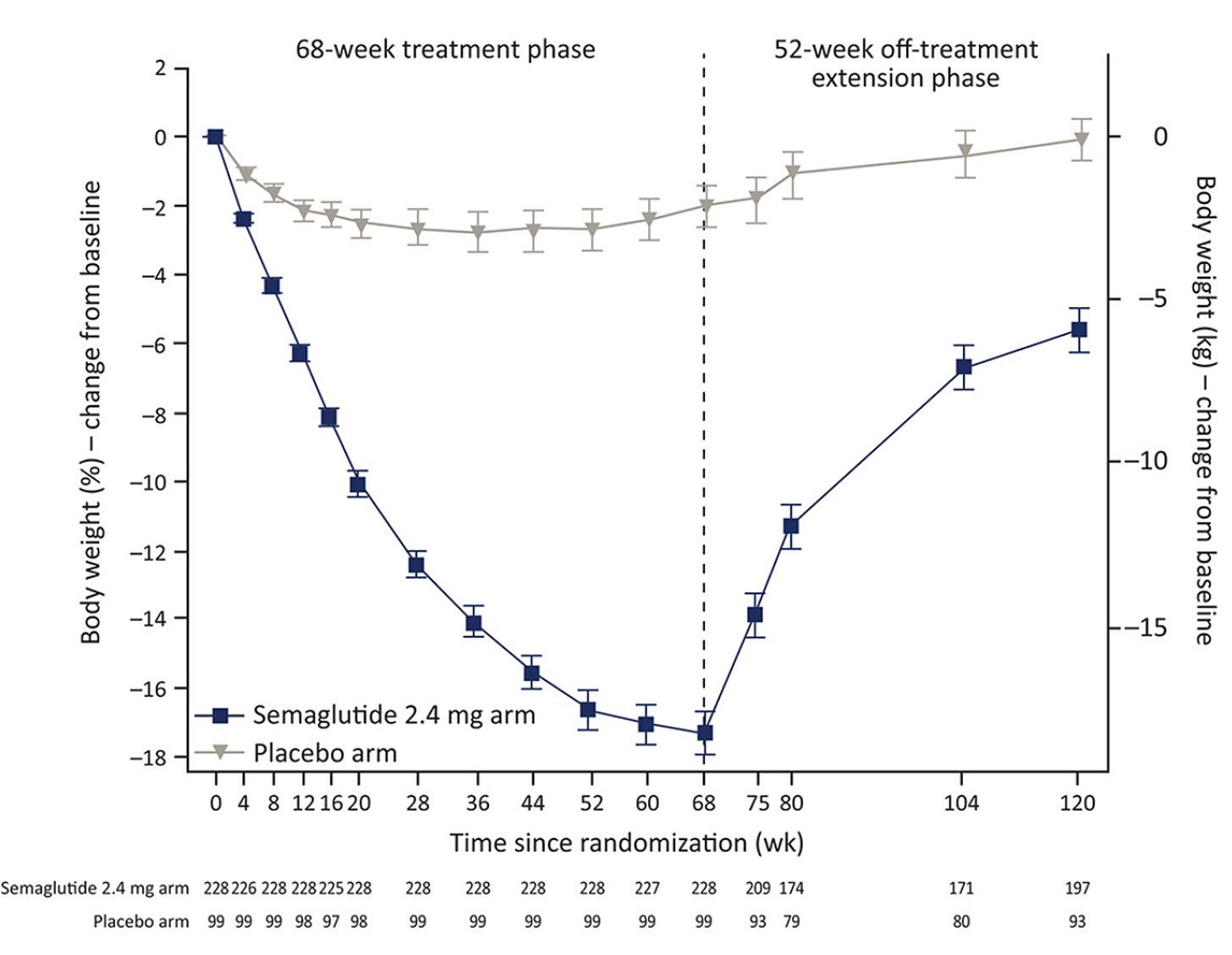
Note: the weight regained was proportional to the weight initially lost.
In short, having to spend 1000 dollars a month for a bit of weight loss, which then disappears once you stop the drug, may not be the best deal. Conversely, I suspect a key reason why this side effect has been publicized is that the goal of the pharmaceutical industry is always to have a large number of people perpetually using a high profit margin product (e.g., a monthly course of the thousand dollar Ozempic costs less than 5 dollars to make), so any product which doesn’t fix the underlying issue but creates intolerable withdrawals when one stops (e.g., the SSRI antidepressants or the PPI acid reflux medications) is “good for business.”
