The Simple Ways to Restore Sexual Health
June's Open Thread

One of the major issues in medicine is that because time is so compressed, it has become impossible for most doctors trapped within fifteen-minute-visits to provide the real healing that requires a real doctor-patient relationship. Because of that, when I started this newsletter, my goal was to be able to correspond with the readers who reached out to me, but as this publication grew, that became increasingly less feasible (especially now that there are 359,000 readers here).
The best solution I was able to come up with was to have monthly open threads where readers could publicly ask any question they had which remain from the last month (as that makes it much faster to answer the questions and everyone can see them) and then tag that to a shorter topic many readers have requested here.
As context for this month’s article, a few months ago, as I was finishing up the DMSO series, I polled you to see which topics had the most reader interest and found by far that was for DMSO and neurological conditions. As such, despite that being the most challenging topic to start with (it required my compiling and presenting over 3,000 studies along with a comparable number of remarkable recoveries from readers) I did so and have now essentially finished that series which in four parts shows how DMSO heals:
•Central nervous system disorders (e.g., Alzheimer’s, Parkinsons, ALS, MS, Cognitive Impairment, Developmental Delay, and various psychiatric disorders).
•Spinal cord injuries, paralysis, and a wide range of spinal pain (e.g., disc issues, radiculopathies, sciatica, surgery complications, ankylosing spondylitis).
•Peripheral nerve disorders, neuropathies and neuropathic pain (e.g., migraines, trigeminal neuralgia, CRPS, carpal tunnel syndrome, diabetic neuropathy, MG).
•Strokes and traumatic brain injuries (which still needs to be updated with all the additional studies I’ve found but nonetheless has provided enough information to allow many readers to avoid the disastrous complications of a stroke).
While this was challenging to do, I’m glad I did it, in part because I wanted to provide the information readers here felt could most immediately help them, but also because many of the studies in those four articles elucidated the core therapeutic mechanisms of DMSO such as it:
•Reducing inflammation and congestion (e.g., by increasing lymphatic circulation).1,2
•Increasing circulation (both for larger vessels but also for the microcirculation by preventing blood cells from clumping together).1,2
•Rebalancing the nervous system by uncompressing nerves, resetting dysfunctional circuits, blocking counterproductive pain transmission and activating the parasympathetic nervous system.1,2
•Protecting tissue (particularly within the brain and spinal cord) from a wide range of otherwise lethal stressors by preserving cellular architecture and effectively scavenging free radicals along with promoting cellular regrowth through cellular resets, elimination of scar tissue or adhesions, neuronal resealing, and microtubule stabilization.1,2,3,4,5
However, while neurology was the most requested topic by readers, male sexual health was the second, so over the last month, in addition to working on compiling that article, I’ve also discussed the material extensively with experienced colleagues in this field.
DMSO and Sexual Health
As DMSO’s therapeutic properties address the root causes of a wide range of diseases, in addition to them alleviating challenging neurological disorders, they also address many challenging disorders of the reproductive tract faced by both men and women, that, once again, medicine consistently falls short in addressing, and since publishing this series, I’ve received an astonishing number of stories from readers whose issues resolved thanks to DMSO which match what’s reported in the literature (e.g., infertility, menstrual issues including cramps or longstanding complications from childbirth). Recently, I finished compiling all of the studies and reader reports (that can be read here), which shows DMSO heals:
•Prostate issues such as BPH (which many readers reported improving), prostate stones, prostatitis (including many cases that did not respond to conventional therapies), and prostate cancer—particularly when used in conjunction with another off-patent therapy (along with mitigating complications from cancer).
•Testicular injuries (e.g., protecting them from radiation or blood loss due to torsions), epididymitis improving fertility (and providing a means to create a safe reversible male birth control) and scrotal injuries.
•Erectile dysfunction, genital infections (e.g., warts or herpes), Peyronie’s disease, priapisms (blood stuck in the penis producing erections over 4 hours, which, after 24 hours often permanently damage the penis), pelvic floor dysfunction, and sexual dysfunction resulting from other genitourinary issues (e.g., prostatitis).
