The Century of Forgotten Vaccine Hot Lot Disasters
How the mantra of "safe and effective" has shielded countless compromised products from scrutiny and led to the same disasters continuously repeating.

•Producing a vaccine has many opportunities for error or contamination. Because of this, disasters continually occur from “hot vaccine lots” being unleashed onto the public. Remarkably, as the years have gone by, there has been less and less accountability for this (e.g., previously public investigations were held and people went to jail whereas now government tends to keep the hot lots on the market and deny there is a problem).
•In 1967, an eminent bacteriologist wrote a book detailing many forgotten vaccine disasters under the belief (he shared with many of his anonymous colleagues) that unless his profession was honest about the dangers of vaccination, the mistakes which led to those disasters would keep on repeating.
•Many of the disasters he detailed related to an excessively dangerous vaccine lot being released onto the market. Remarkably, many of the disasters he detailed mirrored what occurred in the decades that followed (e.g., this article discusses the documented DPT and anthrax hot lots which caused a tsunami of injuries in infants and veterans).
•One of the largest problems with the COVID-19 vaccines were the deadly hot lots that were released onto the market. In this article, I will cover everything we know about those lots and show their remarkable parallels to the century of hot lot disasters which preceded them.
During the COVID-19 rollout, patients gradually began to realize that some of the COVID-19 vaccines were more dangerous than others. Initially this was written off as a conspiracy theory. However, as time moved forward, and more evidence emerged to support the “hot lot” hypothesis there was an increasing acceptance of this theory.
At the time, the most common theory I heard raised to account for this was that a large global experiment was being done to assess the effects of various mRNA doses (e.g., one researcher was able to show that the hot lots of each COVID vaccine brand hit the market at different times in a manner that seemed to be coordinated between the manufacturers and that Pfizer’s lots contained a simple code that correlated to their toxicity).
However, while this was possible (as you can put nothing past these people) I was more inclined to an alternative hypothesis: that it was not possible to correctly produce the mRNA vaccines at scale, so there would be a large number of production issues including many either toxic or inactive lots hitting the market.
This theory was based on both my knowledge of the specific engineering challenges the mRNA technology faced and the fact that hot lots are an enduring problem with vaccines.
Because of this, many (myself included) believe the vaccine industry concluded it wasn’t possible to completely clean up their production process while maintaining the economic viability of the vaccines, so they instead focused on getting the Federal government to exempt them from liability for their hot lots under the argument that “vaccines were essential for our national security” so a certain number of people being injured by defective vaccines was an acceptable trade-off to maintain this “vital” national resource.
Given the severity of this allegation, I will now present several incidents where 'hot' vaccine lots have been identified in the market.
Adventitious Agents
One of the greatest challenges with producing a biological pharmaceutical is that it has to be grown in a medium (e.g., a virus within cells or a growth medium for bacteria). This introduces a few major issues.
•First, if cell cultures are used, an unrecognized virus may already have infected the cells and contaminated the final product.
•Second, anytime a growth medium is used, unwanted pathogens can also get in (e.g., from the air) and then grow there. This is especially problematic because the same labs that produce these products also often house harmful infectious organisms.
•The entire process inevitably requires a purification stage where the undesired contaminants (e.g., unwanted bacteria, foreign DNA, or toxic components of now destroyed bacteria) are removed. Unfortunately, it is often quite difficult or costly to remove these unwanted contaminants, and the cost frequently exceeds what the manufacturers are willing to pay.
In turn, unwanted biological contaminants (euphemistically termed adventitious agents) are an enduring challenge for the pharmaceutical industry. For example, this recent 2022 review paper highlighted some of the most common “adventitious agents” (e.g., mycoplasma frequently contaminate cultures) and cited a few well-known incidents such as:
•In 1946, a sheep vaccine was contaminated with prions (due to it being sourced from sheep in the early asymptomatic stage of the prion disease scrapie—something similar to Mad Cow Disease), which in turn caused the sheep in the herd that received the vaccine to later get scrapie.
•The FDA reported in 1973 that the MMR (measles, mumps, and rubella) vaccine and oral polio vaccine were contaminated with bacteriophages (viruses that eat bacteria). This was due to the blood used to make those vaccines containing bacteria, and the bacteria but not their attached bacteriophages being filtered out of the final product.
•In 1995, the MMR and yellow fever vaccines were found to be contaminated with the Endogenous Avian Retrovirus and the Avian Leukosis Virus.
•In 1997, scrapie was also spread to sheep through another contaminated vaccine.
•In 2004 and 2005, two rotavirus vaccines, Rotarix manufactured by GlaxoSmithKline (GSK) and RotaTeq manufactured by Merck, were found to be contaminated with porcine circovirus-1 (PCV1) after over 100 million doses of the vaccine had been distributed worldwide.
•In 2007, over 1 million doses of the Haemophilus influenzae type b (Hib) vaccine were recalled due to the detection of Bacillus cereus in the manufacturing equipment.
Sadly, as we investigate the past, it will become clear these events were only the tip of the iceberg.
Note: many reported incidents that I am not aware of didn’t make it to this article, while a far larger number of incidents were never reported, but I nonetheless believe the cases listed in this article are more than sufficient to make the point. Similarly, as a I discussed in a previous article, while lab leaks with dangerous pathogens are typically not reported, enough documented instances exist within the peer reviewed literature to establish that those leaks are inevitable and impossible to avoid (which in turn argues that this research ever being conducted).
Sir Graham Wilson
Sir Graham Wilson was an eminent bacteriologist from the London School of Hygiene (e.g., in 1923 he coined the concept of herd immunity—an often impossible benchmark that I’ve previously shown has been used to repeatedly sell dubious vaccines to the world). Wilson grew up in a time when many bacterial infections were treated with vaccines or antiserums (particularly antitoxins for the tetanus or diphtheria toxin). At this time, his profession believed anti-vaxxers were irrational and pseudoscientific individuals and that vaccines were “100% safe and effective.”
However, as Wilson became older, he began to see more and more evidence that there were real dangers to vaccination, and that his profession habitually covered it up to maintain the mythology all vaccines were “safe and effective.” In turn, due to Wilson’s stature in the field, many other (anonymous) vaccine experts shared their records of secret vaccine disasters that had occurred with Wilson and helped him to compile a detailed record of published and unpublished vaccine catastrophes that had occurred as many of them harbored immense guilt over what had happened, but simultaneously felt that they could not take on the risk of speaking publicly about it.
From reviewing the record he put together, what I find remarkable about Wilson’s work was how much of it mirrors what we saw a century later—for example, very few people know that one of the original cases of Guillain Barré syndrome was due to a vaccine injury:
In an article published in 1919 Guillain and Barré referred to Landry's–type paralysis when they reported a fatal case of acute polyneuritis with albuminocytologic dissociation after typhoid vaccination.
In Guillain and Barré's case numbness and stiffness became apparent in the patient's legs the day after injection and the following day in his hands. Paralysis gradually came on and by the 9th day was complete in the legs, arms, and face. Bulbar symptoms developed on the 7th day, and on the 10th day, the patient died.
Note: previously I discussed many of the documented cases Wilson unearthed of a vaccination causing a pre-existing illness (e.g., polio) to spiral out of control.
One of the key themes that kept on recurring in the records Wilson unearthed was that many vaccine catastrophes occurred after a contaminated lot was given to a large number of people (typically children or soldiers). Wilson in turn argued that rather than denying these incidents occurred, his profession needed to be honest about them so that the mistakes that led to these toxic 'hot' lots could be recognized and hence prevented from happening again. In The Hazards of Immunization, he discussed the following hot lot incidents:
I will now review those incidents in detail.
Note: Wilson documented many severe reactions that occurred from the early vaccinations. In this article, I am only covering the subset of reactions which occurred at a higher rate than the typical rate.
Hot Lots of the Past
Note: I tried to find all the sources Wilson cited (his citations were not that clear). For those not cited, please refer to his 1967 book. Additionally, to view any of the abstracts on cabidigitallibrary.org without having to pay for them, you must access them through Google Scholar (by searching for the URL there). Additionally, some of the incidents listed here we not covered by Wilson, and for all of those, direct sources are provided. Lastly, many of the deaths described here were agonizing and horrific, but for brevity, I have not detailed each of them.
Diphtheria
Early diphtheria vaccines utilized the diphtheria toxin to provoke an immune response to it. Since it was so difficult to neutralize its toxicity, numerous accidents occurred due to hot lots being released with an active diphtheria toxin which had a variety of characteristic symptoms (many of which overlapped with other vaccine injuries). For example:
Disturbances of sensibility were sometimes detectable, especially in the older children. They included paraesthesia, formication in the extremities, and diminution in the muscular sense and the orientation of the limbs leading to ataxia. The patellar reflex was first exaggerated, then lost, and regained as recovery took place. One of the earliest symptoms was an exaggeration of the oculocardiac reflex; in several hundred patients it was observed that compression of the eyeball led to stoppage of the heart.
Note: the oculocardiac reflex is now a mostly a forgotten side of medicine (outside of very specific areas of medicine such as surgeries on the eyes). The diagnosis of this reflex is defined by the heart rate decreasing by over 20% after pressure is placed on the eyes (which typically does not happen) due to activation of the vagus nerve. I have a few theories on why vaccine injuries would cause that reflex to stop the heart, but I am not confident in any of them.
Let’s now look at a few of the cases of diphtheria hot lots:
•In October 1919 the city of Dallas Texas began administering the diphtheria toxin (and its antitoxin) to non-immune children. Many different lots were used, and one of those ended up being hot (due to it having over 50 times the maximum permissible levels of free diphtheria toxin). Several hundred doses of it were given (although the exact number remains unknown), and 50 severe reactions to it were reported (with many more not being reported). When 120 of those injected were studied, it was found that 96 had reactions, 12 of which were moderate, 74 which were severe, and 10 of which were fatal.
Each of the 96 Dallas cases in turn had an almost identical progression of symptoms. Their symptoms went in the following order:
1. Intense burning at the site of injection which in a few hours became agonizing.
2. This was accompanied by severe nausea, vomiting, constipation, signs of a kidney injury, extreme swelling of the entire arm, and a reaction that spread into the rest of the body.
3. 24-48 hours after injections, vesicles appeared at the injection site, which leaked a burning fluid, and after they disappeared, left a raw ragged and ill-smelling patch 6-12 square inches (or more) in area which took around 2 to 2.5 months to heal.
4. Around 9-10 days, the heart became highly irregular and this lasted until the 8th to 10th week.
5. Starting at the third week, all the patients had muscles throughout the body become paralyzed (including the ones which controlled neurological functions like vision). Typically, these neurological complications lasted for 18-20 weeks, and tended to be more severe in those who had had a less severe initial reaction to the vaccine.
Remarkably, no investigation over what went wrong in Dallas was ever conducted, so other similar incidents also occurred.
Note: aspects of the incident are discussed within this 1927 book.
•In 1922 a 14-year old in Belgium was injected with a vial of diphtheria toxin (receiving at least 100 times the lethal dose) that had somehow gotten into a batch of tetanus vaccines, and died seven days later from cardiac paralysis.
•In Massachusetts in 1924, two lots were given that became toxic due to being frozen. For one lot, 21 of the 23 who received it, had severe reactions to the vaccine (but none died), while for the other lot, 22 of the 31 had severe reactions. After these incidents were studied, it was concluded that the cold had separated the antitoxin from caused it to agglomerate (clump) together on the bottom of the vial.