Unfortunately, in addition to being a scam, Ozempic has a few major issues.
First, the GLP-1 drugs were designed to resist being broken down within the body, so they would only need to be injected once a week (resulting in their average half-life being approximately seven days, whereas the natural GLP-1 protein has a half-life between 1.5-5 minutes). Since the GLP-1 is responsible for slowing digestion in the body, drugs like Ozempic significantly slow digestion and can create a variety of gastrointestinal issues from doing so (e.g., a study of 25,617 real-world patients found these drugs cause a 3.5 times increase in the rate of intestinal obstruction).
Second, severe side effects are quite common. The most comprehensive study I’ve found of the severe side effects of GLP-1 drugs (e.g., Ozempic) sourced from 16 million patients' medical records found that the drugs were strongly linked to a variety of side effects that frequently required hospitalization. Specifically, when compared to another weight loss combination not typically associated with these effects, GLP-1 users were found to have:
9.09 times greater risk of pancreatitis
4.22 times greater risk of bowel obstruction
3.67 times greater risk of gastroparesis (which means you can barely eat because the stomach is constantly full—and in many cases after Ozempic, ends up being permanent)
1.48 times greater risk of biliary disease (e.g., painful gallstones)
Third, severe adverse events are typically much rarer than moderate or minor ones. Given how frequent these severe effects are, it should come as no surprise that less severe ones are even more common.
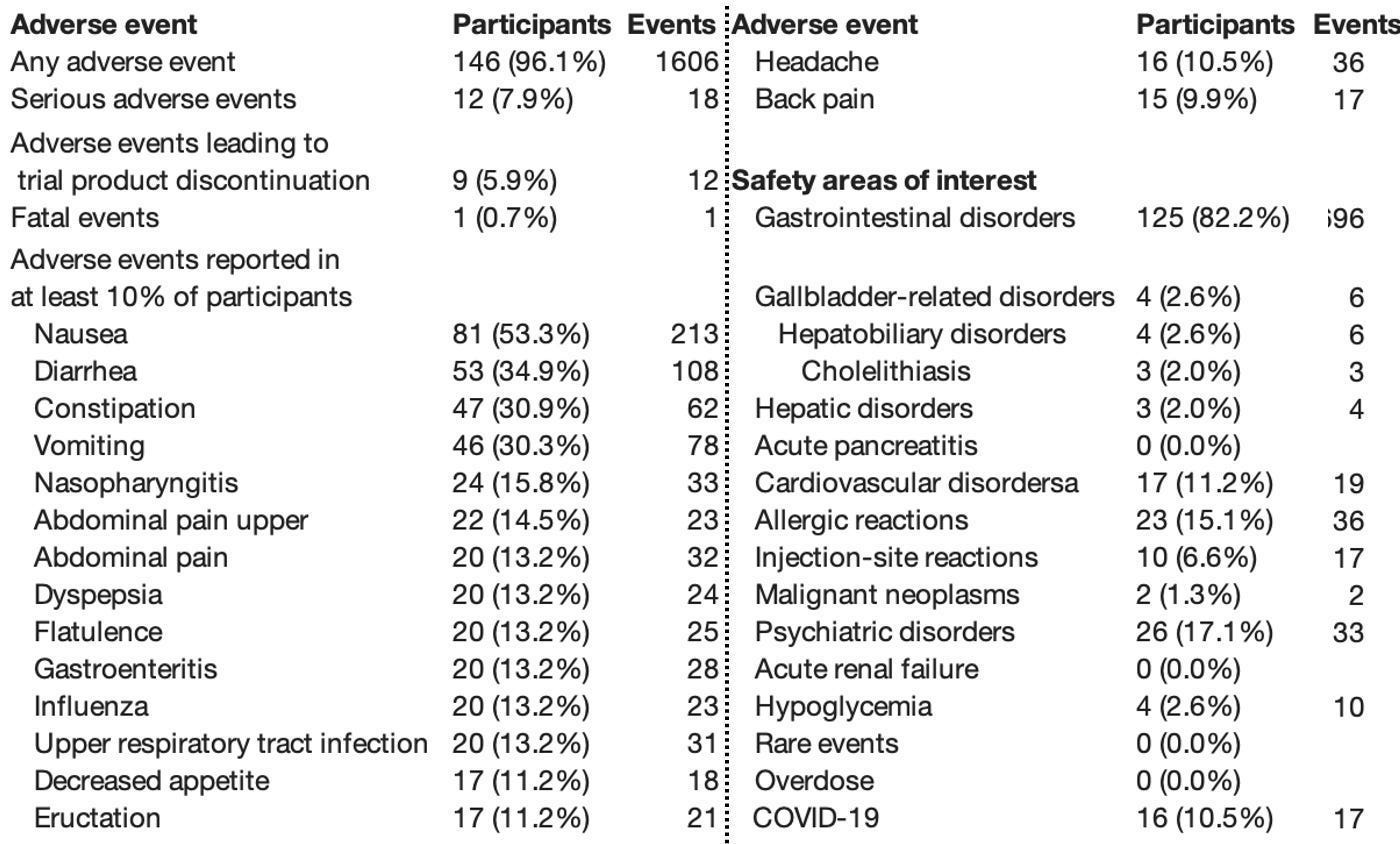
For example, consider a study of 175 people on the weight loss dose of Ozempic:

Likewise, consider how many adverse events were acknowledged within a trial sponsored by Ozempic’s manufacturer:
Furthermore, these aren’t just statistics. Consider these stories I’ve received from readers on 𝕏:
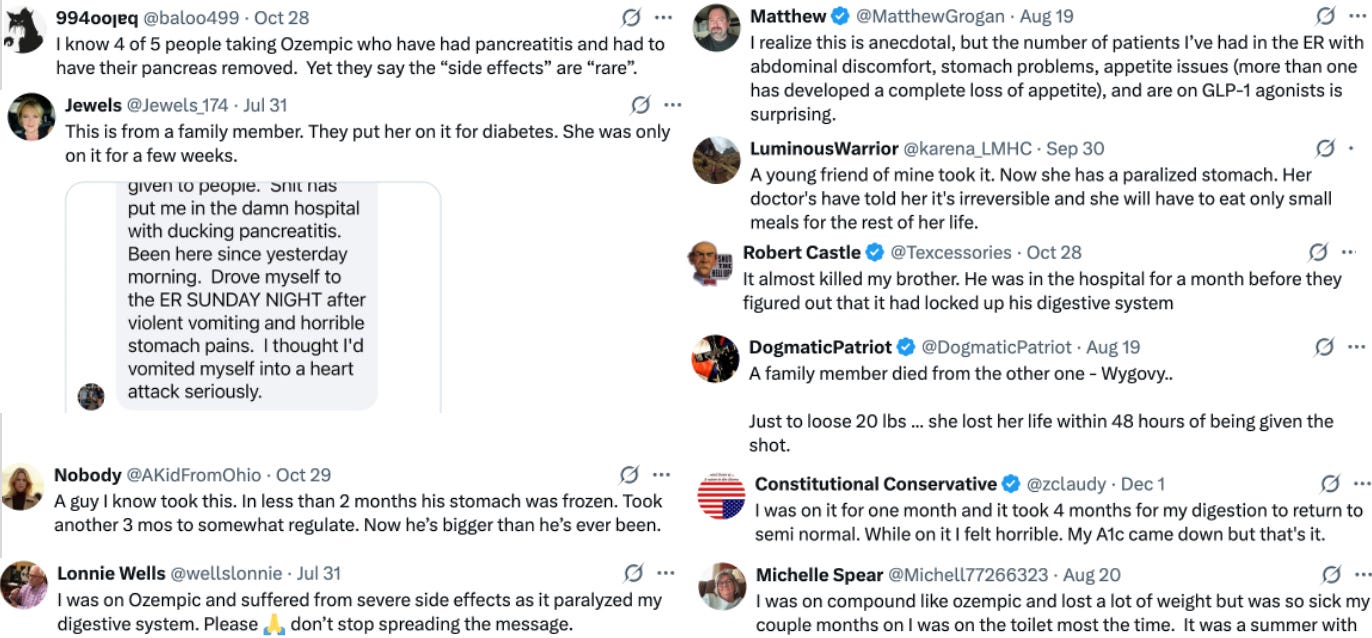

Note: my Twitter (𝕏) account (where I collect stories like these) can be accessed here.
Sadly, these aren’t the only side effects. For example, in addition to lawsuits being filed against Ozempic for gastrointestinal disorders such as gastroparesis, lawsuits are also emerging for other severe conditions such as vision loss. Furthermore, animal experiments are showing it distorts the architecture of the small intestine (which can lead to poor nutrient absorption or chronic intestinal obstructions), and many of the GLP-1 drug labels state the drugs may be linked to thyroid cancer.