The Disease Men Hide
Erectile dysfunction (ED) occupies a strange place in medicine, as it is simultaneously one of the most common conditions men face and one of the least honestly discussed. During my training, I was struck both by how common it was (as in my social circle I’d almost never heard about it except from their partners) and how mean medicine was to men about it. For instance, the favored terminology for ED until fairly recently was “impotence” —effectively a declaration the man is unworthy for having the condition.
Studies hence show men are reluctant to bring up ED with their doctors (particularly female physicians) and my experience tracks this, as typically I only hear about it either because a regretful spouse mentions it or because the man informs me some other “unrelated” therapy I or someone I sent them to administered incidentally fixed their ED (at which point they are happy to share their results).
More than anything else, what bothered me about the way ED was handled was that it was typically viewed as a psychological problem and hence put the burden and responsibility back onto the man once he opened up enough to share his issue with his doctor. In contrast, seeing men develop ED after something which logically could cause ED or their recoveries after receiving therapies which would plausibly address the (non-psychological causes) of ED made me disdain how this issue was handled by my peers and the doctors I trained under. Somewhat ironically, this issue was ultimately addressed by Pfizer, as in their push to mass market Viagra, they made significant investments in educating doctors to instead view ED as a circulatory issue (that hence could be treated with their [side-effect ridden] pill), and as such, the emphasis on the psychological causes of ED has decreased in medicine (although you still see it in older doctors whose training predates that campaign).
Note: While often effective, the PDE5 inhibitors (e.g., Viagra, Cialis) only override one step of the process (sustaining the nitric oxide signal) without addressing why the erection was failing in the first place. This is part of why they so often stop working as the underlying vascular or neurological problem progresses. They also carry a consistent set of side effects from dilating blood vessels throughout the body: headaches in roughly 10–25% of users (depending on dose), facial flushing in 10–18%, nasal congestion in 5–10%, indigestion in 5–12%, and with Cialis, back or muscle aches in up to 10% (along with having rarer but more severe side effects). Sildenafil (Viagra) also temporarily tints vision a faint blue-green (cyanopsia) in around 3–6% of users (a quirk of it slightly cross-inhibiting an enzyme used in color vision). It’s harmless but a telling reminder that these drugs act well beyond their intended target. All of which goes back to a core principle of natural medicine: a pill that masks the problem is rarely as good long-term as restoring the circulation, nerves, and tissue health a part of the body actually depends upon.
Given this, I’d like to briefly review the physiology of an erection and common ways it can go awry.
An erection is fundamentally a hydraulic event. The shaft of the penis contains two columns of spongy tissue (the corpora cavernosa) threaded with smooth muscle, and most of the time that smooth muscle sits in a state of mild contraction (held there by the sympathetic nervous system), which keeps the spaces within it squeezed shut (preventing it from expanding) and the penis hence flaccid. Arousal reverses this, as sacral parasympathetic nerves signal the smooth muscle to relax, primarily by releasing nitric oxide, which is the same pathway Viagra works on (Viagra doesn’t create that signal, it simply keeps it from being broken down, which is why it only works when arousal is already present). As the smooth muscle relaxes, the spongy chambers open and arterial blood rushes in to engorge them, and as they swell they press the draining veins flat against the surrounding sheath, trapping the blood inside and sustaining the erection.
All of this can therefore be disrupted by:
Poor circulation, which is the big one (and by most estimates the single most common cause, accounting for the majority of ED), and which is why ED is so often the first warning sign of cardiovascular disease, frequently preceding a heart attack by three to five years, since the penile arteries are small and hence clog before the coronary ones do. Diabetes, high blood pressure, smoking, obesity and atherosclerosis all tend to show up here first, which is part of why ED should always prompt a look at the rest of the cardiovascular system (e.g., in studies of men with advanced heart disease, ED was present before the heart attack in 64% of cases).