Note: colloidal agglomeration and zeta potential are discussed further here (as one of the primary toxicities of vaccines is that they cause fluids in the body like the blood to clump together and stop flowing).
•In Baden in 1924, 34 infants and children received a hot lot, of whom, 6 had no reaction, 11 had mild reactions, and 17 had severe reactions (of which 10 were fatal). A subsequent investigation revealed that when this lot was produced, diphtheria toxin was accidentally mixed with another diphtheria toxin rather than an antitoxin.
•In Tashkent (U.S.S.R.) in 1927, 14 children received diphtheria toxin instead of antitoxin, 8 of whom died. In their case, administering the antitoxin, appeared to prevent their immediate death and instead caused them to die from a progressive paralytic neurological disorder.
•In 1928 in Queensland, 21 children were injected with a diphtheria toxin-antitoxin mixture of whom 12 died. Unlike the other cases, this one appears to have been due to the vaccine being contaminated with Staph Aureus.
•In Columbia in 1930, 48 children were given toxin instead of antitoxin, many became severely ill (often becoming comatose or convulsive) and 16 of them (with 14 dying in 1-3 days and the others dying from progressive neurological symptoms). One noteworthy aspect of this incident was that many of the children developed the characteristic diphtheria membrane in the throat (which gradually suffocates you), suggesting that the toxin itself had an affinity for the throat (rather than just the infection) as no diphtheria bacteria could be found.
•In Italy, in 1933, several hundred infants and children became severely ill after being injected with a hot diphtheria lot, with over 30 dying.
Note: in most of these cases, autopsies also showed damage to organs throughout the body.
Once a safer way to produce the vaccine was discovered (using a toxoid rather than a toxin), production was shifted to the new method. However, incidents still happened with these newer vaccines. For example, in 1948 in Kyoto Japan, over 600 infants and children became ill from one lot, with at least 68 dying (along with 16 more deaths in Shimane). In one sample of 15,561 who received their second injection, 606 fell ill, and 68 died from muscular paralysis (with 59 dying in 1-2 weeks), and it was later discovered these hot lots again contained the free diphtheria toxin.
Given that children were regularly dying from diphtheria, I can understand why governments around the world believed any treatment for it was justified. Nonetheless, given that in each of these cases, the diphtheria toxin maintained a remarkably consistent lethal dose (roughly one-millionth of a gram) they should have done more to ensure that quality control was in place to prevent these agonizing deaths from happening. Sadly, as we’ve seen since then, that lesson still has not been learned.
Note: there was also a 1926 case in China where 33 of 89 people who received a diphtheria toxin antitoxin injection became ill (with 5 dying), from what appeared to be streptococci contamination. Subsequent investigation revealed that the source of this contamination was likely the distilled water used to dilute it.
Tetanus
There were also cases where a hot lot was created from a failure to inactivate the tetanus toxoid and it caused numerous cases of tetanus, particularly in Central Europe. Likewise, there have also been numerous cases where a different vaccine sickened many because it was contaminated with tetanus bacteria. For instance:
•In a well-known 1901 incident, a horse was used to produce diphtheria antitoxin that naturally developed tetanus during this period, then had its blood drawn (for the diphtheria antitoxin), at which point, while the horse was not yet symptomatic, it had significant amounts of tetanus in its blood. Human error then resulted in the blood not being discarded nor it being tested prior to human administration, and 20 children in St. Louis who received it became ill with tetanus, of whom 13 died.
Note: this incident along with another incident that occurred the same year from a smallpox vaccine contaminated with tetanus that killed 9 children led to the 1902 Biologics Control Act, an act which gave the government the authority to decide which biological products could be sold. This led to 30% of the companies making vaccines or serums going out of business and eventually led to the creation of the FDA in 1938.
•In 1900 in Italy, a privately manufactured diphtheria antiserum became contaminated with tetanus bacteria. At least 18 children who received that injection developed tetanus and of them, 13 died. A subsequent investigation discovered other bacteria also had contaminated the serum. Wilson in turn concluded this incident was likely due to contamination from the cork sealing serum’s container and insufficient phenol being used to sterilize it.
•In 1902, an American author compiled 52 cases around the world occurring between 1839 to 1901 where someone developed tetanus from a contaminated smallpox vaccine. Typically, this took 2-4 weeks to happen and resulted in the deaths of 41 (78.8%) of them. The same year, another author also discovered 95 documented cases of this happening between 1854 to 1902, of which 61 died, 24 recovered, and the fates of 10 were unknown. Of note, many of those cases occurred in New Jersey and Philadelphia in the autumn of 1901 and 75% of those vaccines came from the same manufacturer.
Note: Wilson was not able to determine which cases were counted by both authors.
•Since 1902, Wilson was only able to identify 41 reports of tetanus being caused by a contaminated smallpox vaccine, which he took as a sign physicians had become more reluctant to report this happening.
Note: in 1998, a mass diphtheria tetanus vaccination campaign was conducted in Jordan’s schools. In September of that year, slightly under 20,000 children were vaccinated and 800 reported side effects including 122 being admitted to the hospital for symptoms such as fainting, nausea, fever, and headaches. While a hot lot was likely responsible for this, the WHO and the Jordanian Ministry of Health instead concluded it was due to “vaccine anxiety” and a “mass psychogenic illness.”
Polio
Most of the early polio vaccines were made by exposing the polio virus to formaldehyde so it would become inactivated and no longer dangerous. Unfortunately, it was somewhat difficult to provide enough formaldehyde to completely inactivate the virus without also causing enough to damage to the virus that it no longer could produce the desired immune response. As such, numerous incidents occurred where people were injected with “inactivated” vaccines that erroneously had viable polioviruses.
For example, one early “inactivated” vaccine was tested on approximately 9000 people in 1935, with 12 developing polio (6 of which were fatal), and following the advice of an outside expert, this early vaccine was canceled by the government.
Note: Wilson pointed out that there was a logical explanation for why the 1935 vaccine’s Polio virus was not inactivated. Unfortunately, while this was detailed in the medical literature, it was only after the 1955 debacle that the problem became recognized and addressed. Tragically, despite manufacturing processes, cases continued (e.g., there was a 1958 incident and I likewise know two people who got polio from a polio vaccine).
Likewise, in 1955, a new inactivated polio vaccine (Salk’s) was unleashed on America despite warnings from the government scientists who tested it that it was not safe to be deployed. The vaccine was produced by 5 manufacturers, with two having hot lots (most of which came from Cutter Labs and some of which came from Wyeth). Ultimately, at least 220,000 people were infected with the live polio virus in Cutter's vaccine (including 100,000 contacts of immunized children) 70,000 developed muscle weakness, 164 were severely paralyzed, and 10 died.
Note: the exact number of polio cases varies depending on the source.
The Cutter incident was one of the most notorious vaccine safety accidents and ultimately led to the polio vaccine program being paused and numerous resignations in the US government. Many lawsuits also followed against the manufacturers. Sadly, in the most important one, the jury found that Cutter was not negligent in producing the vaccine (since the other manufacturers had also had difficulty inactivating the polio virus), but rather that Cutter had breached an implied warranty that their product was safe—in essence creating the concept of liability without fault, which completely changed the legal landscape and essentially making it impossible to prevent pharmaceutical companies from releasing toxic lots onto the market.
Later, live (attenuated) polio vaccines were developed which also had issues. For example, in 1960, 280,000 children in West Berlin received one, and 48 children developed polio (25 of which occurred within a month of vaccination).
Note: this vaccine was eventually discontinued in America in the late 1990s, but like the original DPT vaccine, remains in use throughout the poorer nations.
Presently, the majority of cases of polio-like paralysis around the world (including high-profile ones that are used to argue for more vaccination) result from the live polio vaccine (or its shedding) rather than from the wild polio virus. In one of the most tragic cases where Bill Gates and his Foundation diverted India’s public health budget to initiate a mass live polio vaccination campaign for India’s children (often giving each child as many as 50 doses of the vaccine), it was estimated that his program caused 491,000 children to become paralyzed with a “polio-like” illness.
Note: another major issue with the polio vaccines was their contamination with the SV40 virus (which Wilson noted was an extremely difficult contaminant to remove). The “official” story with SV40 is that while the virus was carcinogenic, no increase in cancer ultimately resulted from these contaminated lots being given widely to the public. Physicians who were in practice at the time however felt differently, and my colleagues who use holistic cancer treatments in the present also believe it is a real issue. Additionally, the SV40 virus was found to have contaminated adenovirus vaccines given to the military, while another cancer causing virus the avian leukosis virus, in 1962 was discovered to have contaminated the yellow fever vaccine supply.
Yellow Fever
Since the yellow fever vaccine is also a live attenuated virus, it had the inevitable risk of creating a severe illness in vaccine recipients and unfortunately was quite challenging to sufficiently attenuate while simultaneously making it produce a sufficient immune response (e.g., one version was produced by passing a yellow fever virus that been adapted to mice through mouse brains between 256 to 258 times).
Note: there was also a real risk that other mouse viruses could contaminate these preparations. Additionally, one researcher who tested cases of fatal encephalitis following yellow fever vaccination was able to confirm that the patients had the yellow fever virus within their brains.
As early as 1936, Wilson identified cases of encephalopathy, which began with a severe reaction, progressed to a loss of neurological function and in some cases was eventually fatal. In one review of 102,000 people vaccinated for smallpox and yellow fever in Africa, it was determined that 18 fatal cases of encephalitis occurred, and in another sample of 142,000 who were vaccinated, 32 died. Additionally, there was also a case where an unknown number of Costa Rican children received the yellow fever vaccine, 12 developed encephalitis and 3 died.
In Brazil after 55,073 who were vaccinated for Yellow Fever, 199 (0.36%) developed encephalitis. In a subsequent campaign, 2,973 received the old vaccine, of whom 49 (1.65%) developed encephalitis, while 9,870 received a new one and only 6 (0.06%) developed encephalitis. This again suggests the presence of a hot lot.
Note: Wilson cited examples with other live viral vaccines which illustrate that humans are often more susceptible to becoming severely ill than animals, which again illustrates how hard it is to effectively test this technology.
Between 1933-1937, two authors tracked 2200 yellow fever immunizations. Of those, 48 developed symptoms of hepatitis (e.g., jaundice) 2-7 months after vaccination that were likely due to the injection. As yellow fever was not known for causing hepatitis, those authors concluded another contaminant was present that did so (e.g., a virus that was resistant to the sterilizing agents they were using). In a followup report the next year, they found that out of 3100 immunizations, 89 cases of hepatitis occurred. Finally, the next year, they concluded the contaminant causing hepatitis was a virus present within the human bloodstream.
Between 1935-1937 in Brazil, a yellow fever vaccine made from two pools of hyper immunized monkeys was observed to cause 20-30% of those injected with it to develop a non-severe form of hepatitis, but simultaneously it did not affect any of the 620 Brazilians who received another vaccine.
A 1942 report discussed a yellow fever vaccine lot in South America that caused 1,260 cases of jaundice and one death among 107,000 people who were vaccinated with subsequently incriminated lots, of whom 1,072 developed jaundice and 24 died. According to Wilson, 82 of the 304 (27%) who received one lot developed jaundice, while in another area, 8 out of 40 (20%) were affected, and in another area, 6 out of 916 (only 0.65%) were affected. The following year, three more “hot lots emerged,” with one given to 9604 people causing 736 cases of jaundice (7.7%) and 19 deaths, and another given to 9587 people causing 150 cases of jaundice (1.6%) and 3 deaths. In contrast, one lot given to 620 people did not cause a case of jaundice, again illustrating there was a massive variation in the toxicity of the lots. Finally in all these cases, jaundice typically developed 12 to 20 weeks after vaccination.