Note: in a previous series, I discussed one of the largest issues with the SSRI antidepressants—because they are given at a very high dose, individuals frequently experience severe withdrawals when their dose is changed. These withdrawals, in turn can trigger suicidal behavior, psychosis, or violent behavior, which is sometimes homicidal (and a common theme in most school shootings). A major issue with Ozempic is that since it slows the rate at which the stomach empties, it alters and delays the absorption of psychiatric medications. Since the users are often very sensitive to changes in their dose, many reports now exist online of significant psychiatric destabilization occurring in Ozempic users who were also on psychiatric medications. This may in part, explain why a study found that Ozempic caused a 45% increased risk of suicidal ideation, and that increased to 345% in those who were already taking SSRI antidepressants.
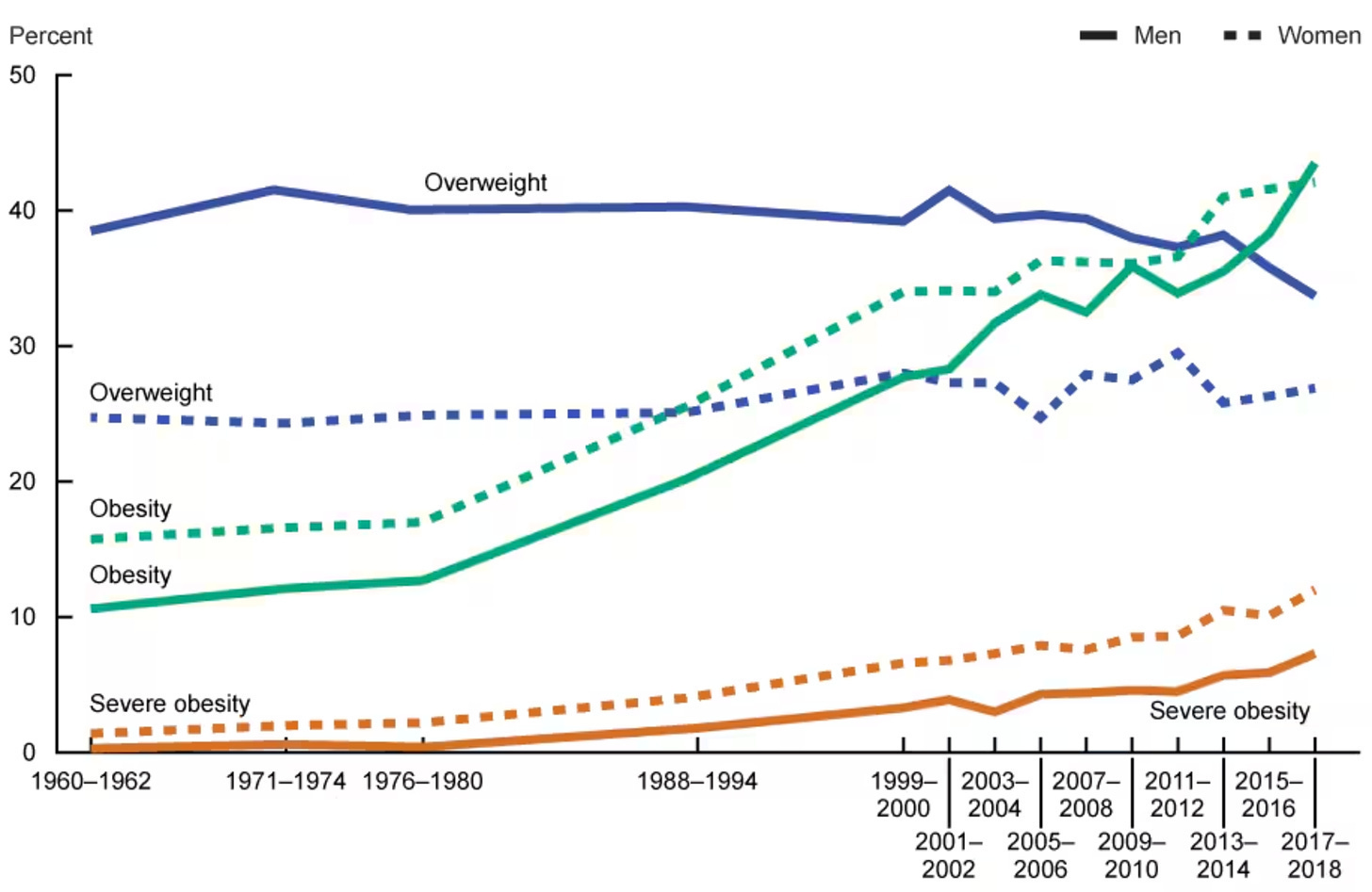
What Causes Obesity
In America’s case, it’s very clear that obesity has been continuously rising and that, like many other chronic illnesses, we haven’t been given an explanation for why it is happening.