Note: our preferred ways for dealing with heart disease and poor circulation are discussed here.Medications, an enormous and underappreciated category, since a long list of common drugs can cause ED (often without the prescribing doctor ever connecting the two). For example:
•Blood pressure medications (which disrupt circulation), particularly beta-blockers are the most well known for doing this (and making patients miserable).
Note: the dangers of blood pressure medications and over treating blood pressure (along with natural ways to address the condition) are discussed here.
•SSRI antidepressants often cause (often permanent) sexual dysfunction for roughly half of users doctors rarely warn patients about. For example, one study found SSRIs caused sexual dysfunction in 59% of 1,022 patients who’d had a normal sex life beforehand, with 31% experiencing erectile dysfunction specifically, and worse still, a subset of patients develop what is now termed Post-SSRI Sexual Dysfunction (PSSD), in which the genital numbness, loss of libido and erectile dysfunction persist long after the drug is stopped, sometimes permanently.
Note: the dangers of SSRIs and natural alternatives for depression are discussed here.
•Finasteride (which neutralized testosterone and is often prescribed for hair loss or BPH), causes a host of severe issues for men including lasting ED.1
Note: the ways DMSO mitigates finasteride’s toxicity is discussed here and the ways it provides a safe option for hair regrowth here.•GnRH agonists like Lupron (used for prostate cancer and a range of off-label disturbing purposes like blocking puberty) are extremely toxic because they shut down the body’s hormone production, with one of their many side effects being ED (e.g., one study found a 267% increase in ED1 while another found 80% of men on these drugs reported impotence1).
Note: I suspect DMSO’s nerve healing properties would likely allow it to counteract longterm ED induced by pharmaceuticals, but I have no direct experience in this area.Nerve impairment, since the signal originates in the sacrum, which means anything that compromises those nerves (spinal stenosis, disc problems, sacral nerve impingement, pelvic surgery such as prostatectomy, or diabetic neuropathy) can produce ED even when blood flow is perfectly fine.
Pelvic floor dysfunction, where an overtight, spasming pelvic floor physically compresses the arteries and nerves feeding the penis, which is both common and badly underdiagnosed.
Low testosterone, which while very common in men, is less of a direct cause of ED than people assume (it affects desire more than the erection mechanics themselves) but nonetheless contributes.
Chronic prostatitis, where inflammation in the prostate frequently causes or worsens ED through pain, inflammation, and the pelvic floor tension that accompanies it.
Peyronie’s disease where fibrous scar tissue (plaques) forms inside the penis’s outer layer, causing curvature (which can be uncomfortable for the partner), shortening, pain, or erectile dysfunction (due to the plaques obstructing distal blood flow into the penis)—estimated to affect around 10% of men, although only 0.5–1% of cases are formally diagnosed, as many men do not seek care. In many cases, early Peyronie’s disease (which is the easiest to treat but lacks the classic symptoms and hence requires ultrasound to detect) goes undetected but nonetheless contributes to ED. For example, in a study of 386 men undergoing Doppler ultrasound for ED or penile pain (without curvature or palpable plaques), 41 (10.6%) had detectable Peyronie’s plaques. Of these, 73% had ED as their main complaint, and about half showed reduced blood flow distal to the plaques. Other studies have also found higher rates of ED in men with subclinical Peyronie’s, with roughly 10% of men presenting with ED showing varying degrees of Peyronie’s disease (especially in longer-lasting or more severe cases).1,2
Note: Peyronie’s is quite difficult to treat, as all options are less than satisfactory (e.g., traction therapy requires hours each day for months and typically offers only partial improvements in early cases, ED medications like Viagra help with erections but do not fix the plaque, about half of patients benefit from injections of collagen-dissolving enzymes, and while surgery can straighten more severe cases, it often has side effects that can worsen sexual function).Lifestyle and psychological factors, which round out the picture, since obesity, heavy alcohol use, poor sleep and a sedentary life all contribute to ED through their effects on circulation and hormones, and (as discussed earlier) genuine psychological causes such as pornography and also past trauma exist—in turn making it critical to recognize ED (like many conditions medicine consigns into a small box) is often not an isolated issue but rather part of broader disruption to one’s health.
Note: the primary psychological cause of ED we do see now (which was not possible in the past) is pornography addictions (an association which has clearly been shown in some studies1,2 while others found a weaker correlation1,2), and to a lesser extent past-sexual trauma (which men are even more reluctant to speak about than ED1).
DMSO and Erectile Dysfunction
As with other therapies, my knowledge DMSO helped ED originally emerged from readers sharing rather remarkable stories like these with me which they often accidentally discovered while using DMSO:
A minute or two after applying the DMSO I had this unanticipated erection, I mean a raging hard-on. Mind blowing. I’m a 75-year old male with no ED problems, but having so much pelvic pain, I haven’t had, nor thought about sex for a long time. I wasn’t having any stimulating thoughts, I was just going through my self-medication routine.
We are a 60 and 58 year old couple [and] have been using DMSO for a little over a year now. We have 4 grown children and I (the wife) had 3 episiotomies that left me with scar tissue. Never bothered me until post menopause when sex became very painful. I began applying DMSO pain relief. The scarring healed and sex is no longer painful. My husband then developed ED [and applied DMSO]. We are happy to say we again have a great sex life and are so empowered to have “cured” ourselves.
Likewise, others reported similar success after directly trying DMSO for ED.
I have had sore feet for 30 years due to high arches and the DMSO topically relieved the pain greatly. I have had ED I assume from statin use for over 20 years and I thought, hmmmm improves blood flow why not.I started having “movement.” Damn amazing. Thanks AMD.1,2,3
I had the same thought and after a week or so, the difference was significant. So, yes, I will second the use of DMSO to improve penile blood flow [for erectile dysfunction].
Finally, some individuals without overt ED nonetheless noticed the same effects:
I was suffering form low testosterone after a weight cut and I used DMSO on my private areas for pimples after shaving & it seems to have stopped the pimples. Within a few hours I was getting erections non-stop, it sort of revived my testosterone, like a wake-up call for my gonads to start working. I noticed my erections were much much harder & stiffer erections, nothing extreme but for someone who is health & gyms, I was impressed. You may use these testimonials but please remove my name.
While these results seem quite surprising, once you understand the causes of ED and the therapeutic effects of DMSO (e.g., increased blood flow, parasympathetic activity and muscle relaxation) they fit well within DMSO’s expected effects. Furthermore, extensive research has demonstrated DMSO’s affinity for addressing erectile issues.
Existing Research
The most concrete piece of evidence is that DMSO directly relaxes the erectile tissue. In isolated strips of human corpus cavernosum (the exact smooth muscle that must relax for an erection) pre-contracted with phenylephrine, DMSO produced dose-dependent relaxation beginning at extraordinarily low concentrations (from around 10⁻⁹ M) and reaching roughly 29% maximal relaxation,1,2 with a separate study finding that at higher concentrations it abolished resting tension entirely.1 In turn, because DMSO is absorbed through skin so readily, the concentrations that relax this tissue are easily reached by simply applying it topically, which is to say DMSO does, on its own, a version of exactly what the erectile machinery is supposed to do (with the chronology of reader reports directly corroborating this).
