The Critical Calculation Medicine Won't Make
How a simple framework reveals that "proven" therapies often lack value while the "unproven" ones lack only approval

Story at a Glance:
As decisions always have pros and cons, making the correct one is often quite challenging. One framework, “expected value” (EV), solves this puzzle by calculating the relative probability of a good (positive) and bad (negative) outcome.
In medicine, while frameworks like EV should be used to guide medical policies and clinical decisions, they frequently are not, resulting in practices like mass COVID vaccination which have explicitly negative EVs being adopted and then held to regardless of public pushback or evidence to the contrary.
Much of this stems from our widespread societal faith that large randomized controlled trials (RCTs) are the definitive arbiter of scientific truth, despite their numerous shortcomings. In contrast, valid and affordable approaches for determining scientific truth are continually marginalized, making it nearly impossible to “prove” competing therapies work or that sanctioned therapies have serious harms.
Much of this originated from two subjective linguistic interpretations which the FDA then used to prohibit the public’s access to life-changing (but non-commercializable) therapies like DMSO and protect its industry sponsors—which as DMSO stories in this article show, has created profound consequences that have been well-hidden from all of us.
This article will explore how this dysfunctional dynamic has harmed the health of America, meaningful changes that could preserve the vital functions of the FDA while simultaneously preventing it from sabotaging America’s health, and the changing political winds we’ve helped create which are gradually forcing those changes to happen.
The majority of decisions in life aren’t clear cut as they have both an upside and a downside (or multiple upsides and downsides). However, rather than being fully cognizant of the complexity of the decision, the human mind will typically narrow the picture and see only one side of the coin to reduce this large cognitive load. Many perpetually unresolved political conflicts essentially result from this, as each side emotionally primes their adherents to focus on the arguments in favor of their position and those which undermine the other side, resulting in both sides having a view of reality where their side is correct and the other is irredeemably wrong—which in some cases holds true, but typically is not.
One of my favorite frameworks for encapsulating this paradigm is the biostatistics concept of “sensitivity and specificity,” which denote how likely a test is to catch something that is there (sensitivity) and how likely it is not to overshoot and only identify things that are actually there (specificity). The value of this framework (beyond providing an informed way to choose medical tests) is that it emphasizes the reciprocal relationship between the two, as if one is increased (e.g., more aggressively screening for something), the other decreases (e.g., that screen will have a higher rate of false positives).
Because of this, ideally, the sensitivity and specificity of a test (and what will then be done with either result) should be appropriate to a patient’s clinical situation and in parallel, work is always done to improve the tests themselves so better balances between sensitivity and specificity can be met. In contrast, in overly politicized issues (e.g., criminal justice), the focus always ends up being on maximizing sensitivity OR specificity rather than finding a reasonable compromise between the two, which maximizes both as much as is feasible.
However, the reality is that you will frequently be confronted with situations where there is a less than ideal balance of upsides and downsides (e.g., sensitivity and specificity) between the two options, but a choice nonetheless must be made. Fortunately, due to how common these situations are, effective decision making strategies have been developed and refined.
Predicting Expected Values
The classic mathematical formula used to “solve” these situations is expected value (EV), which essentially calculates “on average, how much will this situation benefit or harm me.”
This translates to (magnitude of outcome 1 * probability of outcome 1) + (magnitude of outcome 2 * probability of outcome 2), and this is repeated for all possible outcomes (e.g., it could go to calculating outcome 10) so that the total probabilities add up to 1. So for example, if you had a situation where you paid a dollar to flip 2 coins and then got 99 cents for each “heads” you got, the EV for the four outcomes (HH, HT, TH, TT) would be (1.98*0.25)+(0.99*0.25)+(0.99*0.25)+(0*0.25) or $0.99. Given that your cost to play this game is $1.00, it is hence “not a good idea” to play the game as there is a negative DV (on average you will lose money).
Many businesses (beyond just casinos), in turn, are essentially structured so that the EV of the transactions they make are positive for them (and negative for the customer) hence (excluding highly unusual circumstances) ensuring a steady stream of profit which sustains the business or industry.
While everyone has a general grasp of EV (e.g., if you saw a dollar bill fly into the freeway, almost no one runs onto the highway to try to grab it as the risk of being hit by a car makes the EV very bad there), a few points are critical to understand about it:
First, most people do not have a strong grasp of probabilities, and as such, predatory industries will frequently mislead them about the actual probabilities, leading them to believe bad EV choices are actually good EV choices.
Second, rather than being a simple binary calculation, EV calculations are often complicated because there are many potential outcomes (variables).
Third, EV can encompass a variety of outcomes beyond financial gains or losses, at which point it becomes harder to fit into a numerical formula.
For example, many of the policies that were pushed on us during COVID-19 essentially arose from people being implicitly presented with erroneous EV formulas by the mass media, and then extrapolating decisions off those formulas which appeared beneficial (positive EV) but in reality were harmful (negative EV) with a correct formula.
To illustrate, the odds of a child dying from COVID-19 were effectively 0 (and in the small number who died, there was almost always a severe underlying condition), so no real benefit could be derived from vaccinating, whereas injuries (including fatal ones) routinely occurred. So, the EV of a child taking the COVID vaccine was always negative (as there was no “positive” outcome, whereas a negative one could occur).
Likewise, when the Pfizer NEJM paper came out (which made many, including most of the medical profession, decide they had to get the vaccine no matter what since it was “95% effective!” and would end the pandemic), the paper itself stated:
Adverse reactions were much more common in the vaccine than the placebo group (27% vs 12% for a direct event and 21% vs. 5% for an unrelated adverse event)
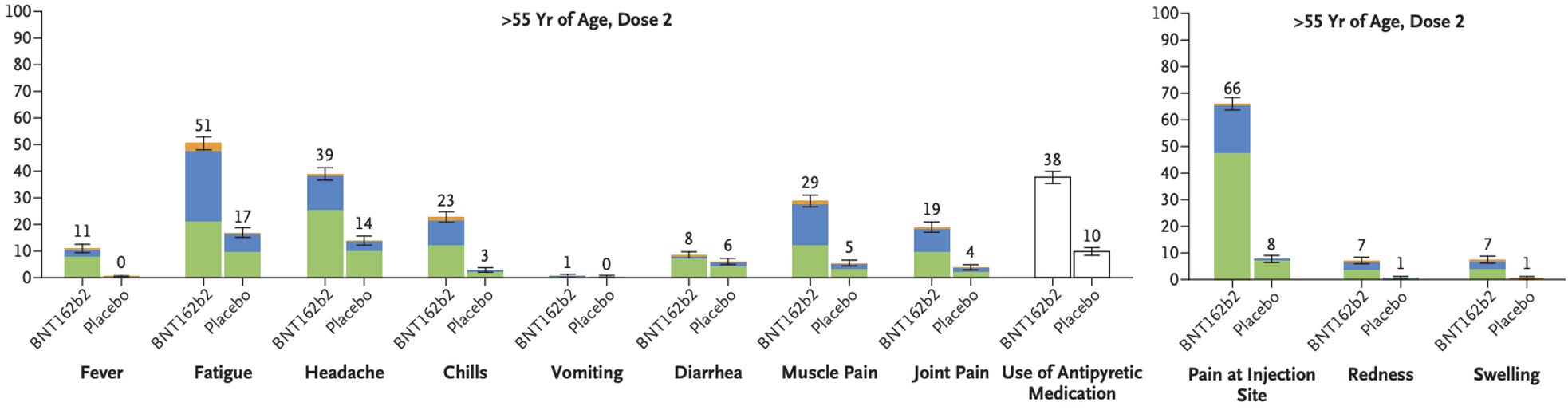
In contrast, for COVID infections, those same symptoms occurred, typically 1-2 times as frequently (sometimes 3x).