•Wilson also discussed a 1942 press conference in Washington on 24 July 1942 where America’s Secretary of War reported that 28,585 cases of jaundice had been observed in the Army between 1 January and 4 July after yellow fever vaccination, and of these 62 had proved fatal. No statement was made on the number of men inoculated, but Wilson suspected it was probably between 2 to 2.5 million men. Finally, the Army concluded that the issue was likely something in human serum used to stabilize the vaccine, as once they stopped using human serum, cases of hepatitis stopped occurring after vaccination.
•In 1942, a yellow fever vaccine lot (containing pooled human serum) was given to 11,358 people in the Virgin Islands, 500 of whom then developed jaundice 75-130 days later. After testing the lot, it was determined that the jaundicing agent only affected humans (not animals), and that heat did not eliminate it, but ultraviolet light did.
Note: ultraviolet light is highly effective at inactivating viruses.
Finally, in 1943, it was shown that the jaundice disease could be transferred by taking nasal washings from someone who had developed jaundice from the yellow fever vaccine and putting it in the noses of previously healthy volunteers.
Note: fears of human serum transmitting hepatitis led to a search for a yellow fever vaccine that could function without being mixed with human serum. Once one was discovered and human serum stopped being used in the yellow fever vaccine, cases of hepatitis following yellow fever vaccination disappeared as well.
Rabies
Wilson cited 41 cases of rabies or encephalitis (or both) in the published literature which resulted from the rabies virus not being inactivated prior to injection.
Wilson also identified a hot lot (which resulted from the manufacturer not properly testing it before releasing it) that was deployed in Brazil. Following its deployment, at least 18 of the 66 vaccinated developed a fatal encephalomyelitis described as follows:
Symptoms came on 4-13 days after the beginning of treatment, and the illness proved fatal in 2-9 days, usually 5 days. It was characterized by general malaise, myalgia, pain in the neck, continuous high fever, intense headache, muscular spasms, convulsions, dysphagia, diplopia, and frequent projectile vomiting, followed by paralyses, intense dyspnoea, abundant salivation, urinary incontinence, torpor, coma and death.
Wilson also cited a case of someone who died from tuberculous meningitis after vaccination where upon autopsy it was shown the vaccine rabies virus was found in their brain and a case in Warsaw in 1901, where 22 out of 40 patients vaccinated for Rabies in one day in 1901 suffered from general streptococcal infection and four died (indicating the vaccine was contaminated with streptococcus).
Note: Wilson also discussed the vaccine for the Venezuelan equine encephalitis virus, which when tested on 327 persons (who received a total of 1174 injections), 14 became fairly ill with the disease 3-6 after vaccination (and in 7 out of 8 cases the virus was recovered from their blood). He cited this case to again illustrate that the virus could not be consistently inactivated and to show that humans were sometimes more susceptible to the virus than the animals being inoculated).
Tuberculosis
The tuberculosis (BCG) vaccine is cultured from an attenuated (weakened) form of the bacteria. In 1929, a BCG vaccine was created which accidentally contained the actual tuberculosis bacteria it in. Over the next year, 251 infants received it, of whom 72 died from tuberculosis, 135 became ill with tuberculosis but lived, and 44 developed immunity without symptoms. Many of these children developed severe lesions throughout their gastrointestinal tract and internal organs, something rarely seen in natural tuberculosis. Conversely, none of the 161 unvaccinated infants had any issues.
Unlike each of the other disasters, this one went to trial and four people were charged. There it was discovered gross negligence had repeatedly occurred and that this negligence led to the incident. Eventually, one defendant was sentenced to 22 months imprisonment, another to 15 months, while the other two were let off. This widely publicized trial appeared to have been a wake up call for the industry, and to Wilson’s knowledge, no contaminated BCG vaccines had since been produced. This in turn I believe highlights why it is so problematic the vaccination program now enjoys complete immunity from the law.
Note: at the trial, the court was also told that a similar incident had occurred in Pernik, Bulgaria where 75 out of 280 children had died after vaccination and 111 had become seriously ill.
There were also cases of other injections being contaminated with tuberculosis. In 1922-23, 25 children received convalescent serum from three children who had recovered from measles. Three of those children then developed minor cases of tuberculosis.
Typhoid Vaccine
In 1916, in Columbia, South Carolina, 322 people received a typhoid vaccine contaminated with Staph aureus. 68 had a severe reaction, and 26 developed local abscesses. Of the 37 under the age of five who received it, 4 died. Based on the record of this incident, Wilson suspected contamination had occurred when the vaccine was being filled.
Bubonic Plague Vaccine
In India in 1902, 19 people who received a plague vaccine contracted tetanus 5-6 days later, and all died shortly after. A commission was set up to investigate the catastrophe where it was discovered numerous small errors and untrained staff had caused hot lots to be produced. The director of the laboratory in turn “admitted that the staff were largely untrained and that a certain amount of contamination of the vaccine was inevitable,” but also noted that many of his practices were being used across the world.
Note: another author, in 1965, argued that the contamination that occurred here probably resulted from the lowering of standards caused by the increasing demand to produce more vaccines.
Cholera Vaccine
In 1906, 24 Philippine prison inmates were injected (without their consent) with an experimental cholera vaccine designed by the government that was accidentally contaminated with bubonic plague, leading to 13 of the men dying. The US Senate requested an investigation of it (that never reached America). Once investigated it was discovered bacterial incubators erroneously were left unlocked and a visiting physician had likely accidentally switched the cholera and plague cultures in the lab. Nonetheless, the responsible scientist was exonerated and went on to have a noteworthy career in American tropical medicine.
Measles Vaccines and Antiserums
•In 1938, 7 children in a mental institution were each given 4.5 ml of commercial measles serum obtained from a reputable commercial firm. Within 78—83 days all children became jaundiced and severely ill. Three of them died of acute atrophy of the liver.
•England’s Ministry of Health in their annual report described a similar incident that happened the year before in 1937 where 109 persons were injected with 'convalescent' measles serum from the same batch, with 41 contracting jaundice 16-114 days later and 8 dying (with those often dying having a coffee-ground vomit and extreme physical restlessness).
Note: additional details for this incident were provided in the Ministry’s 1943 report.
Another incident occurred later after the injection of serum belonging to two small batches, but no details were given.
•In 1951, 10 people received a prophylactic measles antiserum, with 7 of the 10 experiencing a severe attack of hepatitis 57-64 days after injection and 3 of those 7 dying (one of whom had encephalitis without jaundice). It was then determined that 6 of the 60 donors (for the antiserum) had a previous history of jaundice but it was never determined if any of them still had the hepatitis virus.
In 1961, three experimental measles vaccines were tested on 56 mentally disabled children living in institutions. Many reactions occurred:
•1 child “coincidentally” died of pneumonia 8 days after vaccination (which followed a severe exacerbation of a pre-existing seizure disorder due to the vaccine).
•9 had marked reactions (6 had an illness similar to natural measles, one of which was associated with bronchopneumonia, 1 appeared toxic with photophobia immediately before the onset of the rash, 1 had bronchitis, and the remaining child had tonsillitis).
•22 had moderate reactions and were sufficiently unwell in most cases that they needed to be confined to bed for two days.
•37 had high fevers.
•48 suffered from a morbilliform rash (a rash classically seen in measles).
The investigators in turn conceded that the trial yielded positive results, but suggested “that further attenuation of the measles virus is desirable,” in effect admitting the children were given a hot lot due to insufficient attenuation of the vaccine virus.
Note: due to the emotional magnitude of these events, the English Parliament later investigated the trial.
Other Vaccines and Antiserums
Wilson discussed a 1922 case at a Vienna hospital where 25 children were injected prophylactically with a batch of convalescent measles serum drawn from three von Pirquet positive subjects (a way of testing for an active or previous tuberculosis infection). Two to three months later 3 of the children suffered from a swelling at the site of injection and of the inguinal glands, became tuberculin positive (meaning they’d had a tuberculosis exposure) and 2 of the 3 had ulcerations at the injection site.
In 1944, two lots (A and B) of convalescent mumps serums were given to British army recruits. Lot A was given to 266 soldiers, and two weeks later, 204 of those soldiers also received Lot B. Hepatitis developed 59-94 days later in 44.7% of the 226 men who were subsequently evaluated, with those who developed hepatitis including 17 soldiers who had only received lot A, suggesting that A was contaminated with a hepatitis virus .
There was a case where 11 children were injected with Staph Aureus contaminated tuberculin, 1 of whom died and the other developed similar symptoms but recovered.
Additonally, a strong case can also be made that HIV emerged through contaminated vaccines given in Africa, Haiti, and New York (the London Times even wrote an article about it) due to both the Polio and hepatitis B vaccines being grown from contaminated monkey blood and kidneys.
Contaminated Administrations
Another common issue was the vaccines being administered in a non-sterile way which allowed the transmission of other diseases with vaccination (which was a problem since the vaccines were injected into the body and hence bypassed the natural defenses of immunity). The smallpox vaccine in turn was the most notorious in this regard. For example, to quote Dissolving Illusions:
Because using pox material directly from cows was initially disagreeable to people, Jenner developed a “humanized cowpox vaccine.” This method first utilized disease material from an animal, inoculating the raw pus into humans. The vaccination procedure then consisted of rubbing pox pustular lymph from the pock of an inoculated human to a cut in the arm of the next human recipient and was termed “arm-to-arm vaccination.” Another method of inoculation was to place numerous human-pox scabs into a jar, fill it with water, and shake. The resultant pus was used as vaccine material for one town.”
Often multiple sites were used in an attempt to try and ensure maximum protection. Successful vaccination was thought to have occurred by a “good take” after wounding up to four parts of the arm at one sitting. This practice of vaccinating more than one site continued in various parts of the world until 1975.
Obviously, many other diseases from the vaccinated were spread by this route, but arm-to-arm vaccination was used for about 100 years, until it was outlawed in 1898.
Dr. Beddow Bayly’s 1952 statements should leave everyone wondering how such a vaccine could have possibly been responsible for the eradication of any disease:
“When we recall that vaccine lymph is derived, in the first place, either from a smallpox corpse, the ulcerated udder of a cow, or the running sores of a sick horse’s heels, the choice depending upon the country of its origin and the firm which manufactures it, it is hardly to be wondered at that it has far-reaching ill effects on the human constitution. Years ago, the Lancet declared that “no practitioner knows whether the lymph he employs is derived from smallpox, rabbit-pox, ass-pox, or mule-pox.” Our own Ministry of Health has long confessed to complete ignorance of the ultimate source of its own supply of lymph; but last year Dr. A. Downie stated in the British Medical Journal that “the strain of vaccinia virus used for the routine preparation of lymph in this country [England] is believed to have been derived from a case of small-pox in Cologne during the last century.” That, of course, disposes of the whole theory of cow-pox vaccination.”
In turn, many cases of disease transmission from the smallpox vaccine occurred. For example:
•In 1861 no fewer than 46 children and 20 nurses were infected with syphilis after receiving smallpox vaccines obtained from a donor who had syphilis.
•In 1883, somewhere between 1200-1500 German shipyard workers were vaccinated for smallpox, and depending on the container their vaccine came from, between 5% to 26% developed jaundice (141 out of 540, 35 out of 466, and 14 out of 283). Conversely, none of the roughly 600 men who were vaccinated from another source developed signs of hepatitis (e.g., jaundice).
