The Forgotten Science of Vaccine Disease Provocation
Why do vaccines cause people to get the diseases they are supposed to protect you against?

Story at a Glance:
•Many people notice they appear to become ill with the disease they are being vaccinated against (e.g., the flu or COVID) after receiving a vaccine.
•While this association is frequently ridiculed by medical profession, over a century of evidence exists that demonstrates it occurred for a variety of diseases (e.g., there is extensive literature on it for typhoid fever, tuberculosis, and polio), to the point it was previously termed “disease provocation.”
•Unfortunately, since the knowledge of disease provocation would decrease vaccine sales, it tends to “vanish” from the medical profession’s memory, leading to almost identical debacles happening a few decades later that doctors at the time were “baffled by” (e.g., we discuss how this happened with polio).
•Disease provocation appears to be due to the immune system being diverted to targeting the vaccine’s antigen rather than doing it’s natural job. Since we frequently depend upon the immune system to control latent infections or recent ones currently in the incubation stage, that immunological diversion can lead to an existing infection spiraling out of control.
•In this article we review many examples of how this happened with infections in the past and highlight how this same process can cause vaccination to increase one’s risk of a severe flu infection, a severe COVID infection, a Lyme disease reactivation or a HPV infection progressing to cervical cancer.
Throughout my life, I have noticed more people than I can count (including groups of people) come down with the flu after they receive the flu vaccine. Whenever this is brought up in medical circles, the response typically is “correlation is not causation” and being lectured on the fact the injected influenza vaccine does not contain any live viruses so it can’t give you the flu.
More recently, I (and quite a few of my colleagues) noticed that this also happened with the COVID vaccine and more concerningly, we would come across cases where the person we knew not only got COVID but in some cases became severely ill, had to be hospitalized and then died. While this was understandably “denied,” I soon came across research from the adverse event reporting databases which showed that the two most common causes of death seen in association with the COVID-19 vaccines were heart issues (e.g., dying suddenly) and COVID-19, with the heart issues typically being clustering near the time of vaccination, while after a few weeks, the most commonly reported cause of death following a COVID-19 vaccine was…COVID-19.
Note: this is also shown in national trends of COVID-19 cases and deaths, as they tended to spike after vaccination campaigns were conducted.

Since I saw this so frequently, it left me wondering exactly what was happening.
Note: one of the most convincing cases I saw came from a response submitted to a survey (Steve Kirsch had me analyze) where a man reported having a PCR confirmed (a-symptomatic) COVID-19 infection which immediately progressed to a severe infection after vaccination.
Initially, I suspected this was due to a hyper-inflammatory process. This was because many of the complications of COVID-19 are due to the immune system’s response to the virus rather than the virus itself (e.g., in hospitalized patients, as the disease progresses, the viral load often drops, but despite the virus being eliminated, the patients become more ill and the illness becomes more fibrotic in nature).
Note: one of the most interesting models I came across to treat COVID-19 came from Shankara Chetty, a South African doctor who concluded the body was forming an allergic response to the spike protein, which in turn necessitated either eliminating the virus early on (so this would not happen) or treating it as an allergy once the second phase began. Given that this worked for 7,000 people and his model matched what many of us observed, I found this theory quite compelling.
Since vaccines excessively stimulate the immune system, I theorized that the inflammatory response the vaccines create are tipping an already stressed system over the edge into a dangerous hyperinflammatory state.
Note: this is a common component of the Cell Danger Response, a chronic dysfunctional mitochondrial process which underlies many chronic conditions.
This hypothesis in turn was reinforced by an inconvenient discovery with the HPV vaccine. For reference, the HPV vaccine was pushed upon the world under the theory that a chronic HPV infection could transform cervical tissue into cancerous tissue, and that since HPV was thus the cause of cervical cancer, preventing women from getting HPV through a vaccine could hence prevent women from getting cervical cancer.
Unfortunately, there were a lot of holes in that chain of logic. One of these was the discovery that if someone was vaccinated for a strain of HPV they already had, it significantly increased their risk of getting cervical cancer.

Note: an identical effect was also found with GlaxoSmithKline’s competing HPV vaccine Cervarix. In a previous article on the subject of disease provocation, I took a deeper dive on the HPV vaccine data.
However, requiring women to be tested for HPV prior to getting the vaccine would have significantly reduced vaccine sales (e.g., those who had already been infected wouldn’t vaccinate and many patients wouldn’t return for a follow-up visit once their negative test results had come in). This I believe explains why a decision was made to ignore this glaring problem and instead simply recommend beginning HPV vaccination at a much younger age (at 9-12) under the hope this would precede their first sexual exposure to the virus—which was unfortunately because the HPV vaccine had a very high rate of severe side effects, and it was not dosed at a lower amount for younger (and hence smaller) children.
Note: similarly, while individuals acutely ill with COVID were encouraged to wait a few days before vaccinating, the current guidelines do not advocate for having PCR test for COVID prior to vaccination (despite the fact so many were given that many Americans were receiving them on a weekly basis).
Like the COVID-19 example, I assumed “negative vaccine efficacy” had to be due to a hyperinflammatory response from vaccination (as the reason HPV created cervical cancer was due to the chronic inflammation it created in the cervical tissue).
Recently, as I began reviewing a remarkable collection of literature on the forgotten dangers of vaccination, I discovered that what I had observed with these vaccines was actually a longstanding problem that had been seen in the past with many other vaccinations, but sadly, again and again, that lesson was forgotten. Because of this data, I now believe this primary issue is not excessive inflammation but rather vaccine-induced immune suppression.
Note: a variety of mechanisms have been proposed to explain the significant immune suppression observed following COVID-19 vaccination (e.g., the COVID vaccine being shown to destroy of the hematopoietic stem cells which create a pivotal part of the immune system or antibody dependent enhancement—something known to observe with various vaccines including influenza and SARS). In this article I will primarily focus on one mechanism.
Original Antigenic Sin
Original Antigenic Sin (OAS) refers to the observation that if someone is vaccinated for a different strain than what is currently circulating (e.g., of the flu) they tend to have a worse immune response than those who were never vaccinated. Furthermore, multiple studies have shown that OAS affects completely different species (e.g., if you receive an influenza vaccine, you are less able to mount a response to “flus” caused by other respiratory viruses) and that OAS can persist for at least a year after vaccination.
Note: in a previous article, I discussed a 2009 article, a 2009 study, a 2010 review, a 2010 study, and a 2013 study (published in peer-reviewed journals such as the Lancet), which collectively found a 40-166% increase in the likelihood of getting infected with a virus which differed from the strain you were vaccinated against (e.g., a pandemic influenza strain which had a greater risk of hospitalization) and up to a 100 fold increase in one’s viral load (which increases transmission). Additionally, in children who received a non-matching influenza vaccine, a 2012 study found they were 267% more likely to be hospitalized for influenza and another 2012 study found that 29.0% developed an infection with a non-influenza upper respiratory virus (compared to 3.4% of the unvaccinated). Finally, a 2023 study inadvertently showed influenza vaccination significantly increased one’s risk of being hospitalized for the flu.
OAS is thought to be a result of off-target immunity leading to partial immune suppression. Specifically, since the immune system has a finite ability to respond to threats, if it becomes hyper-primed to target one antigen (e.g., the vaccine antigen it is continually provoked to target), its focus is diverted away from other antigens it needs to respond to. This in turn makes sense since the immune system (which does not have an infinite number of immune cells) has to prioritize targeting life threatening infections, but unfortunately, since it did not evolve in tandem with the era of vaccination, it is not always prepared to appropriately to respond to the artificial immune stimulation vaccinations create.
Note: typically speaking, vaccine antigens persist in the body for a prolonged period (as the immune system cannot break down the immunostimulatory aluminum adjuvant they contain). This issue became a much greater problem with the COVID vaccines because the body has difficulty breaking down the synthetic mRNA they contain, which in many cases has led to the (immunostimulating) vaccine spike protein still being produced more than a year after vaccination.
In the case of influenza vaccinations, since the vaccines require months to produce and hence need to be made before the seasonal circulating strain is known, the wrong strain is frequently chosen. This leads to the annual vaccine often being ineffective, and worse still, frequently leading to OAS and exacerbating the existing flu season.
Note: in most “bad” influenza years, I typically hear colleagues argue that it’s a bad season because the wrong vaccine was chosen, but it’s still essential to vaccinate because had lots of people not vaccinated, that year’s flu would have been even worse (an effective marketing slogan which was repurposed throughout COVID). However, my own experience has been that whenever I saw someone in the ICU for an influenza infection during one of those “bad” seasons, their chart always showed they were vaccinated—an observation directly supported by some of the studies I linked to above.
Disease enhancement from a mismatching vaccine is a rarely discussed but well-known problem. For example, a reader and physician who worked in the NIH was assigned to study this issue from 2009-2011 and followed a cohort of vaccinated children and pregnant months over 3 flu seasons also discovered a clear trend of negative vaccine efficacy. When she submitted her analysis, however, she was removed from the NIH and blacklisted from future employment (and as a result, she understandably harbors great disdain for Anthony Fauci).
The solution Fauci and the NIH in turn pushed for was to utilize mRNA technology to produce seasonal influenza vaccines since the production time for them was much shorter (so they could begin being produced once the circulating flu strains were essentially known). Unfortunately, since SARS-CoV-2 mutated much faster than a typical influenza virus, even with this shortened production time, it was still not quick enough to match the circulating variants (even when now boosters were rolled out multiple times each year).
In turn, because of the focus over the last few years on studying everything related to COVID, a study of 51011 people at the Cleveland Clinic gave the most overt proof of OAS I have seen in the scientific literature as more vaccinations were directly correlated to one’s susceptibility to repeating COVID infections:
