The Century of Evidence Putting Light Inside the Body Is A Miraculous Therapy
How Ultraviolet Blood Irradiation treats severe many severe Cardiovascular, Infectious, Obstetric, Autoimmune and Neurological Diseases

Story at a Glance:
•Natural light is an essential nutrient many of us do not have enough of within our bodies. Because of this, when ultraviolet light is added to the bloodstream, phenomenal health benefits emerge.
•Once ultraviolet blood irradiation (UVBI) was discovered in the 1930s, it produced miraculous results for patients on the verge of death and was quickly adopted by hospitals throughout America. There, it demonstrated remarkable efficacy for a wide range of diseases, and the doctors who pioneered its use compiled a large body of research.
•To neutralize this competition, the American Medical Association published a small doctored study that “debunked” UVBI, and before long it became a forgotten side of medicine. The Russians and Germans however recognized the value of it, and for decades have produced research showing UBVI’s remarkable utility for a variety of challenging medical conditions both within and outside the hospital. However, in America, UVBI is primarily used by integrative practitioners who need effective tools to treat complex illnesses (e.g., Lyme disease, Chronic fatigue syndrome, spike protein injuries, or migraine disorders).
•In this article we will review the hundreds of studies showing UVBI's utility for a wide range of medical conditions (e.g., cardiovascular diseases, infertility, preventing miscarriages, many autoimmune disorders, preventing complications from surgery, and treating a myriad of challenging bacterial and viral infections), explain how UVBI works, and provide the resources for those wishing to best utilize this therapy.
In this publication, I have attempted to make the case that we are routinely denied vital knowledge, treatment, and care, in order to protect the interests of the medical industrial complex (as you can only sell costly but abysmal therapeutics to people if no alternatives exist). As that is a rather extreme allegation to make, I’ve tried to show piece by piece how this is indeed the case. For example:
•I’ve highlighted how many unsafe and ineffective pharmaceuticals make it to market (and sometimes are even mandated) because the panels that approved them were stacked with people taking money from the manufacturer (which I recently argued was a tactic Anthony Fauci weaponized against America).
•I’ve discussed how in the early 1900s, the American Medical Association was taken over by a group of unscrupulous businessmen who decided to fund the association by unconditionally promoting anything they were paid to (which amongst other things is why there were so many AMA advertisements of doctors promoting smoking) while simultaneously using the government to outlaw each competing therapy that refused to sell out to them.
•I’ve shown how American society has been methodically separated from the fundamental requirements for good health (e.g., sleep or sunlight), how damaging losing each of those is, and just how far the marketing industry often goes to ensure we never reclaim those basic requirements for health.
Assuming the first three are indeed true, it then suggests that a variety of remarkable medical innovations exist that have been buried. In this article, I will discuss one of those, ultraviolet blood irradiation (UVBI), both because there is a vast body of evidence for its use and because, unlike many of the other lost medical technologies, it’s still relatively accessible.
The Importance of Sunlight
A widely held view now exists that sunlight (particularly its ultraviolet component) is dangerous and something we must avoid and shield ourselves from. In a recent article, I showed how this came from a 1980s public relations campaign that the struggling dermatology profession used to rebrand themselves as cancer fighters. Treating skin cancer (by cutting it out) is both easy and incredibly lucrative, hence making dermatology the most desired specialty in medicine.
Note: to illustrate the importance of sunlight, a 20 year prospective study of 29,518 Swedish women found that those who avoided sunlight were 130% more likely to die than women who had regular sunlight exposure, and much more likely to develop a variety of medical conditions (e.g., they were twice as likely to get cancer).
In the first half of this series (which provides critical context for this article), I thus attempted to shine a light on the critical benefits we receive from sunlight, how many different illnesses result from artificial lighting and lack of sunlight, and that the same changes observed in plants and animals from unhealthy lighting are also observed in humans. Some of the key points I covered there included:
•Unhealthy light causes and exacerbates a wide range of cancers.
•Unhealthy light significantly increases the risk of a variety of infections (particularly within livestock).
•Unhealthy light contributes to a variety of behavioral disorders (e.g., ADHD or animals attacking each other).
•Healthy lighting significantly increases the health, fertility, and productivity of domesticated animals.
•The normal growth cycle of many plants and animals is dependent upon healthy light from the environment. Likewise, the circadian rhythm (which regulates sleep and healing) is heavily disrupted by unnatural lighting.
•Many organisms are extraordinarily sensitive to unnatural lighting. Additionally, many biological structures are highly sensitive to specific wavelengths of light, which is problematic because artificial lighting typically has a few narrow bands of light, rather than a complete spectrum.
•Light plays a critical role in generating circulation throughout the body and protecting the blood vessels from damage.
•Ultraviolet light is particularly critical for health. In turn, the most dramatic benefits of using light therapies are seen when appropriate amounts of UV light are administered to the body.
•Glass blocks UV light, so since much of the sunlight we are exposed to is filtered through glass, modern life prevents us from having access to that light, and hence there is a widespread deficiency of UV light in our society.
•Since the skin has difficulty absorbing UV light, we instead receive much of the light which enters our body through the eyes. In turn, when individuals where glasses that block sunlight from entering their eyes, a wide variety of health problems can ensue that resolve once the glasses are addressed.
The major challenge with light therapies is getting the light inside the body. Fortunately, methods have been developed to do just that, and for over a century, they have produced truly remarkable results.
The History of Ultraviolet Blood Irradiation
One of the oldest “proven” therapies in medicine was having people bathe in sunlight. For example, it was one of the few things that actually had success in treating the 1918 influenza. Prior to antibiotics, it was one of the most effective treatments for tuberculosis and it was also widely used for a variety of other diseases (e.g., erysipelas and mumps). Additionally, one of the pioneers of UVBI noted that low doses of externally applied UV light stimulated the general resistance of animals and human beings to infection.
Note: conversely, since sunlight is “free” and has no lobbyists to promote it, there was little incentive not to make it a scapegoat for every health problem in America.
Before long, the medical field concluded part of the value of sunlight was that the ultraviolet within it was a sterilizing agent, and a variety of UV devices were developed to sterilize things. For example, one of the most effective ways to prevent people from catching COVID-19 indoors was to expose the air to UV light and likewise, one of the promising approaches which was explored for treating COVID-19 was to safely put UV light inside the respiratory tract to sterilize the viral particles there (which was shown to work and was what Trump was actually describing during his infamous remark about putting disinfectants inside the body).
Since blood borne infections (septicemia) were a major problem, in 1927, Emmett K. Knott (who was not a doctor) decided to try sterilizing the blood by extracting it, exposing it to UV light, and then returning it to the body. Initially, when tried doing this (by infecting dogs with a lethal bacteria), he found that while the treated dogs (unlike the untreated dogs) did not have the bacteria in the blood at their time of death, they still died after about a week (from a physiologic depression and respiratory slow down).
Eventually, in 1928 an accident happened and Knott dramatically under-dosed a septic dog (he’d been irradiating their entire blood volume), after which the dog had a dramatic recovery—leading Knott to realize only a small amount of the blood should be irradiated for the treatment to work. Shortly after, Knott received a request from a doctor (and friend) whose sister was on the verge of dying from septicemia (due to an abortion) for blood irradiation. Knott consented because her infection was the same as the bacteria he’d infected the dogs with, the UVBI worked, and the woman had a complete recovery.
For the next 5 years, Knott then refined his method but did not try it on any human beings, likely due to the difficulty of finding a doctor willing to try an unorthodox therapy and the economy being in a tailspin (due to the Great Depression). Eventually, in 1933, another Seattle doctor with a septic patient on the verge of death reached out to Knott, and again UVBI resulted in a dramatic recovery.
Note: Knott details his discovery and refinement of UVBI in this article.
Knott then began traveling the country with his massive machine to promote the therapy, and beginning in 1937, successfully convinced doctors at hospitals around the country (who were highly skeptical of “quacks promoting miracle cures”) to use UVBI. As the therapy, proved itself, more adopted it, and by the 1940s, a few pioneering physicians who tested it on hundreds of patients found UVBI consistently treated a wide range of conditions such as sepsis, pneumonia (including viral pneumonias—an area which conventional medicine still struggles with), kidney disorders (e.g. nephritis), asthma, polio, botulism, rheumatic fever, and viral hepatitis.
At that time, UVBI was found to almost always work if done early in an infection, and still often have miraculous results if the patient was on the verge of death (“already moribund”), and all around greatly shorten the amount of time that needed to be spent at the hospital. Some of the data from this period can be found within this compilation:
Note: Dr. George Miley one of the physicians who had done the most work with UVBI, commented on Emmett. K. Knott’s work in 1940: “I think personally that this is one of the greatest contributions to medicine ever made by a citizen of the United States.”
By the early 1950s, UVBI was being used in approximately 50 American hospitals (including many major ones), with many doctors reporting in the medical literature that they had used it on thousands of patients and had consistently seen immediate and miraculous results from the therapy (which included countless patients with unusually severe infections that antibiotics had failed and were very close to death) alongside a complete absence of side effects.
Some of these doctors felt it was necessary to document their work and a significant body of literature had emerged, comprised of 50 papers written by 20 different authors (and published in 18 different medical journals) which covered over 3000 patients with 36 different diseases—all of which found a remarkable benefit from UVBI. UVBI in turn was promoted throughout the mainstream media (e.g., articles about this miraculous therapy could be found in The New York Times and Time Magazine).
Here for example was one such case from a physician, who between 1938-1943 had successfully treated over 400 patients collectively suffering from 35 different diseases with UVBI
If there was ever a hopeless case, it was one reported by Dr. Barrett of the brother-in-law of a New York physician. While vacationing in Miami Beach, the gentleman fell seriously ill. Dr. Barrett was called to Miami from New York to treat him because the situation was considered hopeless. Since nothing short of a miracle would help him, the attending physicians decided to try hemo-irradiation [UVBI].
The patient had a thrombosis of the cerebellar artery (blood clot in the brain), pneumonia, a bacterial infection of the blood, emboli (clots) of the lungs, a blood clot in the major vein of his left leg, a paralysis of the left side of his body and a paralysis of the left vocal cords — a hopeless and certainly terminal case.
When seen by Dr. Barrett, the patient was delirious and irrational. He had eaten nothing except Coca Cola for 11 days and had lost 45 pounds.
He was immediately treated with hemo-irradiation and had an almost instant response. After a second treatment in three days, there was further dramatic improvement. Although it took him several months, he recovered completely, gaining back his lost 45 pounds and adding on another ten.
This patient would almost certainly have died, probably within a few days, without the hemo-irradiation therapy of Dr. Barrett.
Note: the one side effect noticed from UVBI was its incompatibility with sulfonamide antibiotics, as if they were given beforehand, UVBI worked much less well, whereas if given within 5 days of UVBI, they could create significant and sometimes severe reactions (e.g., renal failure or pulmonary edema). This may also explain why patients treated later in the disease process had a poorer response to UVBI (as they would have been more likely to have previously received a sulfa antibiotic).
Market Monopolization
At this point, the American Medical Association (AMA) got involved and as they had done to many other promising therapies, attempted to extort Knott by offering to perform a study that would validate UVBI for $100,000 (around 1 million today) and to buy the rights to Knott’s device in return for Knott getting a small cut of their sales.
After Knott refused to be extorted (as did the physicians across America advocating for UVBI), the AMA decided to do their study anyway. It was overseen by a friend of the AMA director (who was designing a competing device) and which curiously, prior to it being done, JAMA (the AMA’s journal) announced was likely to fail. The study had a variety of issues (e.g., no one was allowed to inspect the machine, when the machine was returned they discovered a film had been used to block some of the UV light from reaching the blood, it only had 68 test subjects, and many of the cases were conditions UVBI was not used for. Nonetheless, no adverse events occurred, no one died (despite many having dangerous conditions) and many patients experienced significant improvement.
Despite this, the 1952 study concluded with:
We have concluded that none of our patients derived benefit from the irradiation of blood with the Knott hemo-irradiator.
Because of this “definitive study,” hospitals across America (which like now did not read the full study) quickly abandoned UVBI and became fully committed to the emerging field of antibiotics. Knott in turn stopped producing his machine (as the demand for it had dried up) and died a few years later in 1961. Additionally, the recent emergence of the Salk vaccine also eliminated the interest that had previously existed in finding treatments for polio (e.g., UVBI).
Fortunately, UVBI revived itself in Russia, the former Soviet states, and Germany discusses the various devices used in Russia). This I attribute to the fact that like America, Russia (and the former Soviet States) had a functional scientific apparatus and a daring culture, but simultaneously, unlike America could not afford to spend the extravagant amounts of money we did on medical care, and hence did not have the routine censorship of scientific ideas that threaten the medical industrial complex we see here. Rather, operating on a shoe-string budget frequently motivated them to find economical solutions for the diseases they faced. Because of this, I frequently find some of the most innovative and paradigm shifting research emerges from Russia.
Note: this paper describes some of the UVBI devices used in Russia.
While many things could be said about this hit job, I believe the most noteworthy aspect was that the exact same thing has been done to so many other promising therapies as well, where a single (clearly fraudulent) negative study immediately erases a large body of independent research which shows otherwise. For example, four promising cancer therapies developed around this time (Krebiozen, the Hoxey herbs, Rife’s frequency generator, and the Koch Catalysts) initially received great interest from the AMA, but once the inventors refused to give the AMA ownership over them, a relentless quackery campaign ensued which erased them from history (which was corroborated by a Senate investigation).
Note: in 1928, prior to all of this, the AMA had reported on UVBI as being a promising therapy.
As Pierre Kory details in his recently published book “The War on Ivermectin” this happened throughout the pandemic with many of the un-patentable treatments for COVID-19. For example, with hydroxychloroquine, the Lancet (a top 5 journal), published a retrospective trial arising from overtly false data (to the point the article was later retracted) which showed that HCQ was actually killing people and led to HCQ trials around the world being terminated to protect patient safety. In contrast, a large number of independent studies found HCQ was one of the safest and most effective treatments for COVID-19 (if it was used early in the illness—whereas all the mainstream studies deliberately used it late in the illness where it was known to have minimal benefit), and prior to COVID-19, the “incredibly dangerous” HCQ was actually considered to be one of the safest and most essential medications in existence. Likewise, it was well known HCQ’s benefit only arose early in the course of COVID-19, but many of the studies instead gave it during hospitalization and then argued it “didn’t work” and similarly, despite being explicitly instructed by the Secretary of Health and Human Services to provide an emergency use authorization to make HCQ widely available to the general public, the FDA instead only authorized it for hospitalized patients and then quickly revoked the EUA since it “didn’t work” (whereas far worse drugs like remdesivir have instead been FDA approved).
Note: similar absurdities occurred with ivermectin and with vitamin D (which for decades, has proven to be far more effective at preventing the flu than the annual flu shot).
Sadly, these are by no means isolated incidents. For example, Paul Marik (who was widely considered to be the world’s top expert in critical care) was able to repeatedly show IV vitamin C was transformative for sepsis, as, if given early (e.g., when a patient shows up to the ER), this safe and affordable therapy dramatically reduces the death rate, whereas typically sepsis is the number one cause of death at the hospital (e.g., in the first year Marik began using it, his hospitals sepsis death rate dropped from 22% to 6% and in a study he conducted, the death rate dropped from 40.4% to 8.5%). Yet, this therapy has been “debunked” because a few studies were published in top medical journals which only gave IV vitamin C late in a patient’s hospitalization (where it no longer works), and as a result it is almost impossible to get IV vitamin C at an American hospital (even if an outside physician tries to persuade the hospitalists too—something we are often called on to do) because there is “no evidence” it works.
Note: I know of a few hospitals that routinely use IV vitamin C for sepsis, and the doctors who work there have told me their sepsis death rates are very low.
Likewise, after laetrile for decades had shown promise for preventing the progression of cancer (to the point many were willing to go to Mexico for it) one of the nation's top cancer institutes eventually decided to assign one of their top researchers to study it. That researcher, through multiple meticulous experiments found laetrile caused the metastasis rate for mice with spontaneous cancers to go from 80-90% to 20%, prevented cancers from developing in the first place, shrank cancerous organs, significantly improved their animals health and well being, and was completely non-toxic when given by injection.
The institute however, received pressure from the National Cancer Institute and the FDA and opted to completely mischaracterize the data their researcher had obtained and conduct a series of fraudulent studies to debunk laetrile, using tricks such as using 1/50th of the researcher’s dose, making up a new way to evaluate cancer spread (which was never used at any time before or after), incorrectly evaluating the tumor spread, giving the placebo mice laetrile, and evaluating the spread of implanted tumors (which laetrile was known not to work on) rather than spontaneously emerging ones. The institute, along with the FDA claimed no evidence existed anywhere for this unproven cancer cure (even after a collaborative study the institute was eventually forced to perform did show a benefit) and used this to outlaw both the distribution of laetrile and future clinical trials of it.
Note: all of this came to light because one employee who was disgusted with what he saw decided to be a whistleblower (wrote a memoir about it that is eerily similar to what we saw throughout COVID-19).
The costs of each of these are huge. Sepsis for example is the third leading cause of death in hospitals and kills 270,000 Americans each year. Similarly, the primary cause of death from cancers is metastases, and many of the extreme approaches used to treat cancer are justified under the possibility they might prevent a metastasis. Likewise, COVID-19 being “incurable” cost our nation trillions of dollars and killed hundreds of thousands of Americans. Conversely, whenever an industry supported drug comes to market, it doesn’t matter how dangerous or ineffective its data shows it to be (e.g., the data for both the COVID-19 vaccines and remdesivir showed they had significant dangers and provided minimal benefit), a method will always be found to argue they are in fact extremely“safe and effective.”
Note: I also recently discussed how during the early days of AIDS, Anthony Fauci suppressed a variety of lifesaving AIDS treatments (claiming they “had no evidence”) while he simultaneously pushed a failed cancer drug that was incredibly dangerous and on the basis of a fraudulent study, made it the standard treatment for AIDS across America.
Sadly, while awareness of UVBI’s miraculous properties has now largely disappeared thanks to the AMA’s control of the media, reports of it still emerge. For example, here in 2016, Fox News discussed its long history and how it could be used for the flu:
Types of Blood Irradiation
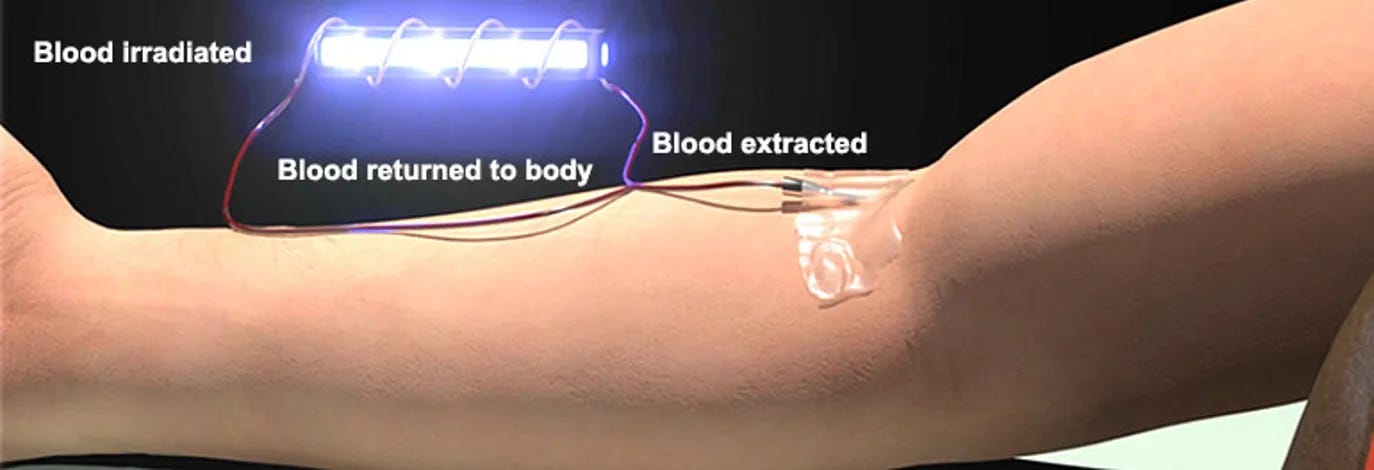
A variety of methods exist for getting light inside the body. In the classic approach, blood is removed from the body, typically diluted, then infused back into the body, and allowed to pass through light on its way back in (which in turn requires part of the IV to be made of a material such as quartz glass which UV light can pass through).
As UVBI has become more popular, German and Russian researchers (in the early 1980s) developed two alternative approaches—directly applying a laser onto a blood vessel at the surface of the body (e.g., the back of the knee at the popliteal vein or under the tongue at the lingual veins) or threading a fiber optic cable into a vessel (e.g., through an IV) and illuminating the vessel from inside. Each of these approaches (collectively known as laser blood irradiation or LBI) have been found to be relatively equivalent to each other, with the main difference being that LBI requires more treatments.
Note: to the best of my knowledge, all the LBI studies cited in this article utilized an internal form of LBI.
Additionally, a leading researcher in the field determined that LBI had a more rapid effect, and was better for bronchodilation and hyposensitization (to allergens), while UBI had a stronger bactericidal and anti-inflammatory effect. Finally, two weeks after treatment, UBI typically obtained better results for the microcirculation than LBI.
Note: this researcher also believed fasting improved the efficacy of blood irradiation.
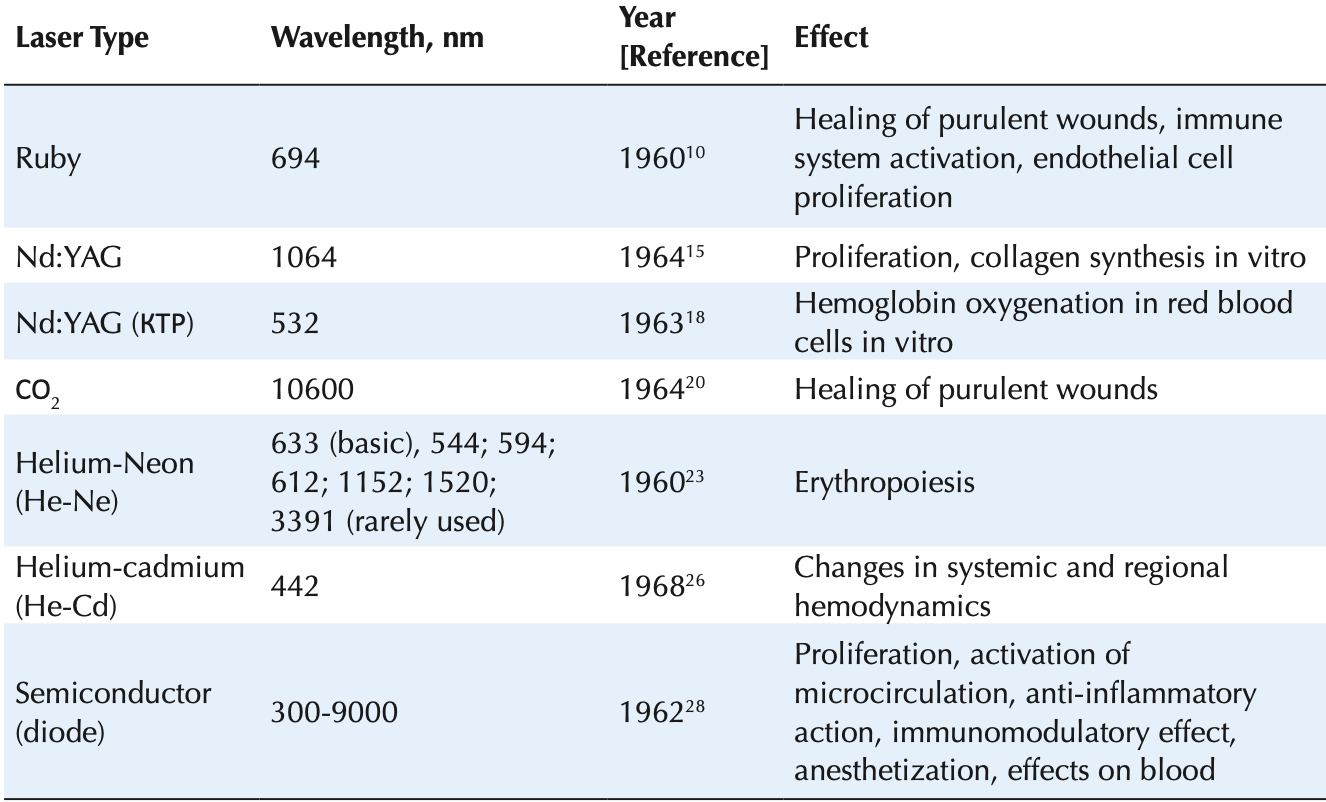
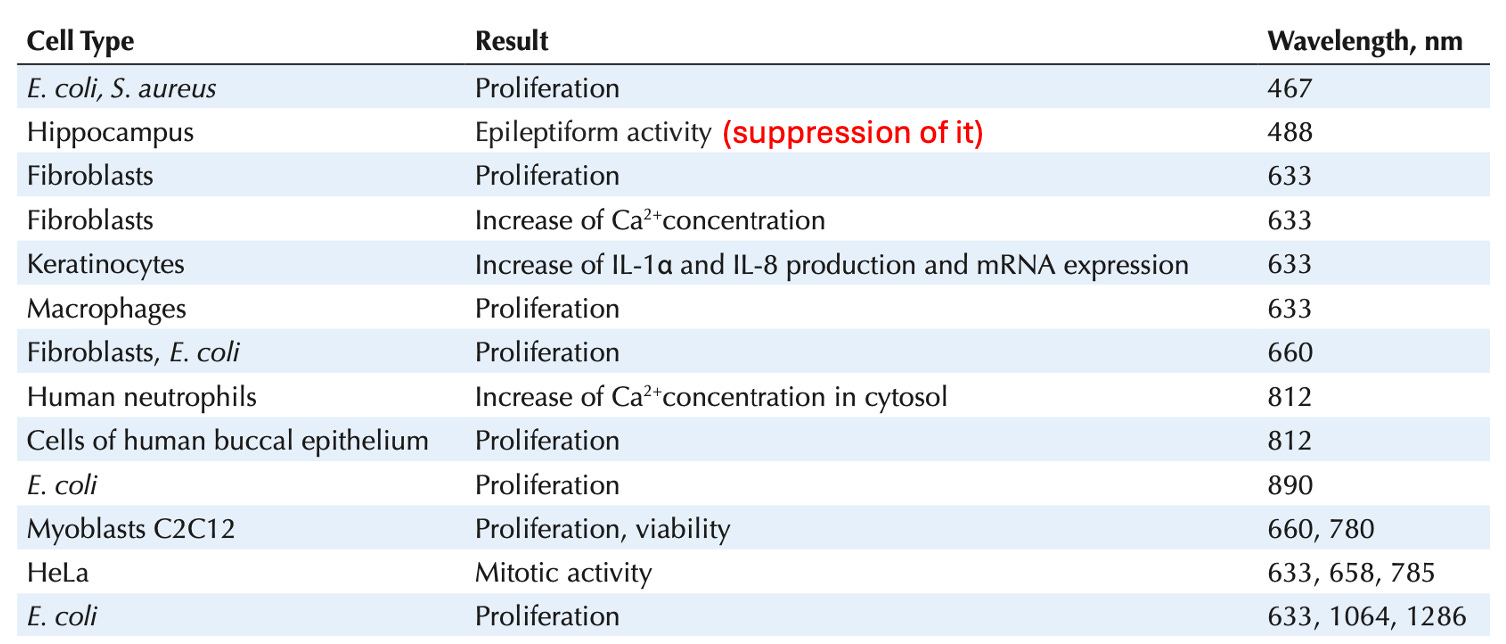
Many articles in turn have been written demonstrating that LBI works for a wide range of medical conditions and that the effects of LBI vary greatly depending on the wavelengths of light used. For example, to quote a recent review paper about the use of LBI in Russia:
Note: UV is 100–380 nm, while visible light is 380-780 nm.