Note: at this time, the smallpox vaccine was sourced from the arms of children in orphanages (who typically were born out of wedlock and not wanted by the parents). One of the major issues at the time were the high rates of diseases in these children such as syphilis (discussed further here). Because of this (and other similar risky routes of disease transmission), in the late 1800s, nations gradually began outlawing sourcing the smallpox vaccine from other human beings.
Likewise, once a newer smallpox vaccine was developed, it still had the typical contamination issues. For example, in 1932 around 112,000 people in Malmö Sweden were vaccinated with a smallpox vaccine that was contaminated with Staph aureus, many of whom (either hundreds or thousands) developed significant complications from that bacterial contamination.
Unsterile Needles
There were also cases of people becoming sickened by what was likely a contaminated needle (as only a small subset of those who received the same lot were affected). For example:
•In 1932, 172 children in Bourbon Lancy received a diphtheria antitoxin. The next day, eight became ill (high fever, headache, vomiting at the site of injection), and one died.
•In 1935, 12 nurses (out of 106 vaccinated over 3 days) became acutely ill and developed bacterial abscesses that contained Streptococcus pyogenes which was traced to a strep-infected nurse who washed out some the syringes in a bowl of saline water (as she had contaminated the water by breathing into it).
•In 1936, 38 children received a diphtheria vaccine. 24 then developed tuberculosis and 1 died. A criminal trial eventually concluded this was due to inadequately sterilized needles.
•In 1938, 2408 children in Holbaek received a diphtheria vaccine, and within 8-12 hours 34 (who were all injected at the same time) became ill, with 21 developing scarlet fever (a severe Streptococcus pyogenes infection). The outbreak was eventually traced to an infected nurse who had handled the instruments at the school where this occurred.
In another 1938 incident, 12 of 29 children who were injected with diphtheria toxoid became ill with streptococci infections that were ultimately traced to contaminated cotton-wool which contacted both the needles and injection sites (with one of those children dying from the infection).
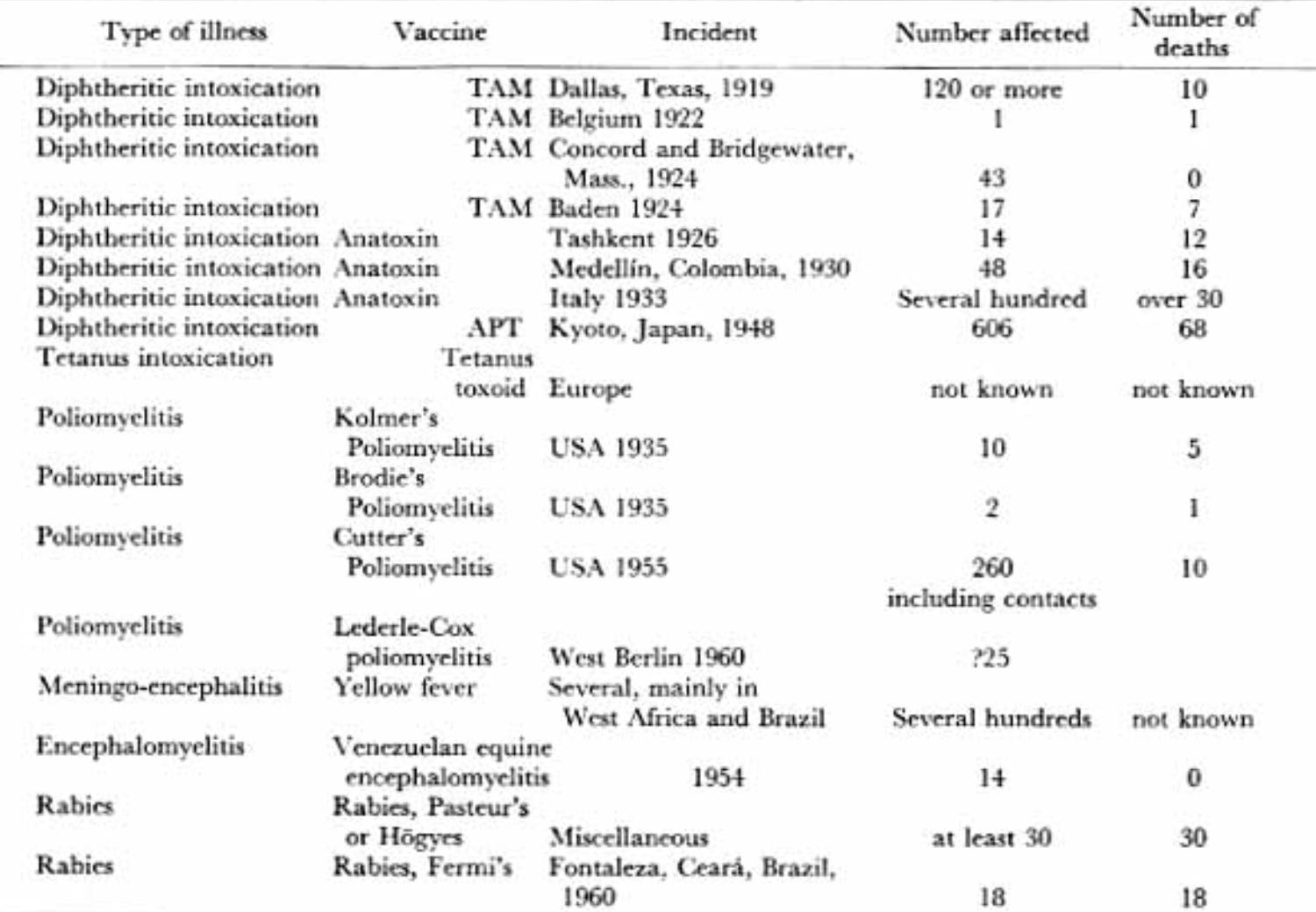
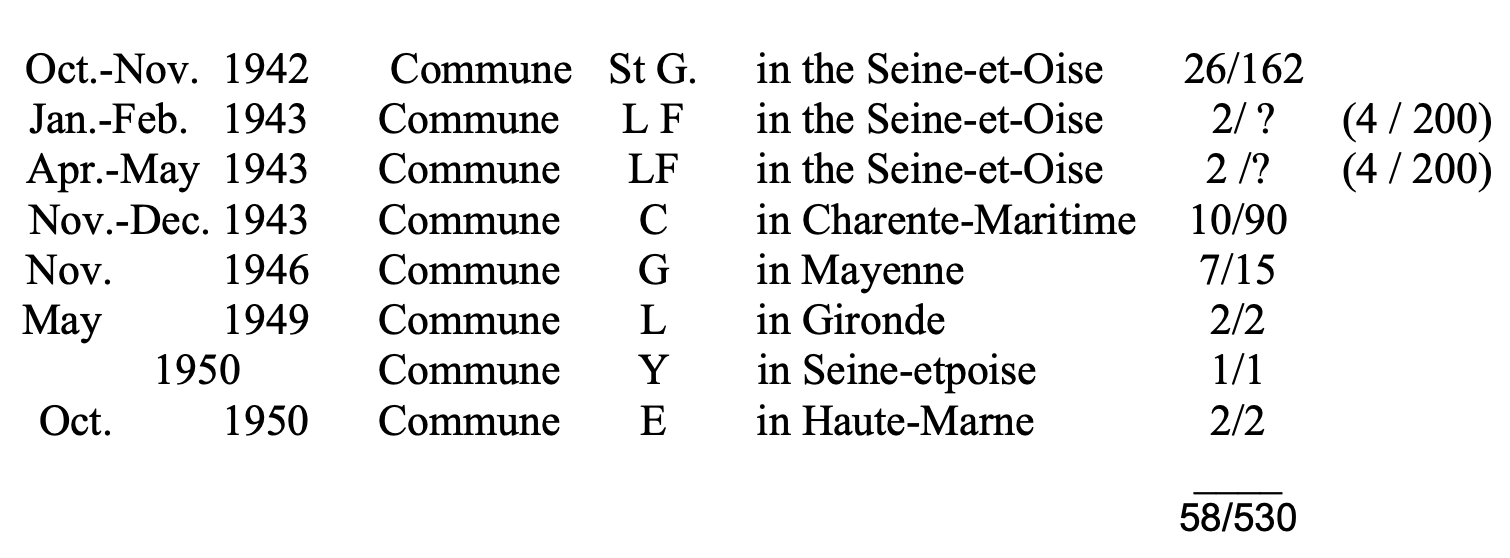
•A group of researchers in 1951 identified 95 cases in the French literature between 1942-1950 of someone getting tuberculosis from a contaminated injection, 58 of which came from a DT or DPT vaccination where depending on the incident between 11% (e.g., 10 out of 90) to 100% (e.g., 2 out of 2) of those injected caught tuberculosis. The authors concluded poor needle sterilization explained many of these cases.
•Records at the British Ministry of Health between 1935-1943 identified 5 incidents (including the 1938 one) of contaminated vaccines that collectively infected 148 people with abscesses that were predominantly composed of Streptococcus pyogenes (along with a few cases of tuberculosis). One of these became septic and was ultimately fatal. Some of the cases were traced to the injector being ill at the time of injection while others likely arose from a vaccinating doctor touching the needles prior to injection.
•In 1943, four children in Lanarkshire who received a diphtheria vaccine developed inoculation tuberculosis.
•In 1945, a group of US servicemen developed hepatitis after being vaccinated for tetanus, and of the 56 who could be examined, 11 had acute hepatitis. When it was investigated, it was concluded this was a result of contaminated syringes rather than contaminated needles.
•In 1946, 631 children in the Hyogo Prefecture in Japan received two injections of the typhus vaccine. At least 102 then suffered inoculation tuberculosis, which in many cases took a few months to manifest. A few developed pulmonary tuberculosis, and in three cases, it spread to their joints and bones, but fortunately none died (as inoculation tuberculosis was typically not fatal). This outbreak was ultimately traced to the vaccinating doctor having pulmonary tuberculosis.
•In 1948, 209 Japanese infants were vaccinated for pertussis, 62 of whom subsequently suffered from inoculation tuberculosis, 3 of whom had it travel to their hip or knee, 6 of whom became severely ill with miliary (severe) tuberculosis and 2 of whom died. The most likely source of this outbreak was concluded to be one of the vaccinators being infected with tuberculosis.
•A 1959 study of 152 cases of inoculation tuberculosis concluded those cases were due to unsterilized needles. However, it did not specify how many of these cases were from a vaccine (rather than say penicillin) being injected.
•In 1964, four children who received the DPT vaccine developed Streptococcus pyogenes abscesses despite disposable needles and syringes being used (along with the vaccine being “sterilized” with its thiomersal additive and later verified to not be contaminated). A lengthy investigation concluded a few of the healthcare workers had strep infections and the vaccines became contaminated by them touching the junction between the needle and the syringe while drawing up the vaccine.
Other Fatal Errors
In 2016, during the Syrian civil war, approximately 75 children received a measles vaccine, which was erroneously diluted with a muscle paralyzing agent (used for anesthesia) rather than saline (due to them having similar packaging), resulting in 15 of the children between the ages of 6 to 18 months dying. In 2019, following a measles outbreak in Samoa (which led to an emergency vaccine campaign) the same thing happened with two children dying within minutes of vaccination (with two nurses in turn being sentenced to five years in prison for their mistake—something likely due to people there becoming outraged over the deaths and becoming reluctant to vaccinate).