Reasonable explanations for this increase include:
•We are eating too much food now and having a sedentary lifestyle.
•Specific additives in our foods (e.g., seed oils or high fructose corn syrup) rapidly trigger obesity within the body.
•The core ingredients of our diet are highly effective at making individuals gain weight and hence should not compose the majority of our diets. Yet, despite this being well known, due to decades of fraudulent research done to protect the food industry, animal fats are normally blamed for the consequences of eating ultra processed food diets.
•Gut microbiome dysbiosis triggers obesity.
•There is widespread metabolic dysfunction in society (e.g., due to mitochondrial or thyroid dysfunction), which causes the same amount of calories to make us gain significantly more weight than we otherwise would.
•The estrogen mimicking compounds present throughout our environment (e.g., from plastics, soy, or birth control pills designed to resist degradation and persist in the water supply) are causing widespread obesity.
•Other environmental pollutants. Joe Pizzorno ND (an expert in this area), for example, presents evidence here making the case the following pollutants each account for a significant fraction of the diabetes cases we see: Arsenic (18%), BPA (14%), Dioxins (other than PCBs) (4%), OCPs (3%), PCBs (13%), Phthalates (22%), PAHs (16%).
•A less overt version of type 1 diabetes (where the immune system attacks the pancreas and disables its production of insulin), which leads to a chronic insulin deficiency.
However, rather than taking these into serious consideration, we’re simply being told the true answer is a lifetime of Ozempic. Fortunately however, the changing political landscape is offering a real hope to reverse this tide of obesity and corruption we are facing.
Home Cooking
One of the primary ways the ruling class controls and profits off the population is by monopolizing life essential resources. As such, the most viable way to escape this is to have parallel systems you can rely upon for those resources (e.g., I’ve promoted DMSO here because it’s a very cheap way to address a myriad of issues which would otherwise require costly medical care). Unfortunately, to protect these lucrative monopolies, again and again, a similar pattern emerges; the cheaper and superior alternatives that allow one to escape these monopolies tend to be systematically buried.
This, I believe, is why beyond our food supply being flooded with addictive and unhealthy food, it is not only frequently difficult to procure the natural ingredients one needs to produce healthy food from scratch, but that many Americans, particularly in the younger generations simply do not know how to cook. I mention this because ultimately, the only way this entire junk food issue can be solved is by reclaiming the traditional knowledge of how to grow your own food (or live somewhere where you can procure it locally) and knowing how to cook it.
For that reason (and because I thought you’d appreciate it), I wanted to share what the readers of this community—on the recent open thread—shared they prepared or ate for Christmas dinner.
Here’s a concise roundup of what commenters shared about their meals:
•Roast duck with Brussels sprouts and mashed sweet potatoes
•Whole beef tenderloin with asparagus
•Grass-fed T-bone steak and shrimp & grits
•Traditional Polish: borscht, pierogi, stuffed cabbage, homemade sourdough
•Venison tips, collards, baked corn, homemade sourdough, tiramisu
•Beef roast or tenderloin (multiple mentions)
•Swiss cheese fondue
•Roast pork, Danish sausages, red cabbage, rum pudding (Danish tradition)
•Ham with various sides (scalloped potatoes, cornbread stuffing, sweet potatoes, green beans)
•Cornish hens with delicata squash
•Leg of lamb with roasted vegetables and Yorkshire pudding
•Standing rib roast with mashed potatoes and Brussels sprouts
•Turkey breast or traditional turkey dinner
•Steaks and big salad
•Pizza with homemade sourdough crust
•Chinese hot pot or take-out
Common themes: homemade, traditional/family recipes, grass-fed or high-quality meats, real/whole foods, sourdough bread, and an emphasis on cooking from scratch. Very little processed food mentioned.
Note: the above list was AI generated from all the comments on that thread and unedited so it would accurately represent that sample and its healthy avoidance of processed food.