8/18,198 (0.044%) vaccinated developed COVID and 162/18,325 (0.88%) of the unvaccinated developed COVID (a 20-fold decrease).
Seven days after the initial dose, 1/18,198 vaccinated and 9/18,325 unvaccinated developed severe COVID (COVID typically requiring hospital care).
Note: this metric was changed to after the first vaccine (whereas the primary efficacy measurement ones were after the second vaccine), since 5 of the severe infections in the placebo group happened prior to the seven day post vaccine cut-off (which was hidden in the appendix). Had this standard been used for all COVID infections too, it would have been (39+8)/18,198 vs. (82+162)/18,325 (a 5.16 fold decrease falling far short of the “95% effective” benchmark), whereas had the study’s primary criteria been used here, it would have been 1/18,198 vs. 4/18,325 (a 4-fold rather than 9-fold decrease)—illustrating how studies always change their metrics and criteria in whatever manner makes the product look best.4 serious adverse events attributed to vaccination were reported (shoulder injury from injection, right axillary lymphadenopathy, paroxysmal ventricular arrhythmia, and right leg paresthesia).
2 vaccine recipients died and 4 placebo recipients died (all from causes unrelated to COVID-19).
Nothing in this study evaluated transmission.
When I read this paper, I was jaw dropped, as it was blatantly stating there was an extremely negative EV for the vaccine as you were trading the symptoms from a COVID infection for a 1/119 chance (0.88%-0.044%) of not getting COVID, so if you assumed COVID-19 symptoms on average were twice as frequent as vaccine symptoms you were increasing your likelihood of getting ill 60-fold by vaccinating (along with the injection site specific symptoms only seen from the vaccine) in return for a possible halving of COVID symptoms (although in reality, people often felt far worse post-vaccine than during COVID). If you attempted to counterweight that by the major benefits of vaccine, the most important one, death, was not prevented, while the medium one “severe COVID” had required between 2,293 to 6,123 vaccinations to prevent one instance (with the higher figure arising if a consistent metric had been used by Pfizer), and the only other possible justification for vaccinating (reducing transmission) had not been tested in the paper.
Furthermore, since fairly consistent methods are used to doctor papers, I was relatively certain:
•Vaccine efficacy had been overstated (e.g., COVID cases in vaccine recipients were not reported) and severe injuries in vaccine recipients also were not reported—both of which were later corroborated by numerous trial participants and trial researchers.
Note: while the trials were happening (inspired by what I’d learned happened in the Gardasil trials where many of the reported adverse events were magically erased), I joined online support groups for the trial participants and noted that many of the adverse events they reported did not appear in the final trial report, and that the overall severity from a reaction to the vaccine was significantly worse than what I typically saw people experience with COVID-19. My suspicion adverse reactions were covered up in the trial solidified once the vaccine hit the market, because almost immediately, I had multiple patients each day seeking help for severe and unusual vaccine reactions and people I knew from around the country began contacting me to ask if the vaccine could cause strokes or heart attack (as it had happened to someone they knew)—and most importantly, my sample size for these early reports was far smaller than the 18,198 vaccine recipients in the trial.
•Any benefits not reported in this paper (e.g., transmission or reducing death) would never be found for this vaccine as every possible attempt had been made to exaggerate the benefits and they could only decline from this point forward (e.g., before long everyone would have immunity to the original strain and COVID-19 would mutate to something no longer covered by the vaccine).
Note: at a six month follow up, deaths were slightly higher in the vaccinated than the unvaccinated group. Likewise, despite there being no evidence that the vaccine prevented transmission (and its symptom-reducing design arguing against this even being possible) health authorities and the media widely promoted the vaccine as preventing transmission to pressure people to vaccinate, until real life data forced them to backtrack on their claim.
•Flipping the criteria for severe COVID-19 (compared to minor COVID) to make the vaccine look better demonstrated that data manipulation was occurring in the paper (hence casting everything else into doubt). Later, as I started noticing a lot of people become severe ill with COVID-19 (and in many cases dying) immediately after vaccinating (including individuals who had minor PCR confirmed asymptomatic infections), I realized this issue had most likely been detected by Pfizer and hence why the criteria for evaluating COVID hospitalizations was changed to “seven days post the second vaccination” (which resulted in many vaccine COVID-19 deaths being labeled as “unvaccinated” deaths).
Note: “disease provocation” due to vaccine-induced immune suppression is a longstanding problem with vaccination (e.g., a good case can be made many of the pre-polio vaccine polio outbreaks were due to vaccination, COVID-19 was the two most common fatal COVID vaccine reactions reported to VAERS and longitudinal data showed the more COVID vaccines you got the more likely you were to get COVID-19)—all of which is discussed here.
Put differently, my immediate thought after looking at the paper was that if after all their best attempts to make the vaccine look as good as possible, it was still this bad, it meant the actual data was likely appalling. Remarkably however, when I discussed this paper my physician colleagues, they could only “see” the 95% effective figure (the 20-fold relative reduction) and all the other points I raised, which were in the paper, went in one ear and out the other, hence illustrating that most people simply do not have a good grab on probabilistic reasoning (outside of those in competitive fields where optimizing EV choices is necessary for success).
Note: the formula which goes hand in hand with EV is Bayes’ theorem [P(A|B) = [P(B|A) × P(A)] / P(B)], which provides a method for updating the probability of something being true as new evidence becomes available. In medicine, it is essential for correctly interpreting diagnostic tests (e.g., understanding that a positive result from a screening test in a low-risk population is more likely to be a false positive than a true one), yet remarkably few physicians actively apply it in their clinical reasoning1,2—which in turn leads to a significant amount of overtesting (some of which in fairness, they know is not justified but is done to avoid potentially being sued), overdiagnosis, and unnecessary treatment.
Finally, it should be noted that the EV of the COVID vaccines was much easier to calculate than that of most other vaccines in use (because there was a much smaller set of variables and much more available data on those variables). For example, to begin calculating the benefit of a routine vaccination, you first need to start with:
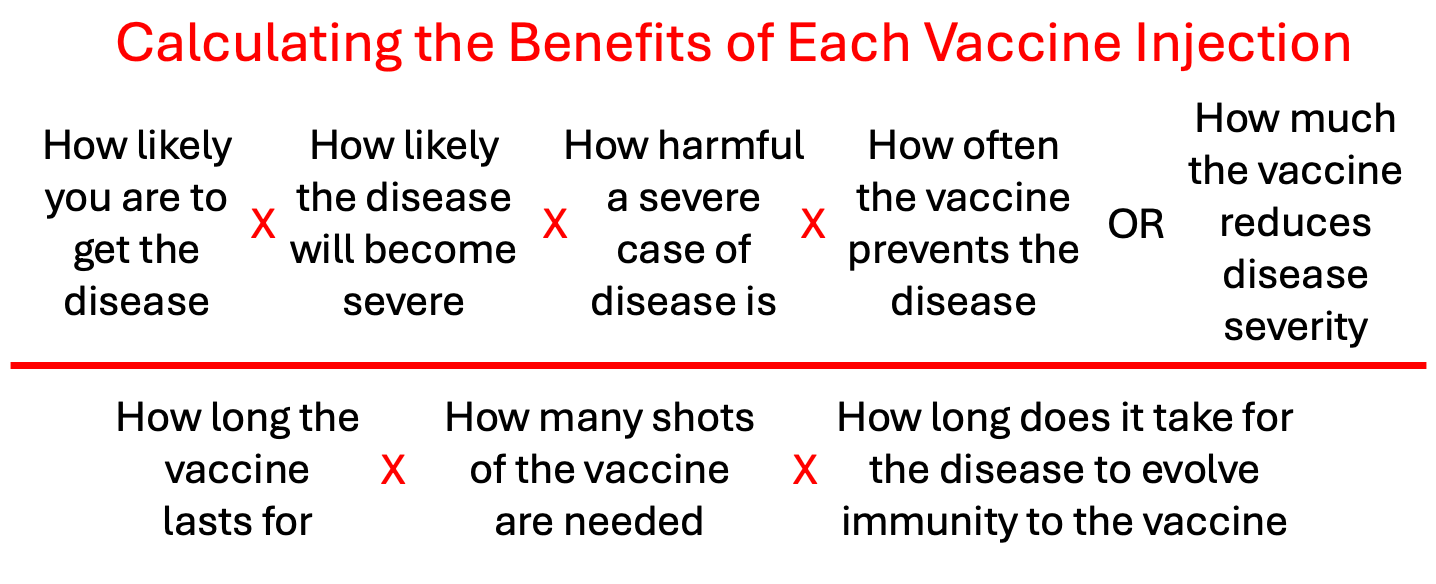
Then you need to weigh that against the risks of each vaccine in the series (as later ones typically cause more injuries), with separate calculations done for each degree of injury severity, along with subgroup susceptibility (as some people are much more sensitive to vaccine injury than others) and then once that is done, somehow assess the cumulative effect of all the different vaccines being taken (as vaccine toxicity and immune dysregulation are cumulative). However, rather than try to engage in that complex calculation, the medical industry’s solution has been to assume all vaccines are “magically safe and effective” and like the COVID vaccine, give both incredibly optimistic models of efficacy while only focusing on a few inconsequential reactions (e.g., temporary injection site reactions).
As such, much in the same way doctors were convinced the COVID-19 vaccines would end COVID because it was “95% effective” (when nothing of the sort then happened) and that the vaccine was much safer than getting COVID (despite trial data indicating the opposite), virtually no knowledge exists on the actual EV of most vaccines because they were given a simplified formula to calculate them which only highlights a few key variables industry wants people to focus (which arrive at a high EV). This sales strategy, in turn, is quite effective as it allows people to avoid the hard mental work of having to complete a complex calculation (hence appealing to human laziness), while simultaneously appealing to the human ego by providing the illusion of mastery and authority in the area (by regurgitating the simple arguments used to authoritatively enshrine a positive EV for the vaccines).
Note: a while back I tried to calculate the risks and benefits of each childhood vaccine (as they vary immensely with some being much worse than others)—all of which is detailed here.
Lastly, it should be acknowledged that the original emergency use authorizations for the COVID vaccines were granted under the premise that no other treatment existed, the vaccine's massive potential benefit justified the existing uncertainty over its effectiveness, and that authorization could be modified as more data emerged. However, not only did other treatments already exist, the FDA then shredded the EV of the vaccines by continually doubling down as more and more evidence of ineffectiveness and harm accumulated.
Stagnating Science
The following holds true for our current society:
•It highly values science and scientific truth to the point that many people worship it in place of religion.
•In order for science to be “valid” (and widely promoted by the media) two bars typically must be cleared—a large randomized control trial is conducted that arrives at a statistically significant corroborating outcome and the scientific authorities must bless a given scientific conclusion.
In some cases, this is a very helpful framework, but in many instances, it is extremely vulnerable to abuse. This is because:
•Large RCTs are extremely expensive (tens of millions of dollars), to the point that they typically can only be financed by national governments, massive pseudo-non profits (e.g., the Gates Foundation), or pharmaceutical companies.
•Any controversial study that somehow makes it through that ideological filter will still often be routinely dismissed by the medical authorities (and in many cases retracted once too many people start citing it).
•Studies that do not meet this threshold are very easy to dismiss, and will virtually always be dismissed if they arrive at a conclusion that threatens a major interest.
Note: it is very common for the abstract or conclusion of a study to provide a summary which contradicts the study’s results if the actual data is “politically incorrect” or “undesirable” (as most people only ever read summaries). Fortunately, AI now makes it very easy to expose this tactic.
•Since most scientists are dependent upon either grants or pharmaceutical funding (the only two sources of funding for costly research), they quickly learn they cannot pursue “controversial research” and hence do not produce research that will tank the rest of their career.
Because of this, we’ve run into a situation where most research is highly conservative and incrementally builds upon existing discoveries rather than making new revolutionary discoveries which advance science and change paradigms. For example, this is how Gerald Pollack aptly described our current situation.
Note: anyone who has worked within research institutions over the past few decades has watched the space for unconventional inquiry steadily shrink — to the point that Nobel laureate Peter Higgs remarked he doubted any modern university would hire him, as the solitary work that produced the Higgs boson would never survive today’s academic culture. But in medicine, the problem goes further: institutional review processes that were designed to protect research subjects have increasingly become gatekeepers of orthodoxy, making it nearly impossible to obtain approval for even simple human studies on anything deemed controversial (which was incredibly frustrating for me and many others to deal with). This is why so much of the compelling research on therapies like DMSO comes from an era before these barriers existed or from countries where they still don’t.
Because of this, many major problems we face (which I believe are solvable or know have already been solved) remain major issues and we are instead continually told to provide more funding for science so those solutions can be found in the future, highlighting the unfortunate principle I discussed recently—that organizations will rarely produce solutions to the problems they continually receive funding to “solve” as doing so dries up that funding.
Note: after publishing that article, numerous readers sent me articles and interviews about the Los Angeles mayoral race, such as this interview with Joe Rogan, since the abject failures there to deal with major issues facing the city, despite vast amounts of money being spent, embody the principle I outlined. Given how egregious the situation they described is and how different it sounds from what Los Angeles was like when I visited the city roughly ten years ago, I am genuinely curious if what’s described here matches the experience of readers living in the area.
Additionally, after I learned about this, my first thought was “what specific drugs are causing people there to ‘act like zombies’?” (since the wounds looked similar to those seen from Krokodil—a corrosive homemade opioid that caused a lot of issues in Russia until over the its precusor was banned). I found out it was due to all the fentanyl being cut with xylazine, a vasoconstricting (hence wound causing) powerful animal tranquilizer (sedative) which extends the high (while putting you in a zombified stupor). Most notably, this practice persists because there are no legal restrictions on the sale of xylazine (so numerous ways exist to easily and cheaply procure it), as bipartisan efforts since 20231,2,3 to schedule (restrict) it have failed to advance through Congress, and while numerous states (recognizing the problems xylazine causes) have independently scheduled it, California has not.
Placebo Effects
Since the expectation or belief something can help you will cause people’s health (or their perception of their health) to improve, particularly on subjective metrics like depression (or things like blood pressure which shift in response to the state of the autonomic nervous system), a possibility always exists that the benefits from a therapy are actually due to the expectation the therapy will work rather than the therapy independently doing anything. However, while this concept is broadly recognized (with it frequently being used to discuss all positive results seen from alternative therapies), a few things are not widely recognized about it:
•Because of how strong the faith our culture holds in doctors is, a strong case be made that many of the benefits patients receive from medical care actually result from the placebo effect. Conversely, reverse “nocebos” also exist, where patients being told something will bad happen to them makes them become ill or accelerate the progression of their illness (often termed medical hexing).1,2,3
•The placebo effect varies widely depending on the condition, the type of outcome measured, and the treatment context. It is often quite strong for subjective symptoms that people can directly feel—such as chronic pain (commonly providing about 30% pain relief), depression, anxiety, fatigue, and nausea—where it frequently accounts for half or more of the total improvement seen in drug trials (with estimates reaching 62% or higher for antidepressants and pain medications). So for certain classes of therapies, more than half of the benefit attributed to them actually comes from the placebo effect.
•In contrast, it has little to no meaningful effect on objective biological measures like tumor size, blood sugar control in diabetes, or the underlying progression of most diseases, although it can trigger real brain changes such as dopamine release in Parkinson’s patients or modest shifts in heart rate, blood pressure, and immune function through conditioning.
•The placebo response is much stronger when the treatment feels more dramatic or “real”—such as sham surgery or injections. Likewise, with antidepressants, it has been consistently shown that if they are compared to active placebos (which mimic their adverse effects) rather than neutral placebos (which do nothing), almost all of the benefits attributed to antidepressants disappear.
Note: this may be in part due to the fact researchers, once they know patients are taking a test drug, have been found to overestimate subjective patient improvements by roughly 36% (which is close to the magnitude of benefit attributed to many psychiatric drugs).
•Certain types of placebo effects are mediated through endogenous opioids (endorphins) because naltrexone (an opioid blocker) will block the pain relief to a lesser extent depression relief medications produce.
Note: this is likely why low dose naltrexone therapy (which increases endorphins) is useful for a wide number of illnesses.
RCT Fundamentalism
Prior to the thalidomide near-disaster, the FDA was tasked with regulating drug safety rather than efficacy, with this limited regulatory enforcement power here leading to a broad swathe of misbehavior (e.g., misleading labeling and over-the-top claims) by the drug companies. The nation uproar around thalidomide, in turn, initiated a series of hearings to craft legislation to create regulatory frameworks to prevent this from ever happening again by giving the FDA broad powers to regulate both safety and efficacy
As research by the drug companies was atrocious at the time (e.g., highly anecdotal, not controlled at all) a provision was put into the 1962 law which allowed the FDA to block drugs from being marketed if “There is a lack of substantial evidence that the drug will have the effect it purports” with substantial evidence “consisting of adequate and well-controlled investigations…by qualified experts.”
This process created three major problems:
•It galvanized the agency to lean towards specificity on drug approvals (as many in the FDA wanted credit for stopping the next thalidomide) and drug approvals slowed to a crawl (while becoming exponentially expensive), leading to widespread criticisms of the FDA obstructing necessary drugs from reaching the market that have persisted ever since (e.g., complaints I’ve read in 1980 hearings are virtually identical to what I see senators say today).
Note: currently, the cost to bring a new drug to market is estimated to be between 0.98-4.54 billion dollars, which makes it impossible for any unpatentable product ever to get FDA approval.
•Secondly, it galvanized the FDA into rapidly establishing its authority and creating numerous divisions to “police” questionable drugs without the organization being structured to effectively or appropriately administer that authority (which led to perpetual mismanagement, chaos, and frequent abuse of that power).
•Third, the FDA chose to define “well-controlled” as a robust (increasingly large) double-blind trial and relentlessly held to it regardless of the public or Congressional pushback they got (except in cases where they wanted to push a drug through).
This decision, effectively instilled the culture of RCT fundamentalism, and created a climate where most doctors and government officials would habitually dismiss the results of a therapy if it did not have a costly RCT behind it, and in the years that followed, science became exponentially more expensive (and hence dependent upon an extremely limited source of funders), new discoveries stagnated, and credible unorthodox research became harder and harder to conduct.
The EV of RCTs
To be clear, RCTs are genuinely valuable—they do gradually refine the standard of care and over time sort out which approaches actually work, which is something no other method does as reliably. The issue is not with RCTs themselves, but with using the absence of an RCT as justification for blocking therapies which have compelling evidence behind them.
With that in mind, whenever I see this topic discussed, the key facet I almost never see mentioned is what the EV of this standard is, as we are effectively trading, eliminating random spontaneous improvements and placebo effects, for making research costly to the point that most of the science we want done can never be conducted.
Assuming this dynamic is the root cause of our present state of affairs, the net EV is not very good as each year more and more is spent on healthcare in the United States (in the most recent 2024 figures, 5.3 trillion or 18% of all spending), but simultaneously, we have the worst health outcomes amongst the affluent nations.
If we look at it more granularly, while accounting for the placebo effect somewhat increases the accuracy of test results, the following issues emerge:
1. The immense cost of conducting drug trials essentially guarantees that sponsors will break the blinding and doctor the data to get a positive result to secure approval (or simply not publish the study if the results are too incriminating). Because of this, the funding bias introduced often greatly outweighs the benefit gained by counteracting the placebo effect and random variation. Unfortunately, while regulators are extremely strict on many aspects of bringing a drug to market, they are surprisingly lax about addressing overt clinical trial fraud (e.g., despite numerous whistleblower complaints and citizen petitions, the FDA never investigated the fraud throughout the COVID-19 trials). All of this was best demonstrated by a definitive 2017 Cochrane review which found that industry-sponsored drug studies were 34% more likely to report favorable overall conclusions than non-industry-sponsored studies.
Note: NIH Director Jay Bhattacharya has launched a major initiative to fund and incentivize replication studies, directly reducing incentives for fraud and data manipulation. This represents the most significant systemic change since the 2007 FDA Amendments Act, which mandated prospective public registration and results reporting for many clinical trials on ClinicalTrials.gov, making it harder (not not impossible) to hide negative trial results. This, in turn, is a key reason pre-2007 research conclusions are viewed by many as far less reliable.
2. With drugs that meet approval, the magnitude of benefit, while “statistically significant” is often quite small (and likely non-existing once data manipulation is accounted for). Because of this, while accounting for the placebo effect can slightly shift the overall efficacy calculus, the net result isn’t meaningful and would not justify taking a costly drug with real side effects that patients do not want. Put differently, while large well-powered trials can detect small improvements which would otherwise be undetectable, small improvements often equate to negligible clinical benefits for the patients who will later take the drugs. This underscores a critical point; if a therapy provides a large enough benefit to provide a meaningful improvement for patients, it should not require an extravagant trial to detect it. For example, statins (which cause noticeable and sometimes debilitating side effects for around 20% of users), assuming industry RCTs are honest, will extend a man’s (but not woman’s) life by 3-4 days after they’ve been taken for 5 years, which is not a large enough EV for me to feel justified in recommending them to a patient.
Note: in many cases, multiple disease processes will create the same “illness” and a drug will only work on certain subsets of the disease (hence why in aggregate the net benefit is quite small, even though in the correct patients, it’s much larger). Unfortunately, the way our regulatory system is set up (and the way doctors are trained to think), identifying those subgroups is not prioritized, and once approval is obtained, the manufacturer has no incentive to limit sales by marketing only to the primary groups that benefit from the therapy.
3. Another Cochrane Review (which is considered to be the most definitive appraisal of medical evidence), in 2014, found that smaller (affordable) unblinded observational trials typically yielded the same results as large RCTs. This underscores another critical point; if a therapy provides a large enough benefit to justify giving it to patients, it should be possible to observe patient’s experiencing improvements from it and for any clinician to produce a small study demonstrating that.
Each of these hence argues that insisting on RCTs to determine the efficacy of a therapy has a negative EV. Instead we have a rather grotesque system where:
•Patients (and dissident researchers) are told to deny what they see with their own eyes as any observation they make which deviates from what the RCTs show must be a product of confirmation bias and false. This amongst other things, is one of the most common methods used to gaslight patients who suffer severe injuries from pharmaceutical drugs (which the manufacturers successfully lobbied to keep from being acknowledged side effects) and the most common tool used to shut down any competing therapy, even in cases where the competing therapy shows a clear and massive benefit whereas the existing one does not help the majority of patients.
•A massive “pay-to-play” scheme is created where it is nearly impossible to create “medical truth” without spending a lot of money to do so, thereby making medical dogmas shift to whatever the industry wants to be true rather than what is true or objectively helps patients. Furthermore, because of how much money is in this, and how many people are dependent on it at every level (researchers needing funding, pharmaceutical-funded experts needing prestige, regulatory bodies needing fees from drug manufacturers, regulators wanting high-paying pharmaceutical jobs in the future etc.), there is so much inertia behind the system that it is extremely hard to break free from it regardless of how irrational and illogical it seems.
•Therapies that have a massive and dramatic effect greatly exceeding what you would typically see with a therapy are dismissed for having “no evidence,” even in cases where the magnitude of benefit greatly exceeds anything which could possibly be attributed to the placebo effect.
Note: another less appreciated aspect of RCT fundamentalism is that while RCTs are well suited for testing the effect of one pill versus another, they are not well suited for testing therapies that are difficult to make true placebos for, and as a result, many things I know have a high degree of efficacy have been perpetually stuck in the limbo of having “no evidence” because the ways they can be tested do not conform to this model. Likewise, regulators are extremely insistent on therapies having a biochemical mechanistic basis to secure approval (even though in many cases—such as with SSRI antidepressants—that mechanism is later disproven) something many natural therapies (which utilize biophysics) do not have.
Finally, because it costs so much to prove a drug works for something, after obtaining the easiest approval, as this whistleblower shows, manufacturers will frequently then market the drugs for uses besides their approved indication (greatly increasing their total revenue), and at worst, occasionally get manageable fines for doing so. On one hand this is “fair” because doctors should have the right to treat as the deem appropriate (rather than having to follow strict guidelines) but it simultaneously illustrates how the FDA’s high bar for efficacy serves to protect industry monopolies rather than the public.
Note: my colleague Pierre Kory believes repurposing (find new clinically relevant uses) for already approved off-patent drugs (e.g., using ivermectin for cancer) is the weak point in this system as it bypasses both the FDA’s blockade on competing therapies that can’t afford costly approvals and does so at an affordable prices (since by being off-patent, high prices can’t be charged for them).
The Best Available Evidence
Medicine has long been an extremely dogmatic profession that is resistant to discarding existing (harmful) practices or adopting new ideas. To combat this, in the 1990s reformers introduced the idea of “evidence-based medicine” with the premise that the “best available evidence” rather than expert opinion should dictate medical care. This well-intentioned concept took off and quickly became entrenched within the medical field. Unfortunately, the industry realized this new dogma was an immense opportunity for them, as they could simply buy out the evidence (e.g., by funding only costly RCTs that supported their bottom line, controlling what medical journals would publish, and buying out the expert opinions that appraised the evidence).
All of this, I believe ultimately resulted from (much in the same way “well-controlled” was selectively defined by the FDA) “the best available evidence” being defined to mean “evidence that meets a statutory threshold” (e.g., large RCTs) rather than “the best evidence currently available for assessing a topic or clinical question” that was described in the original definition.1,2
Because of this, many topics with clearly compelling evidence are disregarded because no large RCT has been done, even though those RCTs will never conducted. For example, with vaccines, a longstanding argument by the industry is that all the data which shows vaccines increase the rats of chronic illness 3 to 7 fold (detailed here) should be discounted because they were not corroborated by large RCTs while simultaneously, large RCTs have been stonewalled on vaccines because “vaccines are so safe and effective it is unethical to ever not give them to children” (in the placebo group) and we are instead expected to default to the incredibly optimistic models used to evaluate how much benefit they provide to society.
If the actual definition of “best available evidence” being used, all of the observational studies which found high rates of harm from vaccines (greatly exceeding anything that could result from uncontrolled statistical artifacts or placebo effects) would be taken as the gold standard until better evidence (e.g., large RCTs) was produced which could displace the currently existing data. However, since the definitions have been flipped, a status quo exists in which the compelling harm of vaccination is allowed, and no “credible” research will ever be conducted on the topic.
Note: one of Secretary Kennedy’s initiatives has been to conduct that research, which predictably has been widely attacked by Senators and mainstream outlets like The New York Times for spurious reasons, such as it being too expensive, too difficult to assess accurately, and unnecessary because we already know vaccines are safe.
The EV of DMSO
I value the incredible support many have given this newsletter, so my goal has been to maximize the value I provide to people who take the time to read it. For this reason, out of the myriad of topics I write about, I’ve tried to focus on topics which are applicable to a large number of people (or fold narrow focus ones into broader articles everyone gets value from), and prioritize those where I have a useful and novel insight to offer (which for many medical topics I don’t as I largely agree with the existing consensus or simply am not familiar enough with topic to feel I can state with relative certainty an alternative approach has real merit).
As DMSO has one of the highest EVs I know of (particularly since it doesn’t require specialized care to utilize), over the last year and a half, I have worked to make a strong case that DMSO is an “umbrella remedy” which transforms the management of dozens of challenging conditions. In turn, tens and quite possibly hundreds of thousands of readers were inspired to try it, the majority of whom had positive, and frequently unbelievable results for a wide range of debilitating and often incurable ailments, while in contrast, serious side effects are virtually non-existent from the therapy, while the minor ones are fairly tolerable and reverse once DMSO is stopped (corroborating the high EV).
All of that was possible because so much scientific evidence exists corroborating DMSO’s value in a myriad of conditions, and once I started posting about it, a large number of readers here wanted to try it. This hence has left me in a rather challenging position—I feel a duty to present all the evidence (and the remarkable experiences readers have shared with me) but due to how much there is, there is no possible way to do so without it being too long. As such, I’ve tried to compress the information as much as possible down to the salient or overlapping details and then subsequently rewrite the articles in shorter formats which briefly mention much of the extensive data packed into the longer articles.
However, while that “works” I simultaneously don’t like doing it because it forces me to write fairly sterile articles devoid of the human impact and heart centered connection I try to maintain. For instance, in the most recent DMSO article I wrote:

There were many profound stories like I wanted to fully cover, but instead had to heavily abridge as my primary duty in writing these is to provide the data which can shift the needle on how DMSO is treated. For example:
A college student with severe injuries including a C4-C5 fracture who began DMSO nearly two years post-injury gradually regained sensation, limb movement, and hand function over the following years—whose progress halted when the FDA unconscionably revoked DMSO's medical use—but nonetheless healed enough to graduate
Was meant to synopsize this passage from a 1980 book on the history of DMSO:
“Quadriplegia is the saddest thing that happens to people,” [Stanley] Jacob said. “It occurs most often to the young and healthy — to soldiers fighting our wars, to youngsters driving, to athletes in contact sports.
“As a quadriplegic, you lie in bed, a total vegetable, unable to move any of your extremities. Your mind functions, but you can’t pass urine. You can’t have a bowel movement without help. You are totally dependent upon someone else to perform the basic functions — to keep you alive.”
I had asked who stood to gain most from DMSO.
“As I get to know the quadriplegics, ever so many of them eventually say to me, ‘You know, Dr. Jacob, I couldn’t even commit suicide.’”
At this time, he was treating eight quadriplegics, and of them only one had a recently incurred injury. He felt, as most doctors do, that treatment is more fruitful in new conditions than in old ones. The one fresh case was that of a sixteen-year-old girl, a fine athlete, who dove off a board and landed on her neck on the bottom of the pool.
“Her doctor was pessimistic but willing to try almost anything that offered a glimmer of hope. She was a complete quadriplegic — utterly helpless.”
She was on DMSO for an entire year. Gradually — one by one, it seemed — her organs began to function again. Eventually she walked. And now she is in college, doing very well.
It was 3:30 p.m. on Saturday, April 5, 1963. Grey Keinsley, eighteen, was driving from Greeley, where he was a freshman at the University of Northern Colorado, to Denver, where he was going to apply for a summer job with the State Highway Department. The Rocky Mountain sunshine and bracing air flooded through the open sunroof of his VW, and it might have been that open top that saved his life. To this day he doesn’t know what happened.
They lifted the athletic body off the barbed-wire fence where it had been hanging, limp and battered, and took him — still breathing but unconscious — to the Community Hospital at Longmont. The doctor said, “Have this boy’s family get here without delay.”
The way it looked to the doctors: the numerous bruises and cuts would heal in time — if there was time. One could survive the concussion. But the broken neck was another thing. X-rays showed a fracture between the fourth and fifth cervical vertebrae, a spinal cord block at that vital link in communications between the brain and the body below the neck.
When Grey heard his parents’ voices, he came out of the coma momentarily, but he was delirious for weeks.
Mrs. Dorothy M. Keinsley of Littleton, Colorado, told me of Grey’s struggle. His father was in the U.S. Army, so Grey had lived around the world. In the United States, he had been a babysitter, grocery sacker, carry-out boy, delivery boy for newspapers and heavy appliances, hamburger cook, yard worker, snow shoveler, and car washer. He had attended schools in Japan and, for three years, played on the football team at the American High School in Poitiers, France. He had been an Eagle Scout and junior scoutmaster. He said his religion was “workable.”
Grey liked girls and they liked him. He was a good student, played trombone in the high school band, danced well, sang well, knew what to do about a sick car, and stood six-feet-one. After his catastrophic accident he said, “Mom, the best part of me is intact — my mind.”
Grey was admitted to Fitzsimons General Hospital in Denver — a fringe benefit for Army families — and stayed there for six and a half months. When they transferred him to Craig Rehabilitation Hospital in West Denver, he could make only shoulder motions and flail his arms. They fitted him with carbon dioxide-powered braces on both hands, and he was able to come home for Christmas 1963.
One day the neurosurgeon asked to speak with Dorothy. “The neurosurgeon told me that henceforth Grey’s only motion would be to move his head from side to side and grin,” Mrs. Keinsley said. “If this was true, I knew Grey’s life-span would be very short. But I didn’t believe it.”
A few weeks later, the neurosurgeon gave it to Grey straight. Grey listened attentively, thought for a minute, then said to the doctor, “One day I will swing my legs off my bed and offer to bet you I am going to walk. At that time, put your money where your mouth is now.”
Mrs. Keinsley saw it this way: “We have not had adequate finances to be classified as affluent, but we’ve had twenty years of training in frugality, and this made me astute in managing.” The Keinsley mother and son got help from several sources, but all of them together didn’t quite pay the medical bills.
Mother and son drew heavily on one resource. Dorothy said, “Grey loves all life and the world. His pantheistic approach has served as a buffer against the cruelty of the world and the cruelty of man to man when adversity strikes.
“I have a strong faith that God will never give one a bigger burden than one can carry, although there have been times when I thought He punched my card twice.”
Grey read Ann Sullivan’s article about DMSO in Pageant magazine. The part about the rejuvenation of plants made him wonder: “If DMSO will do this for useless limbs on trees, what would it do for useless human limbs?” He wrote to Jacob, and his physician made the tests Jacob had required. On February 13, 1965, Jacob came to the Keinsleys’ home in Littleton and swabbed Grey’s neck with DMSO.
“The most dramatic change happened that first day,” Dorothy told me. “Grey had had a constant pain in his right shoulder from the time of the accident, and he had learned to live with it. Late that day, Grey discovered the pain had gone. He was almost incredulous. He expected the pain to return, but it never has.”
Other improvements were gradual, as Dr. Jacob had predicted they would be. One of the welcome changes was in his thermostat; until DMSO, it fluctuated between excessive heat and cold. His body temperature became normal.
Neurosurgeons and neurologists will say that there is some spontaneous return of function for the traumatic paraplegic — but only in the first two years following the injury. If significant improvement doesn’t occur within that time, it never will. There seemed to be no documented case to the contrary.
That principle is passé.
These are some of the battles as Dorothy recorded them, in Grey’s war:
•4/5/63 – The accident. Grey was expected to die. He lived in a respirator.
•2/5/64 – Leaves Craig Hospital and starts classes at the University of Colorado, Denver Center.
•2/13/65 – Starts DMSO treatments. Shoulder pain stops.
•5/1/65 – Temperature sensation stabilizes.
•6/1/65 – Healthy color replaces pallor. Grey feels fine and smells terrible (from DMSO). He is no longer constantly tired.
Return of major functions of the body:
•8/22/65 – Lifted both arms over his head and put on a T-shirt without help.
•9/12/65 – Pains in left hand and wrist. First since the accident.
•10/17/65 – Sensation to touch on right side of body starting to move below nipple line (2 to 23 inches).
•10/29/65 – Severe pains in right hip.
•11/1/65 – Sharp pains in upper left arm for several hours.
•11/9/65 – Severe pains in right hand and arm.
FDA banned use of DMSO.
Pains subsided in a few weeks, but he did not lose any of the improvements.
•11/6/67 – Stops wearing body brace (similar to a corset to support lower back).
•8/22/68 – Resumes DMSO.
•9/6/68 – Tingling sensation deep inside neck in area of lesion.
•10/9/68 – Feels heat in right hand from coffee cup — first time.
•11/16/68 – Moves right leg — feebly.
•12/11/68 – Exerts pressure shaking hands with right hand.
•12/31/68 – Sensation to touch on entire right side of body. It is spotty and not too clear.
•1/19/69 – Exerts very weak pressure with left hand.
•3/5/69 – Moves right thumb.
•4/1/69 – Raises right leg in bed.
•4/13/69 – Lifts his body slightly off the bed or wheelchair by using his arms locked at the elbows.
•6/6/69 – Grey receives his Bachelor of Arts degree in economics.
•6/17/69 – Moves toes on both feet — weakly (through 8/12/69).
•10/12/69 – Moves left leg — feebly.
•1/1/70 – He writes by hand legibly and at length.
•8/17/71 – Grey received his master’s degree and began looking for a job, preferably in a bank.
The chronology omits mention of the many people and organizations who lent help of various sorts: the Mayfield Foundation, which supplied a hydraulic hoist (so his mother could lift him into the family car) and an electric typewriter; cab drivers who gave him a lift; state transportation to and from school; and student grants for his tuition.
The people most responsible for Grey’s victory were his mother and his sister, Pamela. Pamela worked while attending school and helped her mother a great deal with household and nursing chores.
Mrs. Keinsley had to get up at five every morning and spend two hours preparing Grey for school. He required a catheter or condom to void, and even with the hydraulic lift, getting Grey into the car and into school was an arduous job. At first, Dorothy attended classes with him and took notes for him.
Grey supplemented the meager family income — from welfare, child support, and Pam’s babysitting jobs — by grading papers and tutoring students. This brought in twenty-five or thirty dollars a month. He dictated his comments and grades to his mother, who was necessarily his almost constant companion.
When Grey first proposed writing to Jacob, Dorothy hesitated. She was afraid that if Jacob rejected the idea, it would crush her son. She had earlier received three flat and emphatic medical opinions that her son would be completely helpless for the rest of his days. She asked Grey: Could he take it if Dr. Jacob was negative? They sent off the letter to Portland.
In insisting that her son would find help, Dorothy Keinsley did not delight all the doctors. “One doctor bellowed at me like a bull moose in rutting season,” she said. “’Don’t you know your son is paralyzed?’ he screamed. I explained that no one knew it as well as I.”
Mrs. Keinsley said that Jacob not only did not charge for his services, but, out of his own pocket, paid the bills for the exhaustive medical examinations, which were done locally. Jacob makes a house call at the Keinsleys’ whenever he is in Colorado.
When three years of supplication by himself and many others had brought no sign of relenting from the FDA, Jacob decided to resume treatments anyway. He told Grey he thought that injections into the back of the neck, in the vicinity of the scarred spinal cord, might speed up recovery. He asked if Grey was willing to accept the considerable pain of the injections and the increased odor from them. Grey agreed, but first he wanted to square it with others.
He talked with his professors at the university, saying he was willing to drop out of school to save other students from the aroma. One professor said, “Grey, I want you to attend classes as usual. If worse comes to worst, there will be two people present in your classes — you and I.”
The students, every single one of them, stuck with Grey, rooted for him, and helped him however they could.
“In the three years that DMSO was denied him,” Mrs. Keinsley said, “Grey did not progress, but neither did he lose any of the ground he had gained.”
“I wish I could tell you that Grey arose from his wheelchair under his own power. This is coming. We are working toward that goal not only for Grey but for all people who are paralyzed by spinal injuries.”
A specialist in orthopedic surgery and fractures has drawn up a series of exquisitely detailed reports on the nerve-by-nerve and muscle-by-muscle comeback of the patient. They probably are without parallel in medical annals.
Note: a 1971 Colorado news article and 2007 obituary corroborate many of the above events and showed that Grey lived a successful life which greatly exceeded the typical prognosis of quadraplegics.
When you consider stories like Grey’s (and many others, including some readers shared with me of DMSO reversing their paralysis) it should be clear there is a very high EV with DMSO for disabling spinal injuries (SCI) as:
•The risk and cost of DMSO are negligible.
•DMSO routinely gets partial recoveries and if done shortly after the injury (which would require it being in ambulances), complete recoveries.
•In contrast, SCI injuries are often permanent, and at best (but still fairly rarely) will have a small recovery of motor or sensory function in the months immediately following the injury.
•Despite decades of research, there is still no treatment for SCIs.
•The negative impact of a SCI is so severe on one’s life that most patients would deem even a small improvement to justify the immense cost and risk to them.1,2 Likewise, SCI patients often experience severe pain throughout their body (with a third reporting it severely affects their quality of life) which is quite difficult to treat, but as Stanley Jacob (and a few readers here) observed, their pain has an excellent response to DMSO.
Yet, despite that massive EV, and a lot of data supporting DMSO’s use for SCIs (which I complied in the article), virtually no one even knows this option exists. Furthermore, as I’ve shown in the DMSO series, this situation is not unique to SCIs (e.g., the first article in the series detailed how the same situation existed for strokes).
This hence raises an obvious question. How could this have happened?
Note: in that article I also focused on the far more common spinal disorders that cause widespread chronic pain and disability (e.g., low back pain and degenerative disc disease), and dramatic improvements to SCIs that allow afflicted individuals to get their lives back are also seen (which hundreds of readers here have reported).
DMSO’s Regulatory Journey
When DMSO was discovered, while initially skeptical a true wonder drug could exist, physicians were rapidly won over by the profound and rapid improvements they saw from it across a broad spectrum of illness, and before long, it became the most demanded drug in America. Unfortunately:
As Herschler now puts it, “If there is such a thing as a Murphy’s law of new drug development, DMSO proves it. Everything that could go wrong did go wrong.”
Briefly, after Dr Jacob discovering DMSO in 1961, the following occurred:
•The pharmaceutical industry was initially extremely interested in DMSO and many companies (including Merck) made huge investments in clinical trials for DMSO.
•The 1962 Thalidomide scare and the unanimous support for the FDA’s newfound regulatory powers.
•The FDA was initially receptive, but quickly realized they were being deluged with far more applications for DMSO uses than they had the staff to process (especially with their new far more robust standards). Notably, this actually came from the same person who was credited with stopping thalidomide.
•To get out of evaluating DMSO, the FDA seized upon two data points: a patient taking a large number of other drugs dying from an allergy while taking DMSO (which to this day remains one of the only deaths ever linked to DMSO) and data showing DMSO altered the focusing of eyes in dogs (but not monkeys or humans) to not only block all trials of DMSO but also through American embassies notify other countries that DMSO was the next thalidomide and would make you go blind.
Note: one of the most definitive human toxicity studies ever conducted (where prisoners had their entire body covered with multiple layers of DMSO each day for up to three months and then had every imaginable parameter tested) found DMSO, even extreme doses, had no toxicity. It was only after this study was conducted that the FDA finally pulled back some of its claims on DMSO’s toxicity.
•The pharmaceutical industry gradually pivoted from wanting to make money selling DMSO to wanting to keep it off the market because it competed with too many of their products.
•The new head of the FDA decided he wanted to expand the FDA’s policing powers as much as possible, so he decided to use DMSO as the test case for the FDA cracking down on unproven dangerous remedies so that he could empower the FDA.
Because of this, the FDA took a hardline position that DMSO was irredeemably bad, dismissing an immense body of scientific research supporting it (eventually pressuring scientists to stop the research) and ignoring widespread public protest by patients seeking access to it. Before long, the FDA identified a unique tactic to support this position—the fact that it was essentially impossible to do double blind trials with DMSO as:
•Patients experienced immediate and dramatic improvements that they knew came from an active therapeutic.
•DMSO has a characteristic odor that many trial participants experienced.
•DMSO was frequently irritating to the skin if applied.
•DMSO’s effects were systemic, so treating one part of the body would frequently improve untreated parts of the body.
So, each time the FDA leadership was confronted by news anchors, Congressmen, or Senators over DMSO, they insisted they were not stonewalling DMSO, and rather they were just waiting for “well-controlled trials” which could prove DMSO was actually effective, leading to frustrated Congressional testimonials like this:
If we have patients appear before the committee with sprained ankles, the application of DMSO would be followed by objective diminution of swelling within an hour. No other therapeutic modality will do this.
As such, the FDA only ultimately approved one use of DMSO (interstitial cystitis) in 1978, which I strongly suspect was done to head off Congressional criticisms that they were stonewalling DMSO. This is because, in 1980, at both a Senate and Congressional hearing on the FDA’s refusal to approve DMSO for anything, the agency insisted there was no agency prejudice against DMSO and that they would be happy to approve any reasonably conducted drug application sent to them—yet 46 years later, they still have not done so. Instead, DMSO was treated as a safe and inert additive which could be added to a variety of other pharmaceutical products that the FDA then approved (all of which are listed here), something the cynic in me believes occurred because this made it possible to bypass ever attributing a therapeutic benefit to DMSO and making it possible to patent and monetize each specific application which received a costly approval.
Conclusion
The estimated value framework is widely used in many fields (e.g., tests assessing one’s ability to quickly calculate EVs are used during the interview process by tech companies to identify competent candidates) and repeatedly cited in blogs I read written by younger physicians. However, I rarely, if ever, see it folded into broader discussions of medical decision making, something I cynically attribute to the fact that it would immediately displace many of the more harmful (but lucrative) medical practices on the market. Furthermore, I want to emphasize that while most of the ideas in this article are conclusions I arrived at from thinking about this mess, they are obvious enough that prominent figures within mainstream medical research have been raising them for decades — even the founder of evidence-based medicine has acknowledged that the framework was never meant to be reduced to "only RCTs count."