Sudden Infant Death Syndrome
In a previous article, I provided the century of evidence linking vaccination (particularly DPT vaccination) to sudden infant death syndrome (SIDS) and the clear mechanisms which had been established to cause that death. Sadder still, the issues with the DPT vaccine have been known for over a century. For example:
In 2014, unmarked mass graves belonging to Irish orphans were discovered. Further research revealed these graves belonged to a group of 2,051 children upon whom an early diphtheria vaccine was covertly tested in the 1930s. Additionally, an earlier investigation had shown that early vaccine experiments (including DPT) were conducted in the 1960s to 1970s at Irish care homes and the test subjects included babies and handicapped children.
In turn, I would argue that many of these deaths were likely due to hot lots, since (as shown earlier in the article) many other incidents had occurred with an improperly inactivated diphtheria toxin.
Sadly, as the years went by, infant deaths continued, and began to spiral out of control once the pertussis vaccine was introduced after World War 2 ( in a previous article, I made the case it had profoundly damaged society due to it frequently causing encephalitis that left the victims with permanent complications).
One of the major problems with the DPT vaccine (which included pertussis) was that it was very costly to produce cleanly. As a result, the industry insisted on using a cheaper (whole cell) formulation until they were forced to change to the safer (but still dangerous) acellular formulation after the 1986 Vaccine Injury Act.
For example, in 1976, the FDA official who was ultimately in charge of their pertussis lab for 27 years (and helped spearhead the development of a safer pertussis vaccine) stated:
With the exception of one extracted vaccine, all pertussis vaccines produced in the United States are whole cell products. As much as these vaccines resemble each other, the variability in the manufacture of vaccines from manufacturer to manufacturer and the variation from lot to lot from the same manufacturer is usually not appreciated.
Pertussis vaccine is one of the more troublesome products to produce and assay. As an example of this, pertussis vaccine has one of the highest failure rates of all products submitted to the Bureau of Biologics for testing and release. Approximately 15-20% of all lots which pass the manufacturers’ tests fail to pass the Bureau’s tests. Many of the problems associated with the production of pertussis vaccine result from the fact that little is known about the physiology and genetics of B. pertussis.
We know that pertussis vaccines passing the required toxicity and safety tests can cause adverse reactions in children. Local reactions are relatively common and include edema, erythema, induration, pain, and sometimes ulceration at the injection site. Systemic reactions are less common, but include fever, collapse, seizures, persistent screaming, and, rarely, paralysis and death. Adverse reaction rates are not accurately reported, but more adverse reactions are probably experienced with the use of pertussis vaccine than with other biologicals. With control of the disease, we may be approaching a time in which more vaccine-related problems than those due to the disease will be experienced.
The higher rate of vaccine reactions than disease has been responsible for decisions in several countries making pertussis immunization an optional procedure. It is the opinion of public health authorities in the United States that the benefits of vaccination outweigh the risks. of disease. Unfortunately, the reduced use of pertussis vaccine in those countries where it has been made an option may provide the ultimate proof of the efficacy of pertussis vaccine.
Further, the panel is convinced that currently employed surveillance systems to identify adverse reactions to pertussis are inadequate and recommends that definitive steps be taken by the appropriate subdivisions of the Public Health Service to improve them.
Note: a more detailed summary of the issues and major knowledge gaps in the production of the whole cell pertussis vaccines can be found within this article. Additionally, it should be noted that lawsuits for DPT injuries were so frequent and costly that manufacturers had to continually raise the prices (e.g. from 1977 to 1993, in 1993 dollars, the contract price of the DPT vaccine increased by 1033% while the catalog price increased 2847%) and many companies stopped producing it.
One of the most notorious DPT hot lot issues happened between August 1978 to March 1979, where in Tennessee, 11 infants died suddenly within 8 days of vaccination, 4 of whom died within 24 hours. Further investigation determined they had all received the same vaccine lot. This led to the hot lot being recalled.

Despite this, the government denied the vaccine could be at fault:
In June, CDC director Foege wrote a memo to the Surgeon General stating that the experts “did not feel that a causal relationship had been established between vaccination with DPT from Wyeth's lot #64201 and sudden infant death in infancy. However they did not feel that a causal relationship could be totally excluded.”
Note: this stance was also found in a journal article the CDC later wrote about the incident.
More surprisingly, the FDA blocked the manufacturer from suggesting this either:
Three weeks later, Foege’s interpretation of the events stated in this memo to the Surgeon General was used by Harry Meyer, Director of the FDA Bureau of Biologies, as evidence to oppose a request by Wyeth Laboratories to list among its pertussis vaccine contraindications circumstances thought to predispose to SIDS. Meyer told Wyeth in a July 11 letter, “Based on the available data we do not see a medical basis for listing circumstances thought to predispose to SIDS as contraindications to the use of DPT vaccine. We do not agree, therefore, with your proposal on page two of the circular under ‘Contraindications.’ There is no evidence that such a change would prevent SIDS.
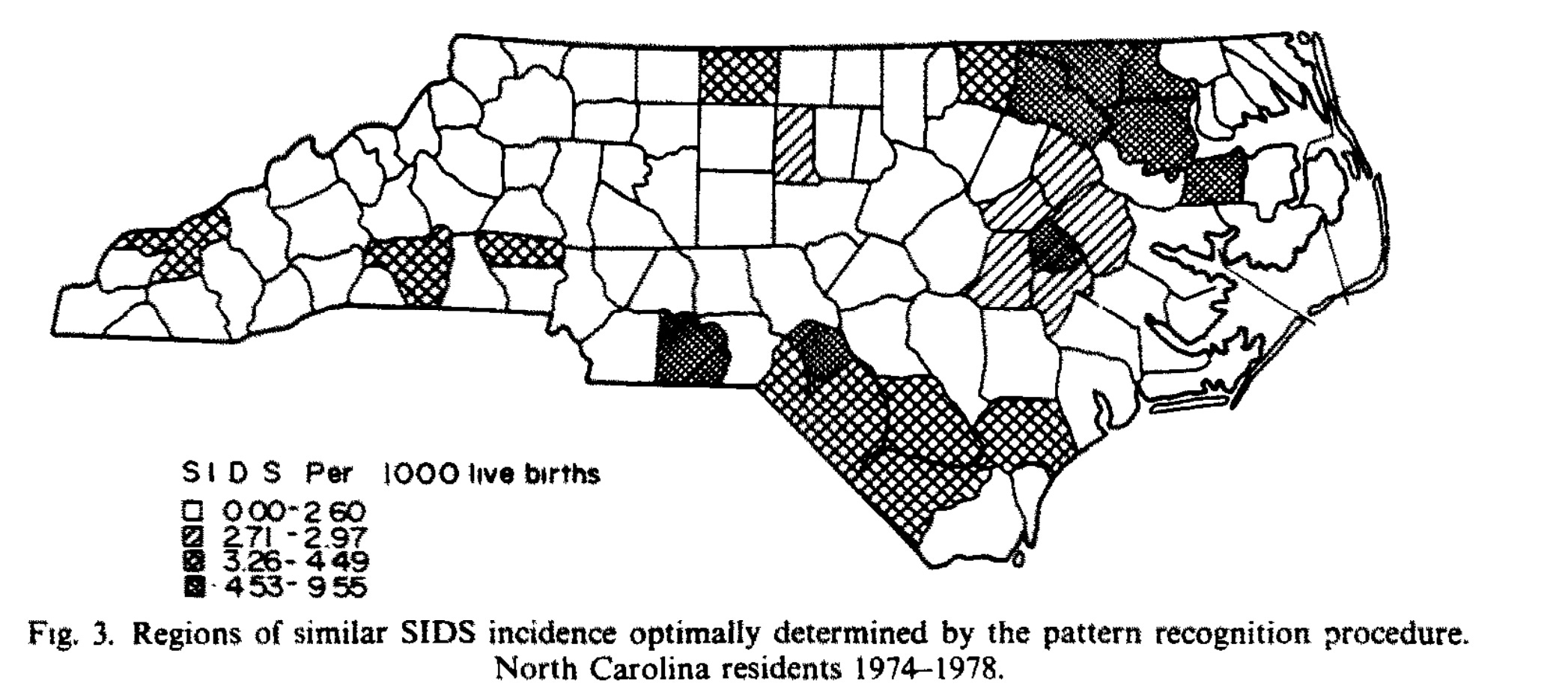
Subsequent research found other previously undetected clusters of SIDS had also occurred. For example, in North Carolina between 1974-1978, a geographic distribution matching how a hot lot might have been distributed was found:
In 1984, two years after NBC aired its pivotal program exposing the dangers of the DPT vaccine, The Fresno Bee (a California newspaper) published one of the last critical investigations of a vaccine that ever appeared in the mainstream media. For example, one article highlighted how in 1978, a study was conducted to investigate the safety profile of the DPT vaccine within 48 hours of immunization, but after researchers discovered adverse reactions were 5000% higher than expected, the study was ended early, and those concerning results were not reported in the final publication (rather they only were reported to the FDA).
Some of the key quotes from that 1984 series included:
Shocklike deaths following DPT shots were reported in the Journal of the American Medical Association in 1933 and 1946.
In Fresno County, Coroner Dr. David Hadden researched records from an unusual cluster of crib deaths in 1981. He said the question about DPT vaccination was not routinely asked of parents.
[Dr. Kevin] Geraghty independently researched the 10 crib deaths in Contra Costa County in the first half of 1983. Three of them showed "disturbing clinical histories not typical of crib deaths," but typical of shock, he said.
“Physicians are innocent victims," said Los Angeles attorney Andrew Dodd." It’s a very sad situation and it’s a scandal, in my opinion, of enormous proportions. And I’m ashamed of it. I am ashamed that I know more than a pediatrician [about pertussis vaccine]. That is not right."
Dr. Kevin Geraghty: "A pediatrician is more likely to believe that the dangers of his stethoscope choking him are higher than DPI causing the degree of damage that I would say it does."
When Geraghty began studying the DPT vaccine 18 months ago, he said his goal was to debunk the critics of the vaccine. "I am a pediatric immunologist; I was trained in immunology. It didn’t take very long for me to know something was very, very wrong."
But another doctor might not know that. Said Dodd: "When he is administering a mass-immunization product — polio, rubella, DPT — he assumes that the vaccine is almost as safe as water. ‘Mass immunization product’ — that means something to him.
"...He’s not going to take the time to read the medical literature because he knows the reactions. . . are very, very rare. The trouble is It’s wrong. it’s wrong, wrong, wrong."
"If physicians only understood that... they are giving a neurological poison... it isn’t a secret, except it’s not generally known."
In addition to exposing the dangers of the DPT vaccine, this series focused on the production issues and hot lots associated with the vaccine.
For example, they highlighted that the vaccines varied greatly from batch to batch:

Note: the pertussis vaccine with high doses of protective units (e.g., those over 24 were found to be the ones most frequently associated with causing brain damage).
Likewise, one article specifically focused on the problems with vaccine hot lots:
In the 40 years that pertussis vaccine has been given to American children, only four lots have been withdrawn from the market as unsafe. Sometimes such lots are called hot lots.
As defined by the National Centers for Disease Control, a hot lot is one that generates reports of more than two deaths, two convulsions, or ten adverse reports in total.
On March 30, a memorandum to Dr. Alan R. Hinman, CDC’s immunization director, identified 13 batches of Wyeth Laboratories vaccine and six from Lederle Laboratories as potential hot lots.
The reports of deaths, brain damage, convulsions, abscesses and allergic reactions totaled 413— including 16 deaths— for Wyeth’s 13 lots, and 114 reports —with three deaths — for Lederle’s six lots.