That relaxant effect compounds when DMSO is used to carry an erectogenic agent, and because it relaxes the tissue independently, the benefit credited to each agent is measured against DMSO’s own baseline (meaning part of the shared effect is likely DMSO’s). As a 50% vehicle it potentiated Viagra’s relaxation of cavernosal smooth muscle roughly 16- to 80-fold,1 and in men whose ED no longer responded to PDE5 inhibitors like Viagra at all, DMSO still relaxed their erectile tissue directly (and potentiated other types of ED drugs1). Most notably, testosterone (which DMSO both independently raises and is often used to topically drive into the body) dissolved in DMSO produced a rapid, dose-dependent relaxation of erectile tissue taken from men with ED, reaching 41-71% (far exceeding DMSO alone).1,2,3
Note: many other natural and pharmaceutical agents combined with DMSO have also been shown to increase erections and treat ED (which are listed here). Among these, DMSO has even served as the vehicle for nitric-oxide-releasing nanoparticles that induced spontaneous erections in a post-prostatectomy model, the situation that so commonly leaves men with ED after prostate surgery.1
DMSO has also been shown to address a variety of conditions which can trigger ED:
Tight pelvic floor musculature frequently contributes to ED. In one Russian study,1 vaginal DMSO was shown (via EMG) to measurably relax the pelvic floor (levator ani muscles) and normalized their resting electrical activity (shifting 85% of patients toward a normal EMG pattern with reduced activity on straining); this normalization of pelvic-floor muscle tone paralleled relief of their pelvic pain, leading the authors to conclude DMSO exerts analgesic, anti-inflammatory and muscle-relaxant effects on the pelvic floor. While this specific route of administration is not possible for men, given DMSO’s ability to spread through tissue and reports readers have shared with me, the same effect appears achievable if needed for ED.
Because DMSO dissolves scar tissue and dissolves collagen aggregates (along with it downregulating fibroblast type I and III collagen synthesis in human foreskin1), it has been successfully used to treat a variety of challenging contractile collagen deposition disorders like Peyronie’s disease along with other protein deposition disorders (e.g., topical DMSO has also been utilized for localized urethral amyloidosis).1
In turn, across the original urological DMSO studies, topical DMSO improved roughly half of Peyronie’s patients (6 of 13 in one series, and softening or resolution of 2 of 4 patients’ plaques in a separate preliminary report).1,2,3 DMSO combined with prednisolone was also developed as a local Peyronie’s treatment in the 1970s.1,2 Larger combination regimens built on this. In 66 men treated with topical 50-70% DMSO daily over 20 sessions (alongside other conservative agents), plaques shrank in 72.7%, dissolved completely in 18.1%, softened in 43.9%, curvature improved in 37.9%, erectile function improved in 42.4%, and pain resolved in most.1,2 In a long-term protocol centered on topical 50-70% DMSO rubbed into the plaque twice daily, 5 of 6 evaluable patients fully recovered with no recurrence over 2-4 years and the sixth stabilized with restored erectile function.1 Another multimodal series of 41 patients including topical 20-25% DMSO reported pain relief in 54%, improved sexual activity in 38%, and plaque/curvature reduction in 40%.1Note: DMSO has been also been used in numerous other publications to treat Peyronie’s,1,2,3 often combined with a variety of other agents,1 and appears in the standard reviews of Peyronie’s treatment options.1
However, while it frequently helped Peyronie’s disease, a meaningful response was typically only seen in half of cases, making it more ideal as a first line therapy (in the hopes it could avoid the need for less ideal options)—although once combined with one forgotten therapy, dramatically better results were seen for not only Peyronie’s but also other challenging contractile disorders DMSO had notable success for like scleroderma and Dupuytren's.Chronic prostatitis frequently drives ED (through the inflammation, pain and pelvic floor tension it creates) so studies which treated prostatitis with DMSO repeatedly found erectile function recovered too. For example, in 52 men with stubborn chlamydial chronic prostatitis complicated by ED, adding DMSO (mixed into a proteolytic enzyme solution) to the treatment protocol not only addressed the infection but also raised the rate of normal erectile function to 72.2% (versus 41.1% in controls), alongside greater eradication of the infection, shrinkage of the prostate, and improvements in pain, cytokine profiles and quality of life.1,2,3 Likewise, a 1981 study of men with chronic prostatitis, vesiculitis and urethritis found DMSO with novocaine, calendula and Benadryl caused all 24 treated patients to have their libido, erection, ejaculation and orgasm fully recover (compared to 13 of 20 controls on standard therapy).1 Likewise, another study found that adding DMSO microclysters to antibiotic therapy roughly halved the ED score relative to antibiotics alone, with greater reductions in pain, dysuria (pain with urination) and prostatic inflammation.1
Note: a few of the BPH formulations I came across (e.g., camphor-DMSO rectal emulsions and suppositories) likewise listed improved erectile function among their benefits.1,2
One author reported that in four cases of genital herpes the patients were able to have sexual intercourse after only two days of treatment, and DMSO let men resume intercourse where pain or urethral blockage had previously made it impossible.1
Lastly, as mentioned above, due to DMSO’s utility in treating ED, a variety of combinations have been successfully explored to commercialize this un-patentable discovery (e.g., one topical preparation combined DMSO with local anesthetics and botanical extracts to prolong intercourse and reduce premature ejaculation1).