Additionally:
•Unlike UVBI, LBI is difficult to obtain within the United States.
•Unlike UBVI, LBI can only have one wavelength of light applied at the same time (due to the need to maintain coherence within the lasers).
Because of that, this article will primarily focus on the data for UVBI.
Note: the cerebrospinal fluid is also sometimes directly irradiated. Additionally, a variety of different low powered (external) laser therapies have gradually caught on in America.
The major problem with these methods is that they are difficult to monetize as each UV device costs a couple thousand dollars and then with the negligible cost a few disposable parts can be used on an infinite number of people (which has disincentivized expensive research in the USA). One “solution” to this has been to combine UVBI with a photosensitizing agent (making each session approximately ten times as expensive) and call it extracorporeal photochemotherapy. In turn, a significant amount of data exists showing ECP (a widely used therapy) effectively treats a variety of conditions such as:
•Cutaneous T-Cell Lymphoma (which it is an FDA approved treatment for where it costs around $50,000-100,000 for a treatment series).
•Graft vs. Host disease1,2 (a form of transplant rejection).
•Lung and heart transplant rejection.
Note: there is also some evidence ECP can be used for a variety of autoimmune conditions such as psoriasis, scleroderma, atopic dermatitis, epidermolysis bullosa acquisita, lichen planus, lupus, pemphigus vulgaris, pemphigus foliaceous, scleromyxedema, rheumatoid arthritis, lupus erythematosus, nephrogenic systemic fibrosis (including severe cases that did not respond to other treatments),1,2 along with other areas such as carbon monoxide poisoning.
UVBI Research
UVBI researchers have identified over 200 journal articles on the use of UVBI and LBI published between 1934 and 2020, a third of which can be viewed online. For those that cannot be viewed online, they will be referenced with a number that corresponds to their citation in this companion article. Additionally, as these studies consistently found a complete absence of side effects from UVBI (or LBI), for brevity, for the most part, their safety will not be included in these summaries.
The conditions that the evidence of UVBI’s efficacy for which will be discussed in this section are as follows:
•Bacterial Infections (e.g., sepsis, septic abortions, osteomyelitis, meningitis, tuberculosis, typhoid fever, and a variety of common infections).
•Viral Infections (e.g., pneumonia, shingles, hepatitis, severe COVID-19, long COVID, polio, AIDS).
•Cardiovascular Disorders (e.g., heart attacks, angina, peripheral arterial disease, intermittent claudication, Raynaud’s, thrombophlebitis, high blood pressure, pulmonary hypertension).
•Autoimmune disorders (e.g., rheumatoid arthritis, asthma, eczema, multiple sclerosis, transplant rejections).
•Abdominal Conditions (e.g., liver, biliary and gallbladder diseases, pancreatitis, disseminated peritonitis, kidney diseases).
•Surgery (e.g., preventing post-operative complications such as infections or pneumonia, reducing the death rate, accelerating recovery time, and treating postoperative ileus or burns).
•Obstetrics and Gynecology (e.g., male and female fertility, preventing miscarriages, preeclampsia, having healthy babies, polycystic ovarian syndrome, pelvic inflammatory diseases).
•Neurologic and Psychiatric Disorders (e.g., depression, schizophrenia, migraine headaches, poor cerebral blood flow creating symptoms like tinnitus, a foggy head or insomnia).
Note: UVBI is also very safe. For example, a 1990 study reviewed 2380 UVBI sessions for side effects. It found 1.3% experienced an issue due to IV placement or manipulation, while 12 (0.05%) experienced a direct side effect (4 rigors, 2 low blood pressures, 3 nasal bleeds, 1 hypoglycemia, 1 bronchospasm, and 1 urticaria), leading them to conclude intramuscular injections should be avoided within 2 hours of UVBI, and that carbohydrates may need to eaten after UVBI sessions.
Bacterial Infections
Dr. Rebbeck has shown that ultraviolet blood irradiation therapy is effective after the sulfonamides have failed. This has been my experience. We have given more than 200 irradiations to 100 patients. These patients have been given a thorough course of sulfonamides with no success. I have seen angry, edematous infections subside in six to eight hours following blood irradiation therapy and in 24 hours they'd be almost gone.—Dr. Roswell Lowry (Cleveland, Ohio)
UVBI originally came into use after its early pioneers observed its remarkable efficacy for a variety of severe infections. For example, in 1942, Dr. Miley reported on 103 consecutive cases of acute pyogenic (fever producing) infections that were often quite severe (e.g., septic) at Hahnemann Hospital in Philadelphia. Results of recovery were 20 out of 20 for early infections, 46 out of 47 for moderately advanced, and 17 out of 36 of those who were moribund.” In short, they also found UVBI would treat infections throughout the body, including suspected infections (where signs of infection were present but it could not be identified).
Note: frequently alternative therapies are only used as a last resort in cases where a patient is otherwise expected to die (which in turn makes them appear less efficacious than they actually are). Additionally, these lower results are likely in part due to previous sulfa drug treatment.
As UVBI yielded dramatic results for mothers who developed severe infections from the birthing process (puerperal sepsis), which at the time was a frequent cause of death, UVBI became a popular treatment option. For example, one physician reported that over 4 years UVBI had been used for puerperal sepsis, they’d had 2,486 obstetrical patients and 0 deaths.
UVBI in turn has shown promise for a variety of bacterial infections. For example:
•Miley found streptococcal infections (e.g., strep throat, rheumatic fever, scarlet fever, acute tonsillitis, acute otitis media, and erysipelas) responded to UVBI.
•In patients who had a Staph albus or Staph aureus infection and only received UVBI, 8 out of 9 recovered (with the treatment failure existing concurrently with a bladder carcinoma). Additionally, Miley cited a case of a young adult who had a dramatic recovery from staph aureus septicemia following two UVBI therapies.
•Miley reported on 6 patients with chronic (and often severe) non-healing wounds that recovered with UVBI.
•7 cases of E. coli septicemia (which was a very dangerous condition in the 1940s) were treated with UVBI. 5 were cured, while 2 died, one from myocardial degeneration (but had a sterile bloodstream) and one from a different staph infection.
Note: the above organisms frequently cause hospital acquired infections, which has led UVBI proponents to argue that UVBI would be an effective treatment for them. Likewise, many of the most challenging bacteria (e.g., the six highly virulent antibiotic resistant superbugs) are susceptible to UVBI and have not been found to develop resistance to UVBI.
Between 1944 to 1947, a physician reported treating 631 patients with pelvic inflammatory disease (35% of which were severe cases), and found that in the severe group, UVBI fully resolved the condition for 79%, improved it for 11%, while 10% then required surgery, while in the less severe cases, UVBI had an even higher treatment success rate. When surgery was performed, if UVBI was done beforehand, the mortality rate was greatly reduced and the post-surgical morbidity decreased by 50%. Finally, in this group, there were 17 mothers with sterility due to their condition (all of whom then became pregnant) and 5 with threatened abortions (who were able to save the pregnancy).
Note: he also published a 1949 report on using UVBI in surgery.
Likewise, a 1990 Russian study of 23 cases of this disease found that UVBI plus standard drug therapy caused patients to recover much faster than controls who only received drug therapy (12 days versus 21 days).2
Note: more modern research (i.e., this and this Russian study) have also found UVBI reduced complications from C-Sections.
•126 patients with septic abortions (66 of which occurred outside of the hospital) were split into three 42 person groups. In the group that received 3-10 UVBIs, there were 2 cases of septic pyremia (fever) and 14 deaths, in the group that received UVBI plus hemo-absorption there were 6 deaths, and in the group which received standard drug treatment, there were 6 cases of septic pyemia and 23 deaths.
•40 patients with septic abortions were given UVBI, with all experiencing remarkable and consistent recoveries. An earlier article by this author detailed similar results in 21 patients.
•25 premature babies in the neonatal intensive care unit for severe infections received UVBI. 17 improved, 8 did not, of whom 6 died. Another study of 52 critically ill infected newborns found 28 improved after 3 UVBIs, and that UVBI had an oxygenating and detoxifying effect for them.
•55 patients with chronic osteomyelitis received 1-3 LBIs and were found to have had improved immune function and outcomes in subsequent surgery.4 Likewise Miley (as shown in the PDF of early UVBI data I attached above) treated 16 cases of acute febrile myelitis, and had 15 recover.
•40 infants (up to 3 years old) who were suffering from acute pneumonia or pleural infections received UVBI and were found to have a much lower death rate and recover 1.7 times faster than 25 historical controls. Another study of infants with acute purulent destructive pneumonia found that UVBI corrected their immune response, created a large reduction in their course of treatment and considerably reduced their death rate. A third study of 56 infants under one with acute pneumonia who received UVBI and drug therapy found, when compared to 45 controls only receiving drug therapy, their temperatures and rapid heartbeats dropped faster, their blood counts had a greater improvement, and their hospital stay was reduced by 24%.
•10 young males with moderate acute pneumonias (and 20 controls) who received UVBI were observed to have a reduction in lipid peroxidation and an improvement of antioxidant production.
•50 patients with severe skull or brain injuries and concurrent pneumonia received 6-8 UBI treatments alongside antibiotics. Compared to 25 controls, their mortality and hospital stay were reduced, and an improved immune response was seen in their T-cell, IgA and IgM levels.
•182 patients with multiple coexisting microbial infections (e.g., pneumococcus, staphylococcus, and streptococcus) received UVBI. When compared to 90 control patients, the treatment group recovered 5 to 7 days faster, had fewer complications, and experienced a reduction in fibrinogen to normal activation of anticoagulatory and fibrinolytic elements. Additionally, those initially diagnosed with anemia had a 30.7% increase in their red blood cell count.
•18 children with meningococcal infections received LBI treatments. Researchers observed improvement in microcirculation, infective-toxic shock disappeared, and hemodynamic status improved 2-3 days earlier than with standard therapy.
•86 patients with destructive tuberculosis received UVBI and antibiotics (while 136 controls only received antibiotics). Within 3 months, 100% of the UVBI group was disease free (compared to 58.8% of controls), 89.5% of them had their lungs recover (compared to 38.2% of controls), and their hospital stay was reduced by 48 days.
•A 1995 study of 222 patients with newly diagnosed destructive tuberculosis found that combining ultraviolet blood irradiation (UVBI) with antibiotics reduced hospital stays by 48 days compared to antibiotics alone. Within three months, 100% of the UVBI group ceased bacterial discharge, and 89% showed no further lung destruction, compared to 59% and 38%, respectively, in the antibiotics-only group.
•88 patients with tuberculosis received low dose UVBI and compared to controls. The 31.9% of the UVBI group had significant improvement, 47.8% partial improvement, and 20.3% no improvement (with many of the non-responders having cases that were far more difficult to treat).
•In a clinical trial, 119 tuberculosis patients received a combination of LBI and drugs and were observed to have a cessation or diminution of coughing, reduction in mucus, improvement in pulmonary function, and stabilization of their lymphocytes.9
•A study of 44 teenagers suffering from acute and progressive tuberculosis found that the 25 who received LBI (intravenously) alongside antibiotics recovered 1.5 - 2 months faster, had a less severe illness, and had less residual lung damage.
•A randomized control trial of of children and teens with infiltrative pulmonary tuberculosis, found that giving UVBI in addition to antibiotics found that it made them eliminate TB twice as quickly, be less ill, and better tolerate the tuberculosis antibiotics.