How many doses did those lots provide? And where had the vaccine been shipped? Without answers, the CDC couldn’t determine the significance of the numbers or connect complaints in other parts of the country. And Wyeth and Lederle gave no answers.
Betty Hiner, of the Food and Drug Administration’s Office of Biologics Research and Review, telephoned the companies on March 30th about some of the problem lots.
Dr. Harrison C. Stetler and John R. Mullen, CDC officials who had sent the original memo to Hinmän, later reported to him "that Lederle does not respond to the inquires about distribution. . . and Wyeth declined to release this information on outdated lots."
As a result, they said, they couldn’t determine whether the lots "represent reporting bias or actual higher reaction rates and whether Wyeth lots have higher rates of reactions than DPT vaccine of other manufacturers."
The lots remained on the market.
(Spokesmen for Wyeth, Lederle and Connaught laboratories, citing litigation, would not comment about hot lots.)
The FDA is considering changes in the regulations so data on vaccine lots and distribution can be obtained from the manufacturers.
Dr. Gerald Faich, the director of epidemiology and biostatistics, said: "We have not systematically asked for that information in the past. We have every intention of getting it in the future."
Faich also disagreed with the CDC’s definition of a hot lot, which "is not a universally accepted definition by any means." Faich said the CDC numbers are merely a "statistical clustering of adverse reactions."
"My impression is that there has not been a true hot lot that required withdrawal from the market excepting Sciavo’s," Faich said.
Under pressure from the FDA and the CDC, Sclavo Inc. recalled two batches for too many abscesses.
Only two other lots have been withdrawn:
•Wyeth’s designated lot 64201 was voluntarily withdrawn by the manufacturer after a cluster of 11 deaths in Tennessee in 1979.
•National Drug Co. lot, 40 years ago, referred to in an article in the 1946 Journal of American Medical Association. For every lot taken off the market, dozens of potential hot lots have not been recalled. One was lot No. 1182, made by the state of Michigan in 1975. (Massachusetts also manufactures DPT vaccine.)
Michigan had made too much DPT in its Lansing laboratory and wanted to sell it to other states. That required FDA testing and approval, as with any other manufacturer.
However, the FDA denied approval and returned the vaccine, saying it was 300 percent too potent.
State health officials disagreed and decided to test the vaccine on children in Ingham County (Lansing). Despite more adverse reactions than usual, health officials released 400,000 doses of the DPT vaccine for use throughout the state a month later.
The Detroit News reported that three children were left with permanent brain damage. Lawsuits In those cases and four others were filed against the state of Michigan.
However, what is the most remarkable about the DPT hot lot story is what Wyeth (the manufacturer of the 1979 Tennessee hot lot) did:

In essence, Wyeth decided that since it was impossible to avoid producing hot lots, the best solution would be to distribute the lots around the country so the deaths from it would be much less apparent (which mirrors the common industry mantra “the solution to pollution is dilution). In turn, I would argue the two main reasons we do not hear of hot lots now are because:
•Their distribution is no longer geographically clustered.
•Both the medical profession and media have become much more reluctant to report these events, which hence is why we have to scour much older records to find candid discussions of the hot lots of the past (even though as Wilson noted, at the time the these incidents were still frequently covered up).
The Anthrax Vaccine
Five of the most damaging vaccines released to the American public were the smallpox vaccine, the old DPT vaccine, the HPV vaccine, the COVID-19 vaccines, and the anthrax vaccine. In turn, when you study the history of each of these events you will notice an eerie number of parallels (e.g., many of the injuries were very similar and the government had a nearly identical insistence on keeping the vaccine on the market and covering up every injury that occurred).
Note: I believe the most dangerous vaccines are those that cause the greatest degree of blood sludging (micro-clotting) within the body. This is typically either due to it being a particularly dirty vaccine that is sourced from a killed bacteria (whole cell pertussis and anthrax), it having a particularly zeta potential disrupting adjuvant (which the HPV vaccine required since a standard aluminum adjuvant could not produce a sufficient antibody response) or it mass producing the spike protein within the body (as the spike protein is highly disruptive to zeta potential and hence causes microclotting and microstrokes).
In the case of the anthrax vaccines, they were a rushed and experimental program which began during the Gulf War under the belief our soldiers might need protection from Saddam Hussein’s anthrax (which never happened). While the Gulf War was arguably the most one-sided victory in American history (hundreds of times as many Iraqi soldiers died as Americans did), it ended up also being one of the most devastating ones in our military’s history as almost 36% of soldiers (approximately 250,000 of the 697,000 who served) came down with a debilitating illness that eventually came to be known as “Gulf War Syndrome (GWS).”
While the cause of GWS has never been established, by far the strongest evidence links it to the anthrax vaccine (as many who were not in the Gulf who received the vaccine also developed the illness). Sadly, like COVID-19, rather than acknowledge there was an issue, the military continued to mandate this experimental vaccine, even as valuable pilots were lost and widespread resistance broke out against the vaccine. At the time (despite continual denials from the Pentagon leadership), many servicemen believed an experimental oil adjuvant (squalene) was being used in the vaccines as:
•There was a history of squalene being used as an experimental adjuvant and it causing reactions similar to what were observed from the anthrax vaccines.
•It was believed that squalene was necessary to make the anthrax vaccination work.
•A custom antibody test showed injured veterans had an allergy to squalene, and in at least one case, a veteran who tested negative before his vaccination tested positive after his vaccination.
•There was a commercial need to develop a squalene-based adjuvant (MF59), and as the injured veterans predicted, the adjuvant they thought was in the vaccines hit the market for civilian vaccines later.
•When an anthrax vaccine lot was thrown overboard by soldiers in 2003, according to one author (I was not able to locate a copy of the results he cited) it was independently tested and found to contain squalene.
•When the suspect lots were tested by the FDA, they were found to have trace amounts of squalene:
Lot FAV 020 had 11 parts per billion of squalene
Lot FAV 030 had 10 parts per billion of squalene
Lot FAV038 had 27 parts per billion of squalene
Lot FAV043 had 40 parts per billion of squalene
Lot FAV047 had 83 parts per billion of squalene
Note: these concentrations are very small. However, in a 2001 study of MF59, a 200nm concentration of MF59 (82.15 parts per billion) was found to elicit an immune response.
Given that the concentrations in these lots increase in parallel to ascending lot numbers, many were suspicious that a test was done, especially since their concentration roughly doubled each time (which is a common thing done in dose-response studies).
Note: curiously, an independent researcher discovered something similar when he compared the toxicity of Pfizer’s vaccine lots in VAERS to the alphabetical lot codes (e.g., see this video, this video and this video) or looked at when the most dangerous lots were deployed on the market (e.g., see this report). Later, when the total number of vaccines in each lot became known, he was able to show this pattern did indeed exist (see this report and a later confirmation from Dutch data). Later, he also found the pattern existed within the Moderna lots (the code was just a bit harder to spot), which suggests that like the anthrax vaccine, there was a need to determine the correct dose of this new technology (i.e. how much was still effective without being too toxic).
Eventually, due to how many problems the anthrax vaccine campaign created, a Federal Judge ruled that it was illegal force the members of the military to receive an experimental vaccine and a Congressional investigation was conducted (which characterized the Department of Defense as being “unusually evasive”). Meryl Nass MD worked with the Congressional investigators. From reviewing the documents they uncovered, she discovered that like the whole cell DPT vaccine (the older one), there were a lot of issues with producing the anthrax vaccine (which essentially required culturing and then killing a large number of anthrax bacteria), making it in her words “a particularly dirty vaccine.”
However, the most remarkable thing she shared with me was that the Government Accountability Organization (the GAO serves as Congress’s watchdog), discovered that Bioport (the vaccine’s manufacturer) changed the filters on the final vaccine product to larger ones that did not become clogged (but likewise were no longer as effective for purifying the vaccine—in effect making the vaccine become “hot”), and failed to notify the FDA of this critical change. Similarly, the FDA also had concerns about other aspects of Bioport’s quality control, repeatedly cited Bioport for their manufacturing processes, and suspended shipments of the vaccine from their facility.
Note: Bioport later changed its name to Emergent Biosolutions. Recently, it was tasked with manufacturing Johnson & Johnson’s COVID-19 vaccine, and after quality control issues again emerged, the FDA required Emergent Biosolutions to dispose of millions of improperly produced doses.
As such, Nass’s opinion was the primary issue was the vaccine itself, and the squalene story was a red herring (e.g., she gave me reasonable arguments to dismiss the points of evidence I cited above).
Note: There is one other compelling theory about what causes Gulf War Illness (which is synopsized here).
Operation Warp Speed
At the start of the COVID-19 vaccination program, we had quite a few major concerns about the vaccines. One of which is related to quality control. Specifically:
•In 2020, FDA inspectors came forward and disclosed that there are serious deficiencies in America’s vaccine manufacturing facilities (which given what you have read thusfar in this article should not come as a surprise). Furthermore, they attested that the FDA has done very little to address this issue, and that these quality control issues became much worse during Operation Warp Speed since as much red tape as possible was cut to speed up the vaccine rollout.
Note: as numerous whistleblowers in the vaccine clinical trials have testified, the FDA refused to investigate clear evidence they repeatedly presented to the FDA which showed that the clinical trials were being run in a fraudulent manner which was inflating vaccine efficacy and concealing vaccine injuries.
•Producing any product at scale is quite difficult. Given that the mRNA vaccines were an entirely new technology, it was highly unrealistic that Pfizer or Moderna would be able to manufacture a consistent product in the volume that was being requested of them.
Note: inconsistent manufacturing is actually a longstanding issue, especially in products that are not subject to as rigorous inspection (e.g., all vaccines are “safe and effective” and hence typically given the benefit of the doubt by those overseeing them) or those immune to lawsuits which would incentivize better production methods (e.g., vaccines). To illustrate, in 2021, Christopher Exley’s team found that the aluminum content of childhood vaccines varied greatly from lot to lot (which is significant as aluminum is one of the primary agents responsible for most vaccine injuries).
•As leaked regulatory documents showed (prior to the vaccine rollout), there were serious issues with preserving the mRNA within the vaccines.
Shortly after the vaccine came out, I began having people call me up to ask about serious injuries (e.g., sudden cardiac death or a stroke) they’d had after the vaccine (which I compiled in a log here). Two cases jumped out at me, as both had occurred in a husband and wife. Given that the severe injuries were still relatively rare, the odds of both a husband and wife getting one in my still small sample seemed highly unlikely, and I tentatively concluded hot COVID-19 vaccine lots existed that both of them had gotten due to them going to the same place for their vaccination. Conversely, I and many colleagues also noticed that the reactions patients reported to the vaccines were either quite strong or non-existent (rather than being a gradual spectrum), which led many of us to suspect many of the vaccines were inert (e.g., the most talented diagnostician I know told me he was convinced many of the vaccines his patients had received were saline placebos).
Before long, independent investigators then discovered that certain lots in VAERS had a much higher rate of adverse events (e.g., deaths) than others (e.g., almost all of the vaccine deaths were caused by around 5% of the vaccine lots), but like every single case in the past, they were not pulled from the market. In turn, many who were injured reported receiving one of the ‘hot lots’ (which can be found on this website).
The major challenge with assessing the hot lots however was that most adverse reactions are not reported to VAERS (or their European equivalents) and that there was no way to know what percentage of the total injections resulted in an injury (as the lot size was not known). To some extent, this issue was addressed by looking at all reactions to a specific lot and seeing what percent of them were severe (e.g., death). Later, a FOIA request eventually got those lot numbers and clearly showed that the suspected hot lots we indeed hot and should have been taken off the market. Unfortunately, the FDA chose to not release the lot sizes for many of the batches which were suspected to be the most toxic.