Note: somewhat analogously, I have long believed that if AI systems objectively evaluated all the EMR data we collect, many routine practices would be terminated as it would be clear their harm outweighed their benefit. However, the people I know who attempted to do this (it’s not very complicated), all ran into roadblocks due to the interests they threatened, and as such, systems like that have still not been implemented.
One of my key frustrations with the current paradigm is that we make a massive investment in costly (but low EV) research for drugs that ultimately often only show a minor benefit in one specific condition. Simultaneously, numerous therapies like DMSO which have much greater EVs (that patients suffering with “incurable” ailments can immediately see) not only languish in obscurity but often are attacked and suppressed to protect the status quo (while DMSO is probably the most blatant example of the FDA going to war against a therapy with broad public support, many other examples also exist such as all the off-patent COVID-19 treatments which were suppressed throughout the pandemic).
However, while this status quo has persisted for decades, it is now starting to shift, as the immense unchecked greed we all witnessed throughout COVID-19 (which polling shows the majority of the public has resentment towards) has not only shaken public trust in the pharmaceutical industry and its products (e.g., routine vaccinations), but also created a massive loss of trust in doctors, hospitals and the drug industry which eclipses anything in the medical system’s history (all of which I detailed here).
As that trust is vital to driving medical sales, there is at last, a real incentive to begin addressing some of the most egregious policies we’ve faced. Furthermore, if anything this trend is accelerating and politicians are noticing as more and more of them are beginning to publicly adopt MAHA’s language and positions.
This was best shown by the recent primary election in Louisiana where Republican Senator Bill Cassidy, the leading opponent of the MAHA agenda, not only lost his primary (which is extraordinarily rare—the last time this happened to an incumbent was in 2012 who was toppled by a Tea Party candidate), but Cassidy received less than a quarter (24.8%) of the vote—effectively ending his 20-year political career. Conversely, Senator Johnson, in his 2022 election (which from the start was a very close race), made the highly controversial decision to run for re-election on a vaccine-safety platform (making him the first Senator in history to do so), resulting in his opponents focusing on this to unseat him, yet (at a time when vaccine skepticism was much lower than it is now), he won the election because this stance energized his base far more than it alienated the rest of the electorate.
Likewise, much of the medical monopoly has only been possible because consumers had access to limited information and hence had to trust what medical authorities advised them to do. Now thanks to AI, it is quite easy for patients to have an in-depth understanding of the risks and benefits of a proposed treatment option, along with the other alternatives they can consider. While I do not believe AI can replace an experienced and creative physician, it can replace one who just follows protocols and guidelines, something which more and more has been the way doctors practice (as this ensures robust sales for the companies that effectively lobby to have their treatments put into the guidelines).
Given this shifting landscape, I’ve put a lot of thought into how this situation can be fully resolved. On one level, I believe it’s critical to expose the medical industry to real competition and provide people with the tools to actively calculate the EV of each option being proposed to them, as many of the harmful policies I routinely see are only able to perpetuate because of an information gap most customers face when they interface with the medical system. Likewise, most doctors in practice sincerely want to help their patients, and frequently get quite depressed by the fact they can only offer low EV options to their patients which provide minimal benefit (particularly if they have a corporate employer—which sadly regulations are making it harder and harder to escape from). For example, this is one of the thousands of DMSO correspondences I have received:
I appreciate all the articles you have been issuing on DMSO
It is really changing things for the better in my practice and your work has been the inspiration for it
Whether that is aches and pains, musculoskeletal disorders, arthritis, or cancer, I have been able to offer these patients something rather than sending them away
Offering viable alternatives is critical, as ultimately, the medical system only listens to money, and it is not until money is being lost that it will be willing to shift the standard of care to one which can compete with those options.
Separately, while I have strong disagreements with the policies the FDA has taken to enforce a state sanctioned monopoly over medical care (so that only those who pay to play can profit off the lucrative medical market), as the pre-FDA era shows us, regulatory action is needed, particularly since so much (finite) money is on the line once insurance begins to cover therapies. From the start, I have believed the greatest challenge the FDA faces is that it’s simply not possible to regulate most of the foods and drugs sold in the United States, and as such, they’ve had to selectively focus on a few manufacturers so that the worst things are prevented from harming the public and all other manufacturers, for fear of an enforcement action, are motivated to police themselves.
Unfortunately, since the FDA is vulnerable to lobbyists (who can either get the White House to fire agency staff or Congress to sanction the agency), this incentivizes the FDA to target their limited enforcement capabilities against smaller fish which lack the lobbying power to threaten the FDA and in many cases, go overboard in doing it so that a perception can be created for the public that the agency takes its duties to protect us very seriously (much in the same way we periodically see token regulatory actions taken against pharmaceutical manufacturers which do not threaten industry’s bottom line but almost never real action).
Given all of this, I believe the best regulatory policy going forward is as follows:
For therapies insurance covers, robust and costly approvals should be a prerequisite for coverage, but in instances where no viable therapeutic option exists, the “best available” alternative option (e.g., that which has shown promise but has less robust evidence behind it) should get at least partial coverage.
For “unproven” therapies which have been in use for decades, amassed a large body of supporting evidence, and failed to demonstrate harm (or at least shown less harm than their conventional alternatives), a parallel drug approval track needs to be created which fully permits the use of these therapies (and protects doctors from being penalized for using them) while avoiding the ensuing requirement for insurance reimbursement. This I believe is fully appropriate as that is effectively the exact same situation which already exists for virtually every drug being used in an off-label capacity, and as such, the only “fair” action regulators can do is to prevent sellers of the therapy from making claims which exceed the current approvals (or like supplements, only make mechanistic claims rather than stating it cures a disease).
For most therapies, the purpose of the FDA should be to ensure safety and quality control (e.g., no bad batches of the therapy being produced), as this is a vital function to perform, and as we saw with the COVID-19 vaccines, the failure of the FDA to perform this task has immense consequences for everyone. Likewise, in studying the history of the FDA, a strong case can be made that the legislative action which provided the single greatest benefit to the public was the 1994 DSHEA act which restricted the FDA’s regulation of natural supplements to safety rather than efficacy, limiting the FDA to blocking claims.
This is ultimately why I’ve put so much work into compiling the evidence for DMSO across this series—because if the system is set up so that compelling data will never be enough unless it comes in the form of a billion dollar RCT, the least I can do is make the data so overwhelming that anyone willing to actually look at the numbers can see the EV for themselves, and the “hard” decision of whether to try it becomes a remarkably easy one.
The great irony is that when you actually run the numbers, it's not the "unproven" therapies that lack evidence — often it's the approved ones and their costly trials that lack value.
A recently updated index of all articles published in the Forgotten Side of Medicine (including the DMSO ones) can be viewed here. Additionally, to learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here.
Somehow you manage to overcome the seemingly endless opposition to the finer points of healing. Bravo! The drive to uncover the truth as you see it and then backing it up with endless examples and data is testimony to your unstoppable optimism. Thank you for this incredible offering.
When the Pfizer clinical trial data were released I reviewed the findings and questioned them (I am not a statistician). I had questions that I asked of my PhD statistician friend and professor and got the same kind of response you got from medical colleagues. She drove 65 miles when the vax became available to get it.
As for DMSO, our vet uses it and said all the equine vets swear by it. He also did not get vaxxed nor did his family who listened to his advice. Sometimes vets are more knowledgeable than physicians.