Of these, one was particularly noteworthy to me, as I’ve come to recognize that (due to its tissue tolerability and broad range of therapeutic effects) virtually every way DMSO could be applied has been (with the possible exception of direct injections into the lymphatics—something I suspect could be quite helpful in cancer due to Walter Bryant Guy1,2 and Gaston Naessens discoveries1,2—but to the best of my knowledge has only been done in animals). However, despite that, DMSO researchers have devised quite a few means of administration I would have never thought of.
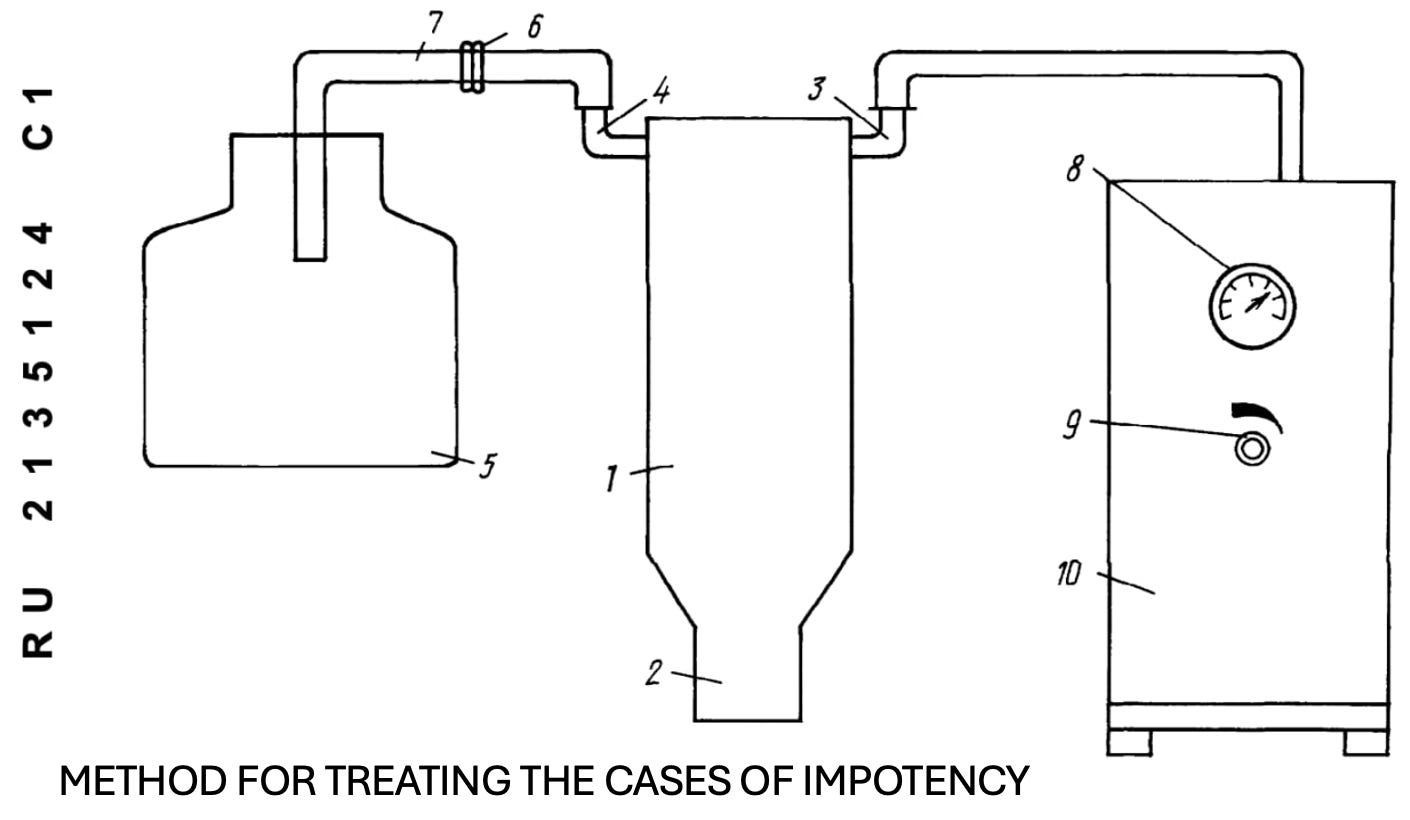
One Russian patent treated various forms of ED by mixing DMSO with 2% papaverine alone or additionally with 1% nicotinic acid and then applying it to the penis by submerging it in a vacuum flask at 0.3-0.6 atm pressure filled to half volume with the warmed solution (36-42°C) for 5-12 minutes per session, conducted daily or every other day for 5-10 sessions. This worked, as in all 20 ED patients under 50 years of age (and 72% of those over 50), there was an adequate restoration of erections enabling sexual intercourse, and for the remaining 28% of older patients improvements were still seen.1,2
Note: while effective, I feel simpler DMSO applications likely would have sufficed.
A New Way of Seeing the Body
As nature is inherently complex, boiling it down to the simple sum of a few parts is inevitably bound to miss much of the broader picture that must always be considered, but nonetheless, both because these reductionist frameworks are so much easier to implement and because the false security they provide (by seeming to eliminate the unknowns of life) is so seductive, we continuously adopt them. In medicine, this mindset has led us to view the body as an automated machine we can predictably control, which on one level has been remarkably helpful, as it has made it possible to redirect the acute course of a variety of otherwise lethal conditions. Simultaneously however, it has left us unable to address a vast range of other problems, and instead forced us into a model of using ever-increasing amounts of drugs to inadequately manage chronic illnesses which continue to progress regardless.
This is why I find something like DMSO so significant, as the fact that a single agent can resolve so many seemingly unrelated conditions (often ones medicine considers separate diseases with separate mechanisms), and do so in a manner many of you can directly observe in your own lives, is itself a sign that our way of carving the body into isolated parts and targeting them one at a time is missing something fundamental. Rather than DMSO being an anomaly to explain away, my hope is that it is beginning to illustrate a different way of seeing the body, one in which the circulation, the nerves, the connective tissue and the body’s capacity to regenerate are all deeply interconnected, so that restoring those underlying functions does far more than any number of drugs aimed at suppressing one isolated pathway at a time ever could. Until we are willing to look at the body that way, many diseases will remain incurable, treatments like DMSO will keep being discarded rather than embraced, and the many people they could have helped (such as the men told their ED was either in their heads or something they would simply have to live with) will keep being failed by a model that was never able to see them in the first place.
In the last part of this article (which serves as an open forum for you to ask any remaining questions that have accumulated over this month) I will review exactly how DMSO is used to treat erectile dysfunction, other treatments we’ve seen work over the years for challenging cases (including those arising from trauma), more general protocols for how DMSO can be used for urogenital issues in both genders and common male issues like Benign Prostatic Hyperplasia and how Stanley Jacob enhanced DMSO’s efficacy for fibrotic conditions (e.g. Peyronie’s and Dupuytren's).