Note: evidence has also emerged showing the Moderna vaccine (which has a higher mRNA dose than the Pfizer vaccine) on average has a higher rate of adverse events. For example, Igor Chudov showed the Moderna vaccine was roughly twice as likely to cause pregnancy issues like miscarriages than the Pfizer vaccine, and a not yet published report of a large data set (which was shared with me in advance of its publication) found that the Moderna vaccine increased one’s mortality risk by around 50% compared to Pfizer the vaccine.
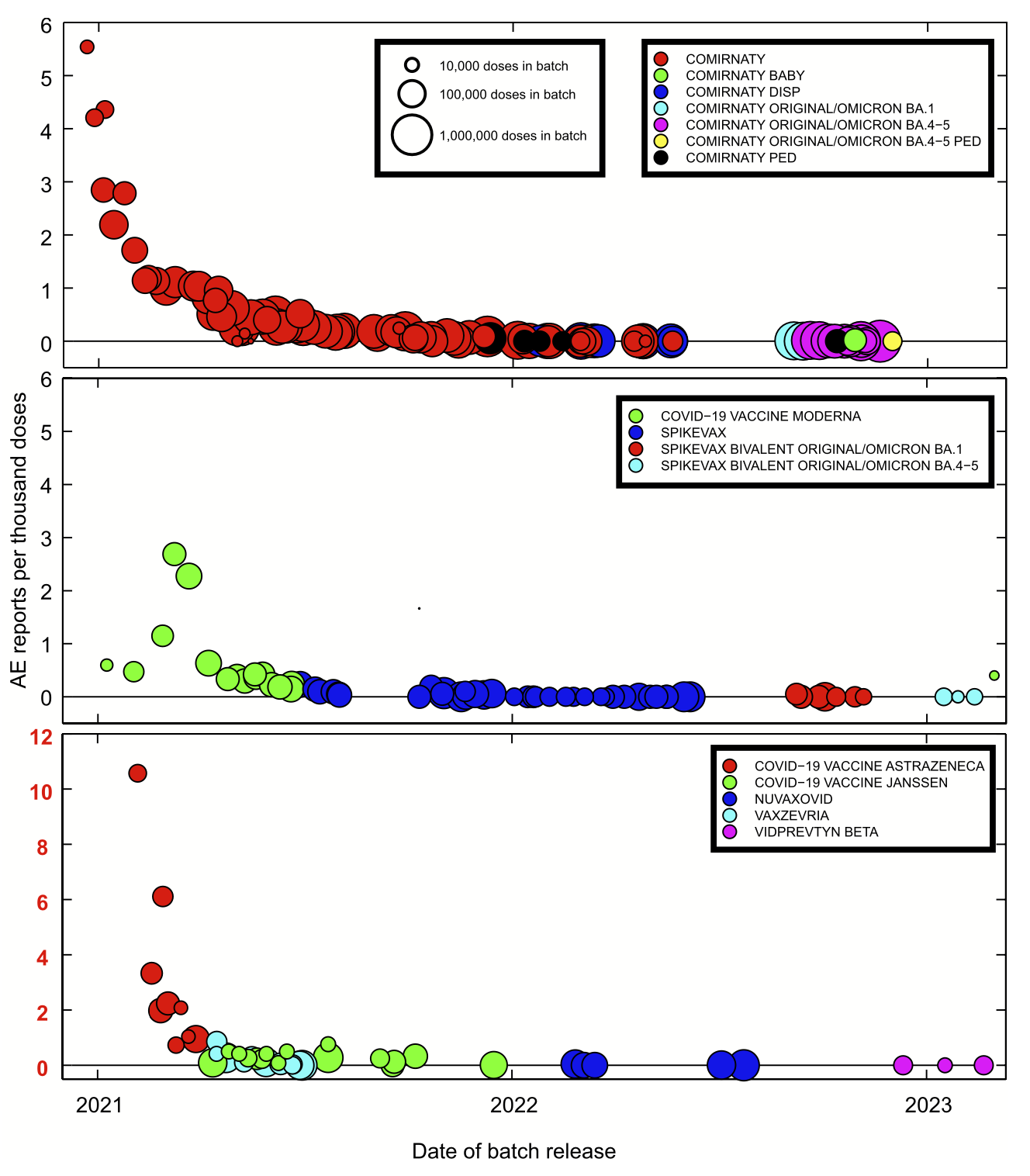
More recently, a peer-reviewed paper was published using the total adverse reactions and lot sizes within Belgium that demonstrated this dose toxicity indeed exists. This graph came from that paper:
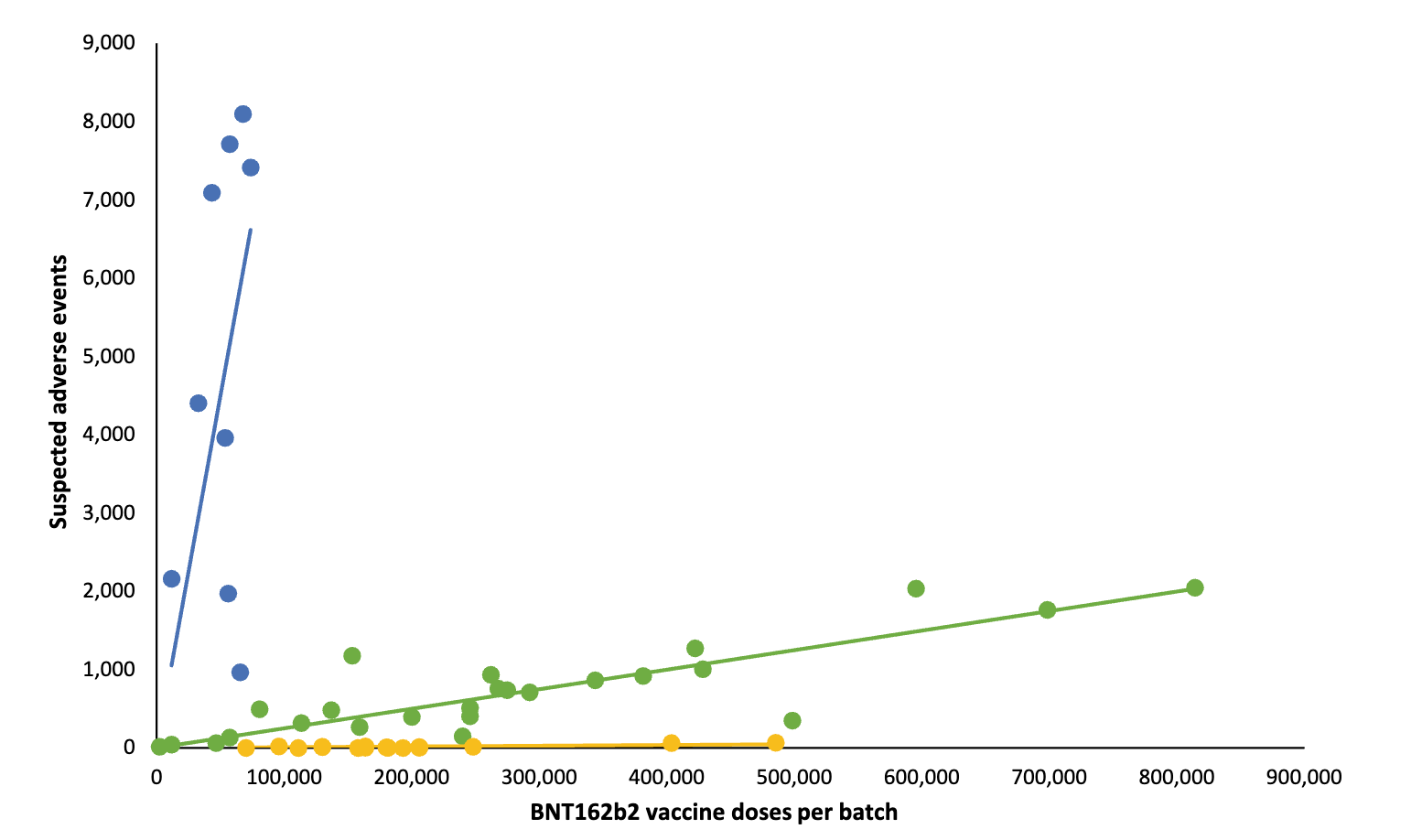
Curiously, the German regulators never tested the yellow (non-toxic) lots prior to releasing them—which alongside their lack of toxicity led independent academics to suspect the vaccines were placebos and the German government knew as such. Remarkably, another researcher determined that only the hot lots were given expiration dates by the CDC, again suggesting many of the existing lots were known to be placebos.
Note: the approximate distribution of the lots was 4.22% were hot lots, 63.69% were regular lots (with medium toxicity) and 32.09% appeared to be placebos. Compared to placebo lots, the regular lots were 38.2 times more likely to cause a reaction, 35.6 times as likely to cause a serious reaction, 30.45 times as likely to cause a death. Comparatively, the hot lots, when compared to the regular lots were 37 times as likely to cause a reaction, 5.8 times as likely to cause a serious reaction, and 13.68 as likely to cause a death.
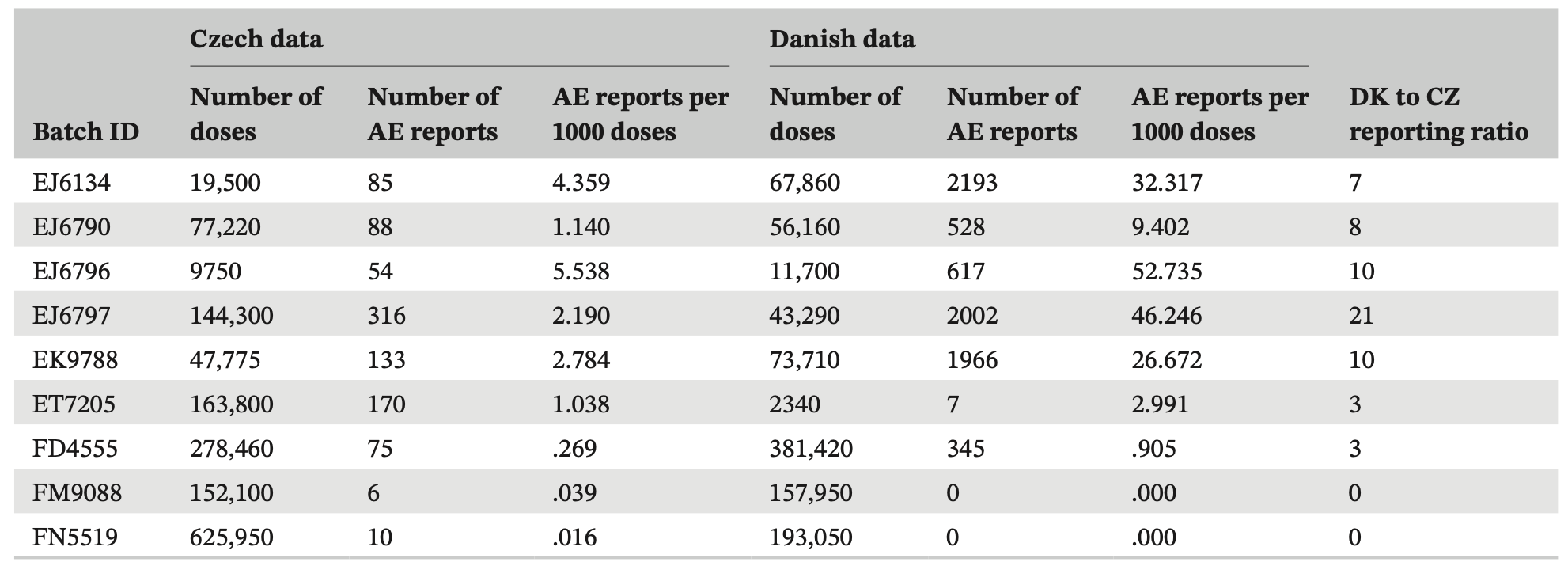
Later, a similar trend was found in data from Czechoslovakia:
Then when these lots were compared to data from Denmark, it was found that the same lots were hot in both countries, although there was a far greater underreporting of adverse events in Czechoslovakia:
Most recently, a whistleblower in New Zealand who access to both the vaccination status of individuals, their mortality status, and the length of time between their vaccination and death chose to jeopardize his freedom to reveal what the database he had worked with showed (discussed here). One of his many disclosures were that certain lots had a much higher rate of causing death than the others.
Note: one of the largest issues we face currents is a lack of data transparency (e.g., the very limited data we get from VAERS is only available to the public because activists fought tooth and nail for it in the 1980s). Were basic data transparency to exist, things like the COVID vaccine disaster could not have happened and individuals like the New Zealand whistleblower would not have to risk their entire future to get us access to some of it.
Quality Control
In addition to signs suggesting the presence of hot lots (which could not exist if a consistent manufacturing process was followed) some of the other indications the mRNA vaccines were adulterated products included:
•Physical contaminants—Japan pulled 1.63M vials of Moderna’s vaccine after visible metal particles were found in them and when examining vaccine vials, Additionally, Ryan Cole (shown below) found glass shards in the vaccines. Both of these suggest the production of the vaccines was rushed to the point basic quality control steps were not taken.
•mRNA integrity—Leaked files from Europe’s FDA demonstrated that drug regulators were aware that much of the mRNA in the vaccines was mRNA fragments rather than the complete vaccine sequence. This suggests that the vaccine mRNA was poorly produced.
•mRNA stability—The mRNA was observed to break down quickly (e.g., into the previously mentioned fragments) and it was unclear how to prevent this.
Note: I suspect the obsession with ultra-freezing the vaccines at the start of the roll-out was a ploy done by Pfizer to assuage the regulator’s concerns the mRNA was fragmented under the logic that the breakdown was only a result of inadequate temperature control after production, rather than also being an inevitable consequence of the manufacturing process. For example, we found evidence (which to the best of my knowledge was never refuted) that the data (Western Blots) Pfizer produced for regulators to demonstrate the mRNA vaccines were producing their intended protein product were in fact computer forgeries (which in turn suggests the actual proteins being produced were not what was advertised).
•Temperature control—Once the vaccines hit the market, the interest in ultra-freezing them rapidly waned and before long was largely forgotten (again suggesting all of that was largely for show). Similarly, more and more we observed vaccines being left out on a table all day long at vaccination sites. This again suggested people were receiving different vaccine doses as some contained mRNA which had more significantly broken down (e.g., those received at the end of the day).
Note: since a large number of relatively untrained individuals administered the vaccine during the rollout, it is likely other steps were also incorrectly followed (e.g., aspirating before injecting, or drawing up the correct vaccine dose).
•Hot lot time distribution—In Europe, lots were found to be more toxic in Belgium (the vaccine production site for Europe). This suggested that the closer to the time of production a vaccine was injected, the more harmful it was (whereas later on much of the mRNA had time to break down and was less able to make spike protein in the body). This was also demonstrated by data repeatedly showing mRNA vaccines in Sweden rapidly became less dangerous the further from their production time that they were injected. That finding was then corroborated within US data. Finally, since the leaked EMA documents listed how much mRNA was present in each vaccine lot, the lot mRNA integrity was compared to the toxicity of each batch—from which it was determined that the more toxic lots were those with more intact mRNA.
•Vaccine production—when Ryan Cole did a recorded examination of the vaccines with Del Bigtree they found many were saline, that the lipid nanoparticle concentration varied immensely from lot to lot and that a variety of other contaminants from poor production were present (e.g., metals):
This suggests that there was either very poor mixing when the vaccines were packaged (leading to some having lots of the lipid nanoparticles and others none) or that the vaccine manufacturers were unable to produce enough vaccine to meet the existing orders and switched to packing placebo vials to meet their contracted orders.
•Empty nanoparticles—In one NMR examination of 4 vaccine vials, it was determined that the lipid nanoparticles, but not the mRNA, were present in each vial. This suggests that the vaccine was not prepared consistently or that the manufacturers ran out of mRNA to fill the vaccines with.
•A citizen’s investigation (which has since been replicated) discovered that bacterial DNA plasmids (which could potentially integrate into the genome) were present in the vaccine. This was a consequence of the vaccine production process being switched after the clinical trials to a more scalable one that used genetically modified bacteria to mass produce the DNA that served as the template for the vaccine mRNA and insufficient purification steps being taken to remove those plasmids (and potentially other harmful aspects of the bacteria like their endotoxins).
Note: more dangerous vaccine lots were also found to have higher concentrations of the plasmids.
Based on all of this, I am relatively sure the primary issues with the COVID vaccines was poor manufacturing, which oddly enough helped many of us since it resulted in many partially active or inactive lots being put onto the market (e.g., due to their mRNA degrading or due to vials being filled with saline). Conversely, most of the injuries seem to have resulted from lots that should have never been allowed to remain on the market.
Note: there are many other microbial contamination issues with vaccines I was not able to go into with this article as it’s already on the long end.
Conclusion
Proper quality control is a key foundation of pharmaceutical medicine and one of the primary things regulators are supposed to enforce. Unfortunately, as these events show, that is not at all what happened. Sadder still, since the majority of medical professionals no longer knew (or even could conceive of the possibility) that vaccine hot lots exist, unlike the doctors and health officials in the past who immediately saw what was going on and stopped the lot, no one this time around did. For example, the New Zealand whistleblower showed that a few vaccinating doctors had an extraordinary high rate of deaths (between 10 to 24% of those they vaccinated died), yet none of them spoke up.
Recently, Dr. David Gortler (who previously served as a senior advisor at the FDA) at a panel Senator Ron Johnson held about the COVID vaccine disaster explained why the contamination and widespread variability we are seeing in the vaccines (e.g., the hot lots) being completely ignored and the complete lack of transparency as to what is actually in the vaccines is so unprecedented:
Note: I wanted to highlight this quote from Gortler “Unfortunately, around 70% of the 127 page document that explains the methodology to perform quality control on RNA injections are redacted much like the document I've shown here.”
When I reviewed Wilson’s book and considered all the vaccine disasters which had happened in the past (especially those from hot lots being released) I was left with the impression that many of those involved felt immense regret over what had happened and were terrified of these events, but simultaneously, believed that vaccines and serums were the only option they had to confront the (very real) plagues facing humanity and that this reality thus justified that collateral damage and lying to public about the injuries so the programs could be maintained. Likewise, I believe their deep fear of contaminated lots helps to explain why they relentlessly pushed for toxic antimicrobial agents (e.g., the mercury preparation thimerosal) to be added to the vaccines regardless of how much the public protested the toxicity of these agents.
In essence, I would argue that is identical to the situation we face now—especially given that at that time, ultraviolet blood irradiation (as shown here) had proven itself to be able to cure most of those dangerous diseases, while now, numerous off-patent therapies (including ivermectin, hydroxychloroquine, and again, ultraviolet blood irradiation) had proven themselves to cure COVID-19. Unfortunately, in both cases, the medical system (e.g., the American Medical Association) suppressed those competing products so it could monopolize the practice of medicine and created a false dichotomy in the minds of the medical profession that pushing along a dubious injection was indeed their best option.
In my eyes, the logic that we had “no other choice” was what convinced regulators again and again to lower the standards on injectable biologics (e.g., passing the 1986 Vaccine Injury Act so that the vaccine producers would be exempt from liability for defective products and not go out of business). In this article, I have tried to show why that was an immense mistake, and that as long as the manufacturers are exempt from liability, production issues will plague the vaccine supply.
Unfortunately, due to the medical industrial corruption we live under, it is unlikely this will change. If anything, as COVID has shown, it will continue to worsen as the corruption within our government continues to worsen as well—the exact opposite of what should be happening as the technology to make cleaner biological products has advanced immensely over the last century.
My colleagues and I hence believe an alternative solution is needed. Presently, we believe the best option is to allow for independent third-party testing of vaccines and for those results to be published—as if that data is available, manufacturers will be forced to produce cleaner products if they want to stay in business. In turn, my sincere hope is that the COVID vaccine disaster will begin to create the political will to bring about that change, and it is for that reason that I spent the last week working on this article to clearly make the case for why we have an immense quality control issue in this industry that must be addressed.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.
Thank you for yet another excellent essay. I am in awe of, and so very grateful for your productivity!
About the quality control issues. Back in late 2022 Debi Evans of UK Column did a very thorough interview with pharmaceutical manufacturing expert Hedley Rees. I would assume you have seen it, but perhaps many readers here who have not might find that it sheds important light on the subject.
Source video: "From Molecule to Man: The Lifecycle of an MHRA Medicine"
UK Column News, Debi Evans, October 31, 2022
[Interview with Hedley Rees]
https://rumble.com/v1qsasc-from-molecule-to-man-the-lifecycle-of-an-mhra-medicine-that-will-fail.-uk-c.html
TRANSCRIBER'S NOTES: This is an Internet interview for UKColumn.
Debi Evans: https://www.ukcolumn.org/writer/debi-evans
Hedley Rees: https://hedleyrees.substack.com/
EXCERPT 1 - Background
"typically you're looking about 10, 11 years... with a biologic it could be longer because it's a process that is so difficult. And with a novel therapy such as an mRNA vaccine, well, who knows? But 9 months or 12 months, you know, is, is a joke. It is a joke."
https://transcriberb.dreamwidth.org/150689.html
EXCERPT 2 - Radical Transformation in Industry Outsourcing
"it's hard to believe that this ever, ever happened, to be honest."
https://transcriberb.dreamwidth.org/150794.html
EXCERPT 3 - The 5 Dose Frozen Vials
"they must have a different backend on the packaging line. Instead of having the bit that fills individual vials, they will have put something on there that puts the vials into these 195 in cardboard trays. They would then have to have got some ultra low freezing capability, freeze them down, and then they would have been shipped like that. That's never, ever happened, in, you know, in the whole history of medicine. And you'd know, I'd, I'd sort of stake my life on that."
https://transcriberb.dreamwidth.org/151072.html
EXCERPT 4 - Collapse of Regulatory Competence
"what's left is just a broken, broken system."
https://transcriberb.dreamwidth.org/151426.html
EXCERPT 5 - The Bad Batches
"if something's not made to GMP, then you can't guarantee it's safe."
https://transcriberb.dreamwidth.org/151626.html
EXCERPT 6 - "You can only defy gravity for so long"
"this is all going to fall apart."
https://transcriberb.dreamwidth.org/151869.html
The most damning crime of modern medicine was not disclosing Sudden Infant Death Syndrome's association with recent vaccination. https://danielnagase.substack.com/p/history-babies-vaccines-and-sudden The fact that legislators let companies mix their lots so that side effects couldn't be clustered in one area comes a close second. Until you can put legislators who voted to permit these crimes in jail, I'm afraid nothing will change.