•A study of patients with chronic tuberculosis and chronic obstructive bronchitis found that UVBI significantly decreased their tuberculosis bacterial count, halved their bronchitis symptoms and improved many other aspects of it (e.g., their ESR, forced expiratory volume, white blood cell counts)
•A three-arm retrospective study on typhoid fever determined that UVBI alone was more effective than UVBI plus antibiotics and much more effective than antibiotics alone.
•A 1991 study of young children with destructive pneumonia found that it improved the immune response to the infection, reduced excessive inflammation, caused a 1.7-fold reduction in recovery time, and significantly reduced the death rate from this disease.
•A 1990 study of 50 patients with severe head or neck injuries and pneumonia found UVBI is an effective treatment for reducing the death rate and length of hospital stay
•A 1990 study of 120 children with sepsis found UVBI improved metabolic function and reduced mortality.
•A 1991 study of terminal kidney failure patients with inflammatory infections found UVBI improved their illness, stimulated immunity, and normalized blood parameters.
•A 1992 study of 1527 patients with different forms of erysipelas (a skin infection) found UVBI rapidly treated the disease and prevented complications or recurrences.
•In the early 1940s, Miley and Rebbeck treated 72 patients with peritonitis (infectious inflammation of the abdominal cavity), with UVBI. These patients consisted of 40 with general peritonitis, 20 with abdominal abscesses and 12 females with multiple pelvic abscesses and severe pelvic peritonitis, 29 of whom had failed sulfa therapy. Of the 43 with moderately advanced peritonitis, all recovered, while of the 29 who were moribund, roughly two-thirds recovered (while two of those who died also had significant carcinomas). On average the early stage of recovery took 34.5 hours and the complete recovery took 81.75 hours. Lastly, UVBI was observed to rapidly resolve paralytic ileus in these patients.
•A 1989 study of 199 patients found UVBI halved the death rate from peritonitis.
•A 1990 study of 60 patients with peritonitis found that UVBI halved the death rate, reduced their hospital stay by 2.6 days, and improved their leukocyte index and after three days increased T-lymphocytes by 63%.
•A 1997 study of 35 patients with disseminated peritonitis found approximately 3 UVBIs reduced the mortality rate from 27% to 11.4% (in comparison to 37 controls receiving standard therapies). The UVBI group also had a 60% increase in their T-cells and a 36.5% decrease in their circulating immunocomplexes.
Additionally, in more modern times, many have found UVBI is very helpful for Lyme disease.
Viral Infections
Viral infections have always been an area where medicine struggles (e.g., many types of pneumonia are viral). Since the start however, UVBI has been recognized to be highly effective in these infections:
•Miley documented 79 consecutive cases of viral infections treated with UVBI in patients at all stages of illness. 98% recovered, including 8 of the 9 that were near death. Additionally, he reported on 6 patients with shingles, all of whom had it disappear and then never come back.
Note: the previous year Miley documented 445 consecutive acute pyogenic (fever producing) infections treated UVBI which found UVBI to be a rapid, efficient, and non-specific control of all types of acute pyogenic infections. This included 74 virus or virus-like infections. Another physician who performed 2,500 UVBIs shared that he’d had similar results to Miley.
•In a later unpublished summary of their decades of work on UVBI, Miley stated that a single treatment with UVBI was typically sufficient to bring about recovery from viral pneumonia.
•43 patients with acute viral hepatitis (3 of whom were chronic) received UVBI (averaging 3 treatments). All experienced a rapid improvement in their acute symptoms (e.g., nausea, pain, or jaundice), with 27 experiencing marked improvement in 3 days or less, 11 in 4-7 days, and 5 in 8-14 days. No patients died.
Note: UV light has been found to cause a 10 million fold reduction in hepatitis B virus in human blood.
•26 patients with Hepatitis and Cirrhosis of the Liver received LBI and were compared to 20 controls who received the standard drug treatment, with no one dying and 88% experiencing good results (compared to 60% of the controls improving and 2 dying).12
•A recent 2015 American trial gave 9 patients with hepatitis C three sessions of five UVBIs over a 22-week period. It found the viral load was reduced by 21.5% at 20 weeks, and reached its lowest (44.9%) at 37 weeks. Additionally, at 20 weeks, their direct bilirubin declined by 41.1%, their AST by 15.2% and their ALT by 19.3%. Additionally, two patients showed marked improvement in their concurrent psoriasis (a condition which also responds to UVBI) at the conclusion of the trial.
Note: this authors of this study also reported their device has “demonstrated efficacy in as yet unpublished animal studies on influenza and simian immunodeficiency virus infection.”
•A study of severe cases of severe viral sinusitis in children found UVBI to be highly beneficial for them.
•27 patients with eye conditions such as herpes zoster ophthalmicus (shingles), iridocyclitis, uveitis, retro-bulbar neuritis and keratitis received UVBI. Controls remained in the hospital for 30.8 days, whereas UVBI were discharged in 17.5 days.
•During the pandemic, 35 patients and 35 controls with moderate or severe COVID-19 underwent UVBI in a Russian hospital. The UVBI group experienced a 7 day reduction in their total hospital stay (going from 18±7 to 11±9 days), with 85% of those in the UVBI plus standard care recovering within 7 days, whereas only 60% of those in the standard care group recovering (and hence needing additional therapeutic interventions), with one dying in the placebo group and none dying in the treatment group. Additionally, relative to the control group, the UVBI group experienced a significant improvement of their CRP levels and the CT imaging of their lungs (e.g., the authors provide CT images of glass opacities disappearing after UVBI). Finally, no adverse effects were reported. To my knowledge this was the only COVID-19 UVBI study performed in a hospital setting (e.g., in the USA there was a willing hospital but the FDA stonewalled and then blocked the research team—in essence holding UVBI to a far higher standard than Pfizer’s experimental and completely untested injectable gene therapy).
Note: a 1996 study of 9 patients in the ICU for acute respiratory insufficiency found LBI improved their respiratory parameters, normalized their white blood cell count and that none of the patients developed ARDS (a common sequelae of COVID which led to many being put on ventilators) despite being at risk for it.
•10 Patients with long-COVID symptoms received UVBI. All of them experienced a significant improvement of their symptoms, which correlated to declining D-dimer levels. Many patients fully recovered after one irradiation and no side effects were reported.
Note: many of us have also seen UVBI be very helpful for long COVID.
•UVBI has been shown to inactivate a wide variety of virus and bacteria and platelet concentrates.1,2
Polio
While Polio is also a viral condition, I wanted a separate section for it because so much of medical history is based upon the premise polio was incurable, and hence we owe an immense debt of gratitude for its vaccine. To illustrate:
•Miley reported 58 polio cases treated with UVBI. This included 7 near-death cases with Bulbar polio (polio of the brainstem), 3 of whom regained their swallowing reflex within 24 hours and one of whom only 1 died (for context, Bulbar polio had a 40% death rate, illustrated by the 2 other bulbar patients who refused Miley’s UVBI both dying). Miley also treated 6 patients with rapidly progressing polio (which typically progressed into bulbar polio or respiratory paralysis), all of whom recovered within 48-72 hours of UVBI (including those who were beginning to enter respiratory failure prior to UVBI).
Note: Miley also had remarkable results with chronic polio patients (e.g., a woman who had been on a respirator and in the seventh month of her pregnancy became the first Polio patient in California to deliver a normal infant at term).
•Another doctor (G.J.P. Barger) who had given 2,500 UVBIs reported that he’d had very similar results to Miley’s results in the 23 bulbar polio cases and 6 spinal polio cases he’d personally treated with UVBI and noted that he often had mere hours to get to the patient once consulted for a UVBI or they would already be dead. To quote Barger:
The chief pediatrician of this hospital has repeatedly stated to his medical student classes that they had fully expected the death of the first five cases of bulbar polio that they had asked me to treat with ultraviolet blood irradiation, and none of them died.
•11 children with severe bulbar and spinal polio received UVBI, with 10 having a full recovery and 1 dying. In comparison, 5 out of 14 controls died.
•A 1943 study injected polio into the brains of monkeys and then successfully treated them with UVBI.
Note: another doctor (Fredrick R. Klenner) also had a great deal of success treating polio with IV vitamin C.
AIDS
In the later 1980s (at the time when Fauci’s AZT hit the market), people were frequently dying of AIDS, but many believed AZT made the disease much worse. Hence, many people tried a variety of alternative therapies to AZT (which often were not that effective). The physicians I knew who treated those patients felt the oxidative therapies, particularly intravenous ozone and UVBI offered the best hope these individuals had, while I do not believe either was a panacea, I personally know of numerous people who would have died otherwise had they not had access to these therapies and instead essentially recovered with them.
In William Campbell Douglass MD’s book, he shared two compelling cases of individuals (including a doctor) who developed AIDS, were in dire straights, and then got their lives back with UVBI. As these testimonies were too long to post here, but I felt nonetheless had a lot of important points that should be heard (e.g., their anguish and anger towards the FDA), for those who wish to read them I posted them here.
Douglass also cited three cases in Russia, two of whom had a dramatic improvement from UVBI, and one of whom had a positive response but stopped the therapy. Finally, he cited his work in Uganda (which was in the midst of a devastating AIDS epidemic) where he started a clinic which provided UVBI and IV hydrogen peroxide and had numerous miraculous results which created a large interest in the community as many there were desperate for a cure (however at the same time, he also had patients who discontinued the protocol die).
Lastly, in their 1997 document describing everything they’d learned over 60 years with UVBI, the early pioneers of UVBI noted numerous cases of AIDS being successfully treated with UVBI.
Note: to some extent this approach has also been researched in America. For example, in 1991, a Baylor researcher found the HIV and CMV viruses could be inactivated by mixing it with a photosensitive die, and exposing it to a 630nm light source. Later, in an interview, he shared that they’d attained a 100% kill rate of HIV, CMV, measles and herpes without damaging the normal blood elements and that the other blood components (e.g., the red blood cells) did not need to be removed for this to work, something done with many of the existing (and more expensive) UVBI approaches in America.
Circulatory Disorders
“Just a couple of months ago, I had problems just walking around the mall. I would have to stop four times and rest just to go two blocks. I was told that 1/3 of patients having what I have get better, 1/3 stay the same, and 1/3 get worse, and there was nothing more that I could do. I had two UBI treatments at the clinic, and my, what a difference. I had a conference in Minneapolis last week and walked over two miles in cold weather (something that I could not do). I not only felt great, but I am also full of energy.” — Lenny
UVBI has repeatedly been shown to significantly improve a variety of cardiovascular disorders, such as cardiac ischemia (chest pain), heart attacks, poor circulation in the extremities, and congestive heart failure (e.g., see this report), and in many cases do so in severe cases that were not responding to conventional therapies (e.g., a patient with Buerger’s disease who already had 2 gangrenous toe be amputated). Likewise, many cardiovascular patients receiving UVBI (or LBI) have been observed to have improved oxygenation and rheological (flow) characteristics of their blood and improved microcirculation. Studies in this area include:
•A 1982 study gave 7 UVBIs to 70 males (56 who had previously had a heart attack) with severe angina (chest pain) who were not recovering from intensive drug therapy. Over 2-16 months, all patients had an “outstanding” improvement in their angina, 46 were able to walk 1 km per day, and 31 of the 39 who had jobs were able to return to work (along with numerous improvements of cardiovascular blood markers). These effects persisted in 38 patients over a 2-8 month observation period while 9 out of 22 followed for 10 months later needed additional UVBI.
•5-10 UVBIs were given to 15 patients with angina (chest pain), of whom 80% benefitted substantially and to 11 patients with ischemia (insufficient circulation) in the lower extremities of whom 73% benefitted substantially.
•145 men with severe ischemic heart disease received 5-10 UVBIs plus standard drugs, with 137 having a favorable response to UVBI. 92 of them had a strong response (fewer incidents of angina and being able to walk 1,000 meters per day), while 45 had a moderate improvement.
•Intercardial LBI was administered 5-7 times to 30 patients during a (severe) heart attack with no complications. In 33%, their pain disappeared (while in 22% it significantly improved), greatly reducing the need for painkillers, and in 2-3 hours, only 15% were still in intense pain (compared to 45% of those on conventional drug therapy). Additionally, blood viscosity dropped by 30%, platelet aggregation dropped by 25%, fibrinogen levels dropped by 20%, and there was a 35% reduction in general peripheral resistance alongside a normalization of diastolic pressure. Stabilization of hemodynamic levels and more rapid resolution of the heart attack occurred and the improvements were maintained for the six months of follow-up.
•24 patients received UVBI and standard drugs within 6 hours of a heart attack and 87.5% experienced an improvement of pain. Additionally, after UBI incidents of premature ventricular contractions decreased sharply for 12-24 hours (at which point another UBI was given to continue that improvement), and UBI was observed to reduce cardiac arrhythmias.
•A group of Russian doctors in one city studied 145 patients with severe blockages of coronary arteries who had previously suffered a heart attack and found 137 of the 145 significantly improved from UVBI (e.g., they had less chest pain and needed fewer medications). In parallel, another doctor reported his team had treated 256 patients with serious heart disease and found that 95% improved from UVBI, and 91% could return to the jobs they’d had to leave because of their heart condition.
•Another Russian team found 10% of those with chronic severe chest pain who received LBI then had heart attacks, compared to 70% of those who did not receive LBI. Likewise, they had an 81% success rate in treating irregular heart rates (compared to a 30% success rate in those not receiving the therapy).
•A study of 40 patients with acute coronary syndromes found UVBI normalized cholesterol levels and potentially did the same for tissue oxygen delivery.
•A double-blind study of 50 patients with Fontaine Stage II of arterial disease (e.g., pain in the legs with light exercise), found those who received 6 days of UVBI had a 360% improvement (compared to a 90% improvement in the placebo group whose transfused blood was not irradiated), while 4-6 weeks of inpatient therapy yielded a 100% improvement, and 16 weeks of drug therapy and distance walking yielded a 160% improvement. These results were confirmed by subsequent trials (although smokers and diabetics required more UVBIs). This in turn means UVBI is superior to the current treatment for intermittent claudication.
Note: regarding this trial’s placebo, research has shown that re-injecting one’s own blood (without doing anything to it outside the body) has a therapeutic effect to varying degrees.
•13 patients with acute thrombophlebitis (the first 5 of whom had not responded to drugs and therapy) received UVBI, with 12 of the 13 then recovering. In a later report, he discussed 18 consecutive patients who also all responded, although those with chronic thrombophlebitis often took longer to recover.
•A Russian team tested UVBI for arterial obstructions in the legs (something commonly seen in severe diabetes or heavy smokers) and found 8 of the 11 patients had significant improvements in their condition (e.g., much less pain and much better wound healing in the legs).
•28 patients with Raynaud’s received LBI and were compared to 30 who only received standard care. 43% had a significant improvement (compared to 33%), 50% benefitted (compared to 16.7%), 7% had no response (compared to 50%), while 1 worsened.12
•A group of doctors at an Azerbaijan hospital gave UVBI to 34 patients with challenging blood pressures (e.g., they were very high or not responding to medications) and found that after frequent UVBI treatments, they had a 30% reduction in both systolic and diastolic blood pressure along with many of their more severe symptoms (e.g., headaches dizziness and chest pains) disappearing, the results lasting for at least 10 months, and that their need for medications was drastically reduced.
•A German study of patients with peripheral artery disease found UVBI normalized their of thrombocyte functions and cholesterol levels.
•The effect of UVBI on hemodynamics was studied in patients with chronic lung diseases. UVBI was determined to create a sustained reduction in the pulmonary-vascular resistance in bronchial asthma and chronic obstructive bronchitis and improve their pulmonary hypertension.
•A 1996 Polish study gave LBI to 9 ICU patients in acute respiratory distress (one with Guillain-barré syndrome, six with multiorgan injury, one with pancreatitis and one with acid gastric contents aspiration). Despite being a high risk for ARDS, none progressed to respiratory failure (rather their lung radiographs improved), along with their blood oxygenation, oxygen pressure, carbon dioxide levels, and white blood cell counts showing a significant improvement.
Autoimmune Conditions
Since UVBI first began being used, it has been consistently observed to work for a wide range of autoimmune disorders. For example, one doctor who reported 110 UVBI cases noted that patients suffering from rheumatoid arthritis improved, remarkably, often within a few hours, and that he had a case where a patient saw him for night sweats but coincidently also had a complete resolution of her arthritis after 3 UVBIs.
Note: that doctor subsequently reported on 400 cases (e.g., infectious and rheumatoid arthritis, tuberculosis glands, chronic blepharitis, mastoiditis, uveitis, furunculosis, sinusitis, acne vulgaris, secondary anemias, asthma, bacteremias, peritonitis, thrombophlebitis, puerperal sepsis, septic abortions, and bronchopneumonia), including many that did not respond to standard therapies. Excellent results were seen, with the author highlighting nine cases where a severe illness rapidly improved.
Other data includes:
•148 patients who had Stage I-IV rheumatoid arthritis on average for 9.1 years were divided into 5 groups (1 placebo and 4 who received differing LBIs). Those in the early stages of the disease experienced significant benefit from LBI (which was also helpful in the moderate stages), while those in later stages had less of a response and were more difficult to treat (e.g., LBI could exacerbate the condition).
•In 1943, Miley reported a series of 80 “intractable” asthma patients who received UVBI every 4-6 weeks over a 4-year period. Twenty-four patients were not followed up, which left only 56 patients to document. Of these, 29 were moderately to greatly improved, 16 were slightly improved, and 11 had no improvement after a period of six to ten months. The 45 who had improved remained so for six to ten months, after an initial series of up to ten irradiations. In 1946, he reported on 160 consecutive “intractable” asthma patients and noted that after 6-12 months of treatment, 72.7% had a favorable response to treatment that lasted for years, and that the younger patients were, the greater the likelihood of a successful treatment (e.g., 92% of those under 18 definitely improved, 58% of those between 30-40 improved, 54% of those between 40-60 improved, but only 23% of those over 60 improved).
•A 1996 study of patients with steroid resistant asthma found LBI had a positive clinical effect, reduced the steroid dose for the majority of patients, reduced immune cell resistance to steroids, and reduced the activity of their monocytes.
•A Russian trial of 88 asthma patients found 90.9% of those with early stage asthma had a positive response to UVBI, while 78.9% of those with mid-stage asthma did, and 65.9% of those with severe persistent asthma had a positive response (with the responses to UVBI being more rapid than that seen from drug treatments). Responses included a reduction in difficult or labored breathing, reduced flare-ups, halving their medication needs, and a decrease or elimination of their glucocorticoids.24 In 1993, another Russian author reported that 4 sequential trials were conducted with over 500 patients, producing similar results and noting that UVBI repeatedly outperformed LBI.25
•Russian doctors reported repeatedly observing a significant improvement in eczema, provided a low dose of UVBI was used. Likewise, they found UVBI helped for leukemia provided a low dose was used.26
•A 1950 study of 5 patients with MS found two had remarkable improvements after UVBI (e.g., one was at the terminal stage and after 4 UVBIs lived a relatively normal life for some years). However, while it was implied the others had a positive response to treatment, it was not clear to me what happened to the other 3 subjects.
•A Russian trial irradiated the cerebrospinal fluid of 26 MS patients, 14 of whom had good results, and 12 of whom had no response, with the better responses (e.g., improved sensation, coordination, and blood work) being those with the less severe cases. The only side effects observed were from the lumbar puncture required to do this treatment.
•A blinded study found that UVBI before a bone graft prevents dogs from rejecting the transplant (with similar results also found in mice with bone marrow on spleen cell transplants). Similar results were obtained in rats with heart grafts and for reducing the rejection of incompatible human blood types. Many cell studies have also corroborated this (e.g., a 2012 study found UV exposure with riboflavin was a better way to prevent blood rejection than gamma irradiation).
Note: a 1988 and a 1998 review paper further discusses the research showing UVBI’s ability to prevent the rejection of foreign tissue, while a 2016 study noted UVBI does not damage red blood cell membranes.
Abdominal Diseases
UVBI has shown great benefit for gallbladder and bile duct diseases, pancreatitis, inflammation of the abdominal cavity (peritoneum), and kidney disorders.
•A 1946 paper discussed 383 patients treated with UVBI with liver and gallbladder diseases, including 264 chronic cases without gallstones, 56 chronic with gallstones, 55 cases with chronic cholangitis and hepatitis (alongside a previously removed gallbladder). The three most severe (moribund) cases recovered, 4 out of 5 of the severe cases recovered without operation, and the remaining patients had good recoveries (although some still required operations). Additionally, UVBI tended to mitigate many of the common complications of these disorders (e.g., peritonitis).
•A 1950 paper compared 110 patients with liver and gallbladder diseases who received UVBI and were compared to 226 controls who did not. The UVBI group had a marked improvement, with 2.7% experiencing excessive nausea and vomiting (vs. 33.1% of controls), 11.8% experiencing excessive abdominal distension (vs. 28.8% of controls), 15.4% having temperatures above 102° (vs. 32.3% of controls), and 0.9% dying (vs. 2.2% of controls).
•Another study compared 85 patients with acute cholecystitis to 40 patients receiving standard medical therapy, and found LBI to be significantly superior.25
•14 cases of necrotizing pancreatitis (10 had hemorrhagic pancreas necrosis and 8 were in serious condition with enzymatic toxemia) were treated with UVBI after standard therapies had failed. They had a very positive response to treatment (e.g., pancreatic enzymes dropped to near normal levels within 5 to 6 hours). In another study of 65 patients with acute pancreatitis (who received an average of 1.5 UVBIs and some of whom also had surgery), UVBI was observed to improve their appetites, reduce their accelerated heart rates and fevers, and normalize their labs.
•60 patients (47 with chronic pancreatitis and 13 with acute pancreatitis) who failed standard treatments received 5-7 LBIs. 92% had a reduction of pain and vomiting, 83% had their nausea improved, 87% improved appetite, and 83% had a reduction of belly distention. Finally, in the acute cases, the level of amylase in the urine dropped from 1826.82 ± 401.4 g/l to 52.77 ± 4.9 g/l.12
Note: early UVBI researchers found that UVBI suppressed inflammation in pancreatitis, relaxed the sphincter of Oddi, and returned amylase and lipase values to normal. Additionally other Russian studies (e.g., this one and this one) have found DMSO helps acute pancreatitis.
•2002 study of 65 patients with traumatic uveitis found UVBI made them 22.7% more likely to recover (92.9% vs. 75.7%), 76.5% more likely to have a visual improvement, reduced their hospital stay by 30.4% and made the eye inflammation take 36.2% less time to disappear. Additionally, a 1990 study found DMSO treated 93% of those with uveitis (with only 5% having a recurrence).
•12 patients with chronic kidney disease (glomerulonephritis) were treated with LBI. Their urine protein levels dropped by 52%, while in the 7 patients with hypertension, their average systolic blood pressure dropped from 180 to 145 and their diastolic from 118 to 88.12
•LBI was given to 33 patients with chronic kidney infections (pyelonephritis), 67.4% of whom had urolithiasis and 32.6% of whom had a prostate adenoma. Standard therapy (given to 17 patients) had a 20% success rate, local laser therapy (given to 11 patients) had a 57.1% success rate, and LBI (given to 33 patients) had a 64.3% rate. Additionally, LBI “[had a] bactericidal action, activated the metabolism of substances and improved microcirculation and rheological properties of the blood. It leads to the removal of all hypoxia; it affects the release of a cascade of the patient’s own central and peripheral autoregulating systems adaptation, which medical substances do not.”
•A study of rabbits with type 1 diabetes found UVBI improved blood sugars and restored lost weight (as did this one and this one), while a fourth study also found kidney function was significantly improved in those rabbits.
https://www.meddiscoveries.org/pdf/1231.pdf
UVBI and Surgery:
Given its ability to reduce infections and restore the normal function of the internal organs, it stands to reason that UVBI would significantly improve surgical outcomes. The early pioneers of UVBI quickly observed this (to the point that they found it was often wise to give UVBI prior to surgery).
For example, while discussing 6,000 UVI’s administered at his hospital, Miley noted that they had concluded UVBI should be given prior to surgery for peritonitis, and that it frequently treated a co-existing ileus (the cessation of bowel functions). Likewise, Rebbeck, another UVBI pioneer reported on its prophylactic preoperative use in infectious conditions, concluding that the technique “provided significant protection with a marked decrease in morbidity and mortality.”
After UVBI was forgotten in America, the Russians (who needed an economical way to practice medicine) adopted it and quickly recognized its value in surgery. When William Campbell Douglass visited Russia in 1991, he estimated that over 500,000 UVBIs had been performed on over 100,000 surgical patients at over 100 hospitals in Russia and the former Soviet States. The doctors consistently reported that UVBI dramatically improved surgical outcomes, and simultaneously addressed one of the most vexing complications of surgery, ileus (no bowel movements) something which often delays people’s discharge from the hospital.
Note: I was unable to find the citations for about half of what Douglass (who had a good reputation for being truthful) discovered in Russia, so I have cited his book for those items. Additionally, many of the newer UVBI studies I located and cited throughout this article were conducted in Russia, corroborating Douglas’s claim UVBI had a revival there (e.g., in 1985 the chair of a surgical department reported that they were regularly using DMSO for surgical patients and that it was greatly improving the immune response and inflammatory conditions like sepsis).
•Two surgeons at a Russian center specializing in this who used UVBI in severe trauma cases (having treated over 3,000 patients) reported that UVBI reduced the number of complications (and the need for antibiotics) by 50% for their severe trauma cases. For context, this included situations like crushed kidneys or extensive internal bleeding.
•Severe burn patients often immensely benefited from UVBI. For example, a team of Russian doctors in 1992 reported on 16 cases of severe third-degree burns (covering up to 69% of the body surface). They observed these patients improved almost immediately after receiving UVBI, their severe pain subsided, their appetite returned, they often were able to fall into a deep sleep, and their blood protein levels usually increased.26
Note: burns like these are immensely challenging to treat. Interestingly, for over a century, the complications of burns have been linked to blood clumping throughout the body (due to a poor zeta potential) and some of the most effective treatments I’ve seen for burns (e.g., negative ion therapy) all happen to improve zeta potential.
•Ukrainian doctors reporting on 173 ear, nose, and throat cases noted that many of the most severe ones they saw (e.g., sepsis from a nasal infection) rather than being fatal rapidly improved from UVBI, including in those who they could not treat with antibiotics (e.g., due to drug allergies), that UVBI doubled the ear drum’s healing speed after surgery and that when UVBI was used, they saw long term remissions (greater than three years) of chronic sinusitis. Those doctors also reported successfully treating 250 cases of endocarditis with UVBI (which is traditionally a challenging infection to treat), with 43 of them also being able to avoid a surgical repair of the heart valves, while those who had surgery had much better post-operative outcomes.26
•Doctors at a Moscow hospital reported on a series of 128 patients with intoxication (e.g., comas) from organophosphates and psychotropic drugs. They found UVBI made them recover in half the time have a 50% reduction in complications like pneumonia and be 40% less likely to die.26
•A Siberian cancer center reported on 22 patients who had colon or rectal cancer, and found that if UVBI was regularly given (e.g., 4 times a day post surgery) it:26
1. Dramatically reduced the need for painkillers (e.g., they often didn’t need them or could discontinue them within two days.
2. Only 10% developed post-operative infections (compared to 30% of those not receiving UVBI).
3. There were no cases of postoperative ileus (temporary cessation of bowel function), something which is typically one of the most common complications of these surgeries.
•Another doctor reported on 78 lung cancer patients who received UVBI prior to surgery. He found that compared to those who did not, those who received UVBI had shorter stays in the ICU, and lower postoperative complications (e.g., 11% vs. 20%), and were much less likely to die (3% vs. 5.8%). Additionally, he found similar improvements for stomach, kidney and bladder cancers.
•Another team found their rates of venous thrombosis in the legs following surgery went from 10.3% to 0% once they instituted UVBI.
•A 1990 study of 81 surgical patients with pyoinflammatory disease found UVBI greatly improved their outcomes. They also recovered 5-10 days faster, had greatly reduced complications and an improved immune response, and blood parameters improved.
•Doctors at a Russian hospital experimented with applying light inside the aorta for patients with peritonitis (a dangerous infection of the abdomen) and found that it resulted in a much better post-surgical recovery (e.g., a 35% shorter hospital stay and significantly less bowel paralysis). Another team experimented with irradiating the peritoneum during peritonitis surgery and found it dropped the death rate from 16% to 9%.26
•A team that treated 52 patients with acute intestinal obstructions requiring surgery found that UVBI resulted in a rapid disappearance of pain in the post-surgical period, easier breathing and a variety of improved laboratory values (e.g., the ESR and the circulating immune complexes).
Obstetrics and Gynecology:
Originally, UVBI (e.g., in Knott’s first case) was used to prevent sepsis in pregnant or postpartum mothers. However, one of the least appreciated benefits of UVBI is its use for mothers and their children (which to some extent makes sense as obstetricians are extremely hesitant to try anything which might harm the baby due to their liability for doing so). Fortunately, UVBI in pregnancy, like its other applications has consistently demonstrated both its safety and efficacy in a wide number of obstetric (and gynecologic) conditions.
Note: the researcher who used UVBI in pregnant patients consistently remarked on the complete lack of adverse effects on the fetus (something also reported by the one OBGYN I know of in America who uses UVBI during pregnancy). Additionally, Russian researchers who examined the question were unable to identify any signs of fetal harm or mutagenicity.
A team of Russian authors found that UVBI treated a variety of challenging fetal conditions, and helped with infections, hypoxia, and slow growth of newborns. Those authors also documented 215 women who were successfully treated for gynecological disorders ranging from adnexitis to endometriosis to disruptions in the menstrual cycle and found UVBI to have analgesic, detoxifying, and anti-inflammatory effects.
•30 consecutive patients with 38 episodes of low abdominal cramps, vaginal bleeding or premature labor (indicating they were at risk of losing their baby) received UVBIs. All had an immediate cessation of their cramps and bleeding. 21 patients who received UVBI promptly (typically within 24 hours of their symptoms beginning) then had a normal pregnancy and a healthy child. The other 8 (in 7 of whom the fetus was already dead, while in the 8th there had been a challenging marginal placenta previa) had incomplete abortions (3 passed dead fetuses after UVBI, 5 only passed placentas after treatment), which did not require surgical removal of the products of conception and had a rapid recovery without infection (whereas many women at the time died of sepsis after abortions). Finally, one woman did not have symptoms, but rather received UVBI prophylactically because she had previously had a miscarriage at 3.5 months and a stillbirth at 7 months (she in turn had a normal birth).
Note: UVBI doctors have reported that UVBI has allowed women with recurrent miscarriages (e.g., 5-14 in a row) to have successful pregnancies). I personally believe much of this is due to UVBI treating pre-existing blood stasis (e.g., microclotting).
•A German researcher using UVBI for migraines noticed that many of his patients also experienced normalization of the menstrual cycle and regained their fertility (9 out of the 30 women who had been unable to become pregnant did so after UVBI).
Note: many UVBI physicians have also helped treat infertility.
•25 men (aged 21-39) with infertility with age ranges of 21-39 received UVBI. Compared to 25 controls, the UVBI group had less oligospermia (lack of sperm) and greater sperm motility (along with an improvement in sleep and appetite). 10 pregnancies occurred in the UBI group, while six occurred in the control group.
•When UVBI was given to 119 women with polycystic ovarian syndrome, many of the common aspects of the disease improved. Specifically, 29 out of 41 with no menstruation had a regularization of their menstrual cycle, 7 of 24 complaining of infertility became pregnant, 8 of 42 complaining of hirsutism (extra hair growth) improved, 12 of 30 overweight women lost 6 – 52 pounds in 3 weeks following UBI therapy without additional intervention, and blood work showed a normalization of their hormones. Additionally, 25 out of 29 complaining of headaches improved.9
•Preeclampsia (previously called toxemia of pregnancy) is a condition which occurs during pregnancy which is characterized by high blood pressure and protein in the urine, followed by other parts of the body having trouble handling the strain they are under and then convulsions, and then in some cases, death. The early UVBI researchers in turn gradually realized UVBI was very helpful for this condition (e.g., Hochenbichler treated 100 patients, even after the onset of convulsions, none developed serious complications and all cleared completely).
Note: the cause of preeclampsia is not known, but I believe it is due to blood stasis impairing needed blood flow (particularly to the uterus) probably caused by a low zeta potential (e.g., the primary treatment for severe preeclampsia, IV magnesium sulfate, is a zeta potential improving agent).
•61 patients with preeclampsia in the 3rd trimester were treated with a high dose of LBI for 20 minutes, 7 days in a row. Compared to 30 receiving standard treatments, LBI was found to stabilize red blood cell membranes, improve microcirculation and blood rheology (i.e.., treat blood stasis), reduce hemolysis (red blood cells breaking down), increase diuresis, resolve edema, rapidly and dramatically reduced proteinuria (0.24g/l compared to 0.82 g/l), lower blood cholesterol, and more rapidly alleviated hypertension compared to the control group. Overall, 80% of LBI treatments were successful (compared to 39% of controls). Additionally, babies of LBI treated mothers had better APGAR scores, only 20% required C-sections (compared to 31% of the controls), had C-sections, and when compared to babies born to healthy mothers, had identical heights and weights.
A letter from a Russian OBGYN to a journal stated that over the last 5 years, their department had found that UVBI addressed many of the shortcomings with conventional treatments for preeclampsia, and that when 53 cases of each were compared, UVBI on average prolonged the gestation by 4.1 weeks and reduced pathological births and poor fetal conditions by 50. There was also less maternal blood loss and fetal hypoxia at birth, and the fetal birth weight was higher. Finally, UVBI improved and normalized the mother’s microcirculation, reduced or eliminated blood sludging (stasis), and eliminated the problem of disseminated intravascular coagulation (a more severe consequence of preeclampsia)
.Note: UVBI has also been used successfully for cholestasis, a condition which causes severe itching and affects approximately 1% of pregnant mothers late in pregnancy (although some estimates are higher) and as a non-toxic alternative to conventional medications mothers “need” but do not want to expose their fetuses to. Likewise, a common treatment for excessive bile in infants is externally exposing them to blue light, something that was inspired by the observation sunbathing treated it, and something John Ott (discussed in the previous article) later showed worked worked best with a full spectrum light (which a few doctors then utilized) .
Neurologic and Psychiatric Disorders
A Chinese randomized study of 58 patients with recent strokes found UVBI significantly improved neurological function, and markedly increased the activities of K⁺-Na⁺-ATPase and Ca²⁺-Mg²⁺-ATPase on RBC membranes, likely improving microcirculation and oxygen delivery to brain tissue.
•A 1988 Chinese study of 170 patients with atherosclerotic strokes found UVBI and oxygenated blood infusions caused 25.3% to greatly improve, 28.2% to have a clinical improvement, while 46.5% did not respond. Additionally, a variety of circulatory parameters significantly improved.
•A rabbit study found that UVBI reduced free radical production and improved antioxidant activity after a spinal cord injury (something DMSO has also been shown to do).
As UVBI improves circulation and autoimmunity, it stands to reason that it might also help neurological and psychiatric disorders. This in turn is the case:
•A 1995 study found LBI helped 70.6% of those with melancholy-depressive syndrome, 53.8% of those with anxiety-depressive syndrome, and 39% of those with apathy-depressive syndrome. Additionally, the frequency of adaptive reactions of a pathological type went from 52.6% to 10.6%, and a decrease in the level of malondialdehyde in plasma was observed
•Miley reported that throughout his career he often saw patients with migraine headaches. In one cohort of 12 patients with classic, longstanding migraines, UBI was given every 6-10 weeks for 1-3 years, during which time 58% of them did not experience any more migraines.
•A 1991 German study conducted a controlled trial where 21 migraines were compared to placebo. From it, he found 9.5% had a complete resolution, 23.8% had significant improvement, 28.6% had some improvement, and 38% had no improvement in their headaches, a better improvement than that seen with a placebo. In addition to this trial, the researcher continued to study the effect of UBI on migraines and concluded it benefitted 60-80% of patients.
Note: another German researcher reported similar results to the 1991 study in 1989. Additionally, since UVBI is a systemic therapy, improved headaches would often be a “side effect of UVBI” (much in the same way one common side effect of using UVBI for headaches was improving menstruation).
•One study done on schizophrenia in Russia showed that light in blood therapy influences the central and regional hemodynamics (blood flow) and has sedative, anxiolytic (lessening of anxiety), and antispasmodic effects. The amount of drugs taken and the treatment period are also reduced.
•A study evaluated 38 chronic (1-23 years) schizophrenic patients (many of whom had simple or paranoid schizophrenia) who had been on a drug regimen or electroconvulsive therapy and not responded to treatment. After a brief course of LBI, 21 out of 38 (55%) responded well with the best results seen in the depressive-paranoid group, and lesser benefits in the hallucinatory-delirious group (8 out of 19 or 41%). A reduction of delirious ideas, hallucinations and monotonous motor behavior was observed alongside an improved mood, interest in their surroundings and socialization. Some were even able to return to work. The study also noted that LBI alone sufficed for patients who were predominantly parasympathetic, whereas drugs were needed for those with more sympathetic activity. These benefits were attributed to improved cerebral microcirculation, and led the authors to hypothesize part of the benefit of electroconvulsive therapy also came from its effect on the cerebral microcirculation.
•50 sailors ages 40-60 with early-stage cerebral circulatory problems were treated with UBI. They experienced subjective improvements (e.g., heads cleared, the feeling of weight on their heads disappeared, tinnitus ceased, felt more ready to work, mood improved, and sleep normalized).
•90 patients aged 47-69 with atherosclerosis, hypertension, and venous circulatory dysfunction who did not respond to other treatments received 4-8 UVBIs. 87% had a positive response, including a full resolution of 51.2% of the neurological symptoms in the 37 atherosclerotic patients. Benefits included the disappearance or significant decrease of headaches, dizziness, tinnitus, the feeling of heaviness in the head, pain in the heart region, normalization of sleep, and in most cases these improvements were long-lasting or permanent.
Toxin Neutralization
One of the most consistent observations by the early pioneers of UVBI was it “inactivating toxins.” For example in one case, botulism, a uniformly fatal condition, was treated by Miley. The patient was in a coma and could not swallow or see. Within 48 to 72 hours of one irradiation treatment, the patient was able to swallow, see, and was mentally clear. She was discharged in excellent condition in a total of 13 days.”
Later, in an unpublished report, Miley shared that he had treated two advanced cases of tetanus with UVBI both of which did not respond to existing treatments (e.g., high dose of tetanus antitoxin or sedatives). In the first case, their hourly severe convulsions stopped, and after the second UVBI, their condition resolved. In the second case, the patient only responded to the second UVBI and then gradually recovered over the next week.
In turn, many have stated that UVBI was previously considered to be a first-line treatment for tetanus, gangrene, snake venom poisoning, endotoxins released by bacterial infections (e.g., during sepsis), and rabies infections. I’ve tried to verify this but have only come across anecdotal reports from colleagues who did one of these or non-specific discussions about it in the literature.
However, some literature exists showing that when these toxins (e.g., snake venoms) are exposed to UV light outside of the body, they are inactivated and much less potent once injected back into animals. As such, it’s possible that UV either changes the shape of a toxin enough that it no longer quite fit its molecular target, or that UVBI counteracted the harmful effects of the toxin (e.g., by improving circulation). Sadly, this remains one of the least studied aspects of UVBI.
Note: as mentioned above, the numerical citations correspond to the references here.
Other Conditions
•A 1951 study found UVBI improved 15/18 cases of bursitis and calcified tendonitis.
Summary of Evidence
Unless you’ve worked in the medical field, it’s hard to even begin to appreciate how paradigm shifting a therapy with this type of data is (or how many existing therapies would no longer be commercially viable if UVBI entered mainstream usage within the USA).
More remarkably, this is just some of the data that’s accumulated (UVBI was gradually found to be effective for many other conditions). For those interested in learning more, I would suggest studying this spreadsheet, which has compiled some of the existing UVBI and LBI scientific literature, this Russian book on LBI, and this book and this book by two of the top experts in the field of UVBI.
Finally, in 1997, the pioneers of UVBI completed this (unpublished) report, which details the wide range of conditions UVBI works on.
Vasogen
As ECP’s success shows, one of the major barriers to UVBI is that, like ozone therapy, it’s not patentable, and hence, it cannot justify the immense amount of money needed to conduct the costly clinical trials and lobbying necessary for FDA approval. In the 1990s, a Canadian company, Vasogen, attempted to solve this dilemma by creating a device that mixed ozone, UVBI, and heat within its proprietary device and then injected it directly into the gluteal muscle.
This proprietary approach (which was deemed “irrational” by a leading ozone researcher) performed significantly more poorly than the other methods of utilizing these therapies (e.g., a blood transfusion of irradiated or ozonated blood), but nonetheless still produced remarkable results, resulting in Vasogen raising 225 million dollars from investors, and conducting more than 60 laboratory and clinical studies over an 8-year period. Vasogen in turn was able to demonstrate the safety of their approach, secured over 24 patents for it (e.g., to treat a variety of diseases) and published a successful Phase II trial for the treatment of chronic heart failure and peripheral vascular disease.
Note: those uses included inflammation and autoimmunity (e.g., allergic reactions, MS, rheumatoid arthritis, lupus, scleroderma, myasthenia gravis, IBS, or transplant rejections), improving circulation and the health of the endothelium (e.g., Raynaud’s, peripheral vascular disease, skin ulcers and congestive heart failure), surgical preconditioning, chronic pain conditions, chronic lymphocytic leukemia, and complex disorders such as Lyme and chronic fatigue.
This brief presentation summarizes the benefits Vasogen demonstrated for a variety of circulatory and autoimmune conditions:
Unfortunately, due to a poorly designed Phase III trial for heart failure (which had benefits but failed to meet statistical significance on its endpoint), Vasogen went bankrupt and few now are aware the company ever existed or that the costly required Phase I and Phase II studies for UVBI have already been done.
Note: pharmaceutical drugs with equivalent (or worse) results than this Phase III trial routinely receive FDA licensure.
Additionally, in 2015, another company (AVIcure Bioscience) completed and published a phase II safety study for UVBI, and in 2019, published a successful phase III clinical trial for UVBI. In both trials, safety was seen for all patients and efficacy was seen in the majority of them. Unfortunately, these studies had studied the effect of UVBI on a chronic hepatitis C infection, and at the same time they were being conducted, after decades of waiting, effective pharmaceutical treatments for hepatitis C hit the market and hence eliminated the interest in alternative therapeutic approaches for hepatitis C (which in many ways is similar to the newly developed antibiotics eliminating interest in using UVBI for severe infections almost a century ago).
Lastly, a related treatment, known as photopheresis exists, where blood is taken out of the body, the white blood cells and platelets are separated from the rest of it, mixed with a photosensitizing agent (methoxsalen), exposed to UVA light, and then infused back into the body. This therapy was originally approved by the FDA to treat cutaneous T-cell lymphoma (where it has minimal side effects), but has since been demonstrated to treat a variety of severe autoimmune conditions.
Remarkably, despite all of this evidence and its widespread usage throughout the world for almost a century, UVBI is still often referred to as a “fringe” or “pseudoscientific” therapy that has “no evidence,” which in my eyes illustrates why those terms are so meaningless.
Note: the key requirement of the 2018 Right to Try Act is that a Phase I safety study has been completed.
UVBI Physiologic Effects
Note: the most detailed paper I’ve found on the effects and proposed mechanisms of UVBI was written by a Harvard Professor who is a leading expert in the fields of photomedicine and photobiomodulation.
Almost everyone who has worked with UVBI has noticed the following occurs:
•A marked increase in the venous oxygen and the oxygen carrying capacity of the blood. For example, in 1939, Miley studied the effects on venous oxygen levels after 97 UVBIs and found a 58% increase after 10 minutes, a 9% decrease after 30 minutes, and a 50% increase one hour to one month after treatment.47 In 1970, another team found an overall 25.6% increase from UVBI.48
Note: at the time it was not possible to measure arterial oxygen levels, but later research found that they increased as well.
•Toxins were neutralized and “toxic” conditions were resolved.
•A rapid increase in the pinkening of the skin occurring within a few minutes of irradiated blood entering the system. Within a few minutes, approximately 75 percent of those receiving ultraviolet blood irradiation will have this dramatic “pinking up.” It may persist for more than 30 days, and it is usually accompanied by a feeling of well-being. Its appearance was typically regarded as a favorable sign in whatever disease is being treated.
•If the patient was cyanotic (blue), the cyanosis resolved. This effect was particularly dramatic in patients near death and often happened in a few minutes.
•Microcirculation would improve and the rheological (flow) properties of the blood would improve.
•The number of red cells, white cells, and platelets in the blood often increase following irradiation with ultraviolet light. However, if blood cells were excessive, their numbers would instead drop.
•Abnormal vital signs (e.g., excessive heart rate, fast respirations, or high blood pressure) would normalize. This included severe fevers (e.g. 108-109°) rapidly dropping.
•A rapid reduction in pain (e.g., in the muscles or head).
•Normal function of the autonomic nervous system would be resumed. This could, mean something that had temporarily stopped functioning regaining its normal function (e.g., a paralyzed bowel regaining peristalsis within 12 to 24 hours of UVBI), or an overactive function (e.g., airway constriction) decreasing. Likewise, cramps would stop but never be triggered by UVBI.
•If underactive, the immune system would be mobilized to eliminate an infection, while if overactive (e.g., in an autoimmune condition) it would be quieted down.
•Other abnormal blood work (e.g., high cholesterol, an elevated erythrocyte sedimentation rate, low calcium, elevated uric acid, or high blood sugar) would also normalize. UVBI was also thought to catalyze the formation of the active form of vitamin D.
•There was a cumulative effect with each treatment building on the previous one.
•The action of UVBI could be immediate, somewhat delayed, markedly delayed, or protracted.
This myriad of benefits in turn suggests that UVBI is somehow able to reactivate the body’s innate ability to regulate itself and heal, and that many of these benefits are a consequence of that ability reactivating. It was for that reason that the first half of this series focused on making the case that sunlight is an essential nutrient and provides a myriad of physiologic benefits provided it can get inside the body.
Note: the pioneers of UVBI believed that those who had the greatest response to UVBI were those who either could not properly absorb sunlight or were lacking sufficient exposure to it (and sadly, both of those apply to many members of society now).
Zeta Potential and UVBI
During my career, I would occasionally come across cases of someone who appeared to be critically ill and on the verge of death then have an immediate and profound response to a treatment where they stabilized within minutes. In those instances, I typically noticed that they would transition from having highly unstable vital signs (e.g., fast breathing, low blood oxygenation, and irregular heart rate) to those vital signs rapidly normalizing despite them having not received a treatment directed towards any of them.
As a response this rapid is exceedingly unusual for critically ill patients, I put a lot of thought into why this might be happening, and eventually concluded that a functional circulatory obstruction resolving could explain it (for example, when there isn’t enough blood in the body, the heart will beat faster to compensate for this lack of blood volume and if there isn’t enough blood reaching the periphery it will become oxygen starved).
Once I learned about the zeta potential concept (that poor electrical charges would cause substances in fluid to clump together and partially solidify the fluid), these observations began to make sense, as if blood is in a state where it’s clumped together (which is what occurs in a state of poor zeta potential) it can’t get to where it’s needed, and conversely, if the zeta potential of the body changes, there will be a rapid change in the body’s circulation without the need to add a significant amount of supplemental fluid into the body to accomplish this effect.
Note: high blood pressure is often due to an impaired zeta potential, however the changes in blood pressure which result from addressing zeta potential are normally not as rapid or dramatic as what occurs with the other vital signs.
Typically, to improve zeta potential, you either need to add more negative charges to the body or eliminate positive charges which are causing fluids to clump together. One of the most rapid ways this can be done is by directly neutralizing pathologic positive charges, and I in turn believe the reason why oxidative therapies (e.g., ozone or chlorine dioxide) create immediate and dramatic improvements is because they (or their secondary metabolites) are oxidizing a harmful positive charge carried by a virulent infection (e.g., chlorine dioxide originally came into use after its discover noticed it caused a dramatic improvement in malaria—a disease which exerts much of its pathology through clumping blood together).
When COVID-19 began, once I read the early reports of the illness, I began to suspect a significant degree of its pathology was zeta potential mediated, as I saw:
•Many clinical signs or rapid and extreme fluid stagnation in the body (hence why the early variants often made people critically ill)
•“Paradoxes” which could only be explained through a zeta potential model (e.g., patients with a critically low peripheral blood oxygenation subjectively being moderately well—something I believe could only be explained by blood clumping together in their periphery and hence giving an artificially low blood oxygenation reading in the finger where it is typically measured).
•Patients on the verge of death having sudden and miraculous improvements immediately after receiving a therapy that would improve zeta potential (e.g., ozone which oxidizes the spike protein’s strong positive charge) was given to them.
Note: I also learned of cases where a similar dramatic improvement in the vital signs occurred following ivermectin administration. I then located a paper showing that the COVID spike protein adversely affected zeta potential, caused blood to clump together, and that ivermectin antidoted this clumping.
In turn, since the vaccine mass produces the original COVID spike protein, it also has a significant adverse effect on the physiologic zeta potential. A large part of my mission over the last few years has been to bring awareness to this concept as it is often critically important for those who have been injured by the COVID vaccines.
If we then take a step back and look at the effects of UVBI, we notice a similar dramatic improvement often occurs (e.g., many early researchers noticed UVBI would rapidly improve blood oxygenation, blood perfusion and irregular heart rates, which they in turn ascribed to UVBI having a “detoxification effect”). Likewise, since the UVBI process requires first drawing blood and mixing it into a saline back (before it is then transfused back into the body) UVBI gives you many opportunities to observe the zeta potential of your patient's blood. In turn, from having done many UVBIs, I’ve noticed that blood from the sickest patients typically has the worst zeta potential (being dark and likely to quickly settle at the bottom of the saline bag—which is essentially what the erythrocyte sedimentation rate test evaluates), and that the improvements seen from UVBI often correlates to a seeing improvement of their blood’s sedimentation rate when subsequent UVBIs are done.
Note: UVBI typically requires mixing an anticoagulant agent with blood when it is withdrawn from the body (originally sodium citrate was used, and then at some point after heparin came into use in 1937, heparin was used instead). Both of these agents will improve the zeta potential of the body, but in my opinion, too little of them are given through UVBI to create the system shifts in zeta potential observed from blood irradiation.
Furthermore, in addition to the clinical observations, there is some supporting evidence that UV improves zeta potential. For example, decades ago, Ott directly observed UV light rapidly eliminated blood sludging within red blood cells:
Likewise, I consider this observation from Dr. E. W. Rebbeck, one of the pioneers of UVBI (who regularly used it on hospitalized patients in Pennsylvania):
In many instances we were able to convert a greatly disturbed micron picture to normal. For instance, a picture of 15-20 chylomicrons clumped together with great variation in size and shape and no Brownian [random] movement (the dancing motion of minute particles suspended in a liquid), often changed to normalcy after five to fifteen seconds [of] exposure to ultraviolet. The normal picture would be that of no clumps, good Brownian movement and all kinds of chylomicrons approximately the same size (about 1/2 micron) and shape.
The unclumping he described is exactly what happens when zeta potential improves.
Note: Gerald Pollack has argued that Brownian motion (something which still has no solid explanation) is due to liquid crystalline water forming around particles in water.
Additionally, throughout the UVBI literature, I’ve repeatedly seen investigators note that UVBI improves the erythrocyte sedimentation rate (ESR), a metric which was originally created by researchers investigating the blood clumping phenomena, and as far as I know is the closest correlate to zeta potential in conventional blood work (although it has a variety of artifacts which prevent it from being a perfect correlates to the existing physiologic zeta potential). Likewise, many have noted that UVBI reduces the viscosity of the blood (another surrogate for its zeta potential) or that it directly reduces blood sludging (which is the closest equivalent to improving the physiologic zeta potential).
Note: I have come across a variety of mechanisms which could explain why UV improves zeta potential. As each of them is theoretical, I felt it was more appropriate to share that the change occurs rather than share a mechanism I am not confident in. Likewise, some of the improvements in circulation could come from things besides a change in zeta potential (e.g., relaxation of the peripheral nervous system, improved mitochondrial function, nitric oxide release, or the formation of liquid crystalline water).
How UVBI Works
In many cases, a great discovery is due to sheer luck accompanying a mistaken premise. For example, the first antibiotic was developed by mixing a substance known to be toxic to bacteria (arsenic) with a dye that stained bacterial cell walls under the theory it would selectively target bacteria rather than the body (with almost all the attempts failing). After decades of attempts were made to replicate this approach, another dye that functioned as an effective antibiotic was found, but before long it was discovered that the antimicrobial agent was not the dye itself but rather a colorless metabolic product of it, sulfanilamide.
Similarly, UVBI was originally developed under the belief that it would sterilize the bloodstream. Once it was determined that it did not, the field instead concluded that it killed the microbes present within the directly irradiated blood, in effect creating a functional vaccine that primed the immune system to go after the microbes in the rest of the body. However, as recent research has shown, this belief also appears to be incorrect.
The largest obstacle for UVBI has been the fact that our culture “needs” mechanisms to believe something works, and in the case of UVBI, while mechanisms for certain very specific aspects of it have been established (many of which are detailed here), there is no explanation for the systemic effects it (or ECP) produces.
Note: a 2020 review discussed the various mechanisms underlying UVBI’s efficacy in viral infections, highlighted that viruses are much more sensitive to UV than normal cells, and that at lower doses, rather than kill immune cells, it simulates their ability to neutralize pathogens (while simultaneously reducing their ability to attack normal tissue). Likewise, pulses of visible light have been shown to destroy viruses without damaging normal cells.
As such, I will share what I believe are the key mechanisms (many of which were discussed in more detail in the first half of this series):
•Blood conducts light. Because of this, if a small portion of it is irradiated, UV will rapidly fill the inside of the body. I originally suspected this because I would see UVBI create instantaneous changes within the body and noticed those changes would disappear the moment I turned off an external UVBI machine (and return once I switched it on), a change which was much faster than irradiated blood could enter the body after being exposed to an external light source. Later, I learned that blood cells have been repeatedly shown to emit light after being exposed to UV.
•The body is extremely sensitive to low amounts of UV light, such as that emitted by blood cells exposed to UV. Additionally, many parts of the body have receptors which are designed to be ultra-sensitive to very specific light wavelengths (e.g., those we depend upon to regulate the vital physiologic rhythms the body utilizes to heal itself). As such, the small amount of UV light that gets conducted throughout the body can have a large physiologic impact.
•Blood has been shown to absorb over 10 times as much UV light as visible light (e.g., at least 15.8% of 305nm light is absorbed).
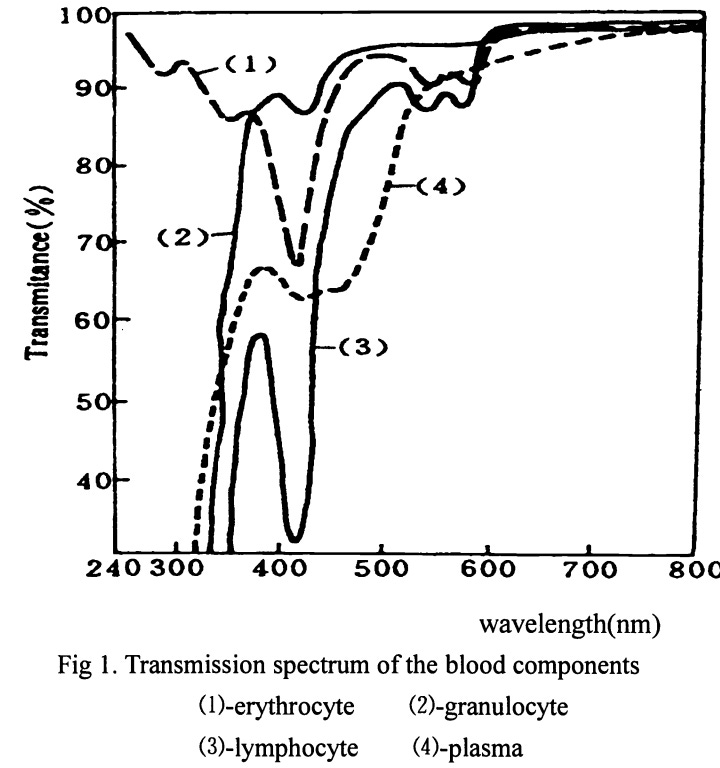
In parallel, cancerous white blood cells (in CLL) were found to be hypersensitive to damage from UVC light (whereas normal while blood cells were unaffected with ten times the dose) and could not repair that damage.
•Cells frequently enter a dormant state after being exposed to stressors (known as the cell danger response). One of the primary signaling agents that “wakes them up” is the emission of ultra faint UV photons (which amongst other things have been shown to make cells grow and begin dividing).
•UVBI improves circulation by fixing the zeta potential. It may also improve it through nitric oxide production and vasodilation.
•UVBI does something which “wakes” dormant cells up. While I believe in some cases this could be accomplished by giving them a signal to wake up or bringing their blood flow back, I do not believe either is sufficient to explain the changes we’ve observed.
•One of the key energy sources for cells is the layer of liquid crystalline water that forms on their surface (and their organelles), as its formation, which requires removing positive charges from water, results in those positive charges (hydrogen ions) lying adjacent to negatively charged cells and hence creating an electrical gradient. Gerald Pollack was recently able to demonstrate that exposure to UV light increases the negative electrical charge of that layer. I found this particularly interesting as decades ago, the pioneers of UVBI suspected that UVBI created an electrical shift in cells which made it harder for the HIV virus to enter them.
Note: liquid crystalline water also harnesses light to create the spontaneous flow of fluid within the body.
•Years ago, Russian scientists demonstrated that cavitation bubbles are formed within the blood (discussed further here), which both provide an energy source for blood to move through the body and a way for the blood volume to expand as needed. One of the mysteries of UVBI is the observation that it causes an expansion of the blood volume and a decrease of the hematocrit, something to the best of my knowledge could only be explained through the cavitation bubble model. In turn, like the previous point, this may explain how UVBI is able to impart energy to the body which immediately imparts momentum to its fluids.
•One school of medicine believes invisible cell-wall deficient bacteria (e.g., mycoplasma) underlie many chronic autoimmune conditions (detailed in this textbook and summarized in this article), as once one knows how to look for them, they are frequently found within tissue suffering an immune response from the body (and likewise, many natural health practitioners have observed interventions which create these organisms such as cell wall destroying antibiotics frequently lead to autoimmune conditions in the future). In turn, UVBI happens to be one of the most effective tools for eliminating these organisms. Consider for example this case report:
A cohort of 5 family members who had a variety of chronic diseases (e.g., Crohn's disease, asthma, complex regional pain syndrome, hypothyroidism, type 1 diabetes mellitus, and lymphangiomatosis) found 4 had a MAP (mycobacterium paratuberculosis) infection. Two patients received antibiotics and UVBI, and then experienced a resolution of their autoimmune symptoms.
Note: evidence also suggests DMSO’s potency against cell wall deficient bacteria underlies some of its therapeutical value in both cancer and autoimmune conditions.
•White blood cells absorb UV light, but overactive ones absorb too much (with it then being cytotoxic to them).
•UVBI generates ozone, and some of UVBI’s therapeutic properties are due to ozone (an observation strengthened by the fact there is a significant overlap in the benefits of UVBI and ozone therapy).
•UV light emitted by cells through secondary radiation (cell such as those in the blood emit light after having previously absorbed it) has an inhibitory effect on microbes. Exactly why this happens is a matter of debate (e.g., it could be due to the cells becoming more difficult for microbes to enter, or it could be due to those faint emissions damaging the microbes).
Note: one of the most intriguing explanations I’ve come across arose from an observation made a century ago by early researchers into the effects of weak biological UV emissions on cell growth, where typically these emissions triggered it, but in certain cases instead inhibited it (e.g., women on their menstrual cycles have been observed to inhibit the growth of micro-organisms such as those in fermented food products and this effect was traced to their blood—something I suspect served as a mechanism to prevent them from becoming infected by bacteria or yeasts during menstruation).
I must emphasize however that these mechanisms are by no means a complete explanation of what is going on.
Our Experiences With UVBI
My first exposure to UVBI was for years of migraine-like headaches I’d had (for which UVBI greatly benefitted me). After that, I learned of Thomas Ott’s work, and my interest became primarily focused towards what it told us about the vast potential of human physiology rather than any clinical applications for it. In turn, it was not until I had the background that a medical education provides that I was able to appreciate just how monumental many of UVBI’s clinical effects were.
Unfortunately, due to the politics of American medicine, UVBI is virtually impossible to get inside a hospital, and for this reason, I’ve had to watch more cases than I can count of a patient who desperately needed UVBI not given access to it regardless of what I tried to do.
For this reason, my experience with UVBI for acute illnesses is typically regulated to colds and the flu (which it would often instantly eliminate) and the odd chance where I could catch someone with a severe illness before they went to the hospital (and it was safe to postpone their hospitalization by a few hours), which in many cases allowed them to avoid hospitalizations. I have however talked to colleagues who were more daring than me and were able to replicate some of the results seen throughout the UVBI literature for severe illnesses.
This changed during COVID, and I (like many other UVBI doctors) had numerous severely ill patients who did not want to go to the hospital that I gave UVBI to who then had rapid (or slow) recoveries and avoided hospitalization. Additionally, we found that like many other treatments for COVID, UVBI became less effective the later in the disease process it was used (e.g., it typically took more UVBIs to get the same improvement as someone became sicker) and that as people became more ill, people with more sensitive systems had a better response to IV vitamin C or exosome therapy than UVBI (although UVBI nonetheless worked—for example see the Russian study I cited above).
Note: one of the things that consistently amazes me about UVBI is how fast the response to it is, as you can often have patients who seem to have poor vitality or be shutting down, immediately come back as they are receiving a UVBI.
Because of all of this, in America, the usage of UVBI is typically constrained to the integrative medicine field (although as mentioned above, a few physicians in other specialties like obstetrics and gynecology are willing to use UVBI on an outpatient basis for their patients). Many of those doctors have used it on thousands of patients, and they all report it benefits the majority of their patients (figures around 80% are often cited for patients with challenging chronic conditions—although in more difficult cases this often requires numerous treatments). That said, we’ve found the efficacy varies depending on which UVBI unit is used, and that the physicians with a lower success rate tend to be using more marginal machines. Likewise, the clinical efficacy of UVBI can be improved by appropriately dosing it, but even without doing that, it still yields significant benefits.
Within integrative medicine, the most common use for UVBI is to treat chronic viral infections (e.g., Epstein Barr, shingles, herpes), as it appears to be one of the most effective treatments for them (and many patients can attest to this), along with Lyme disease (a bacterial infection which is nonetheless difficult to treat). In turn, I’ve met Lyme patients who’d already tried many other therapies but found UVBI transformed their life and I’ve also met other Lyme patients who felt it gave them a tangible improvement but they didn’t report anything as dramatic as the stronger responders.
Note: I have also seen it used to help treat bacterial infections which are not responding to conventional antibiotic therapy (which it definitely helps), however, this is not the default application for it.
The second most common use is for autoimmune conditions, and I’ve frequently seen UVBI be used as an “if in doubt, try UVBI and see what happens” therapy (where it normally helps). For example, it often yields significant improvements for chronic fatigue syndrome. Likewise, it often helps with a variety of allergic conditions. In turn, I believe many of the benefits individuals attribute to UVBI eliminating a chronic infection are actually due to the other therapeutic benefits UVBI provides besides the direct elimination of infection.
Note: UVBI is one of the only IV therapies I know of that will consistently give a positive effect a patient will notice and be relatively unlikely to have side effects.
More recently, we’ve seen it often significantly help individuals with COVID-19 vaccine injuries, although typically it requires repeated sessions, and achieves a partial rather than complete recovery (whereas for long COVID, the response is much stronger and a few sessions often suffice). From having explored this question at length, I also suspect UVBI is able to “detoxify” the spike in a similar manner to what it was observed to do with a variety of biological toxins.
The circulatory benefits, improvements of the cell danger response, and the ability to reactivate some part of the body which has become dormant or isn’t quite functioning correctly are also very real benefits of UVBI, however I find that this application is used much less frequently than the others in America.
Lastly, we believe that UVBI to some extent has anti-aging effects, so we have many older patients who routinely do it to extend the functionality of their bodies and prevent many of the symptoms of aging from developing.
Additionally, a variety of benefits have also been observed with using UVBI for animals (e.g., I know a few holistic veterinarians who have successful practices based around doing this). Likewise, Russian veterinarians have reported excellent results with UVBI for a variety of more severe conditions (e.g., diseases that often wiped herds out).49
Above all, I must underscore that UVBI truly makes a difference in people's lives. It is for this very reason that I prioritized and dedicated time over the past month, often at the expense of other commitments, to compose this article.
UVBI Protocols and Resources
In the final section of this article, I will discuss:
•How we use UVBI (e.g., dosing, which frequencies of light, when to combine it with ozone).
•UVBI’s utility in cancer (e.g., reducing the side effects of conventional treatment regimens).
•Which UVBI machines we have found to provide the greatest clinical benefits.
•How to locate providers offering UVBI with those devices to patients (or pet owners).
•Resources for physicians interested in learning more about this modality.