Lastly, for those struggling with cooking (either due to a lack of time, or knowledge on preparing food), one solution many find extremely helpful are slow cookers (or Instant Pots), as it takes very little of your own time or effort to prepare wholesome food from natural ingredients with them.
Conclusion
As my life progressed, I came to see more and more that decisions at every scale, regardless of what people said, were ultimately driven by what made money and by tracing the flow of capital, I found I could often “predict” what was coming next. As I’ve shown here, the Ozempic story is egregious, but it also highlights something most healthcare professionals do not appreciate: medical guidelines are shaped far more by economic incentives (e.g., what makes money) than by scientific evidence.
Along these lines, I have a great deal of disdain for the FDA’s actions over the decades. Again and again (Ozempic being just the latest example), the agency has chosen policies that ran against the public interest and its own regulatory responsibilities, instead creating lucrative “opportunities” for the pharmaceutical industry. Worse still, in many cases (as we saw with the COVID vaccines), it chose to defend toxic products regardless of the scale of public protest.
Fortunately, nature always has a way of restoring balance. As corruption within our medical system has reached the point of absurdity, and as increasingly dangerous drugs are pushed onto the public by regulators, more and more people are waking up. The public hence is becoming less willing to accept official narratives and less receptive to reflexively “trusting the experts.”
In our case, this has contributed to the rise of the MAHA movement, which views cleaning up the food supply as one of the most critical (and economical) steps toward restoring health. More surprisingly, it has also created an almost surreal situation (one I never expected to see in my lifetime) where FDA leadership is openly discussing real health issues and pushing back against some of the lucrative pharmaceuticals that have harmed Americans for decades.
For example, consider this recent brief interview with the head of the FDA, which touches on several topics (including Ozempic) that I’ve tried to bring awareness to throughout this publication, and which, to the best of my knowledge, have never been raised by federal H.H.S. leadership before.
Note: the critical importance of natural light (and the toxicity of artificial light) Makary alluded to is discussed further here. The importance of sleep, and the harm caused by circadian disruption in adolescents, is discussed here.
In this vein, I believe the Ozempic situation is a pivotal moment, as the tables have turned since the era of Fen-Phen. Now, rather than resistance coming from regulators, it is being driven by a new wave of health-minded Americans who do not want unnecessary and damaging drugs pushed on their kids.
At the same time, while a deeply entrenched culture had established itself within the regulatory apparatus that worked closely with industry (as seen, for example, in how Califf promoted indefensible products throughout the Biden years), this shift in public consciousness has created the political will to install genuinely health-minded officials such as Kennedy and Makary. This is an extraordinary convergence, as I do not believe anything else could have stopped the momentum behind a voracious drug market projected to approach $100 billion a year in annual sales.
Note: This is an abridged article. In the full version, I discuss the above points in more detail and explore the causes of food cravings alongside natural methods for restoring metabolic health and our preferred methods for losing weight. For more sources and links on this subject, click here.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.
Apparently they weren’t making enough money as it was because they are now pushing its use in cats.
I am a pharmacist and worked for pharma for 29 years - both prior to pharma paying for their approvals and after. My point of view was that one regulatory change bastardized the very protections that were supposed to to be there from the FDA. No longer an independent regulator/reviewer, the agency was now beholding to the very bodies they were to regulate. The pre-pay for approval FDA was golden. The people who worked their saw thru mission as protecting the public from the very nonsense that goes on today. The scientists there were truly professionals who knew all the possible work arounds and short cuts and didn’t let any company get away with it. There is a drug for benign prostatic hypertrophy, first in class. When the drug failed to met its endpoints, they raised the number of patients in the trials to extreme amounts, forcing the statistics to comply. I went to the public FDA session for its approval - I did not work for this company. I knew the statistics were slanted toward positivity only because of the extreme increase in patients. So did the FDA statistician. When the statistician got up to speak and started to address the issue in increased patients forcing the statistics to positivity, he was quickly cut off. I was young in those days. I was stunned. That was the beginning of the end of the FDA I had known. Old now as I watch drugs approved I’m disgusted. A cancer drug for breast cancer with a70 percent and great chance of diabetes, Alzheimer’s drugs tgat don’t work, GLP-1 drugs that haven’t even begun to show their evil. GLP-1 drugs were fashioned after a heila monsters venom. Why was anyone surprised by the gut paralysis? Im saddened that we no longer care enough to do this right. But everyday I go to work I see the old drugs that were highly scrutinized by my old FDA still being used and still working better than the newer ones. God bless us all. It’s all we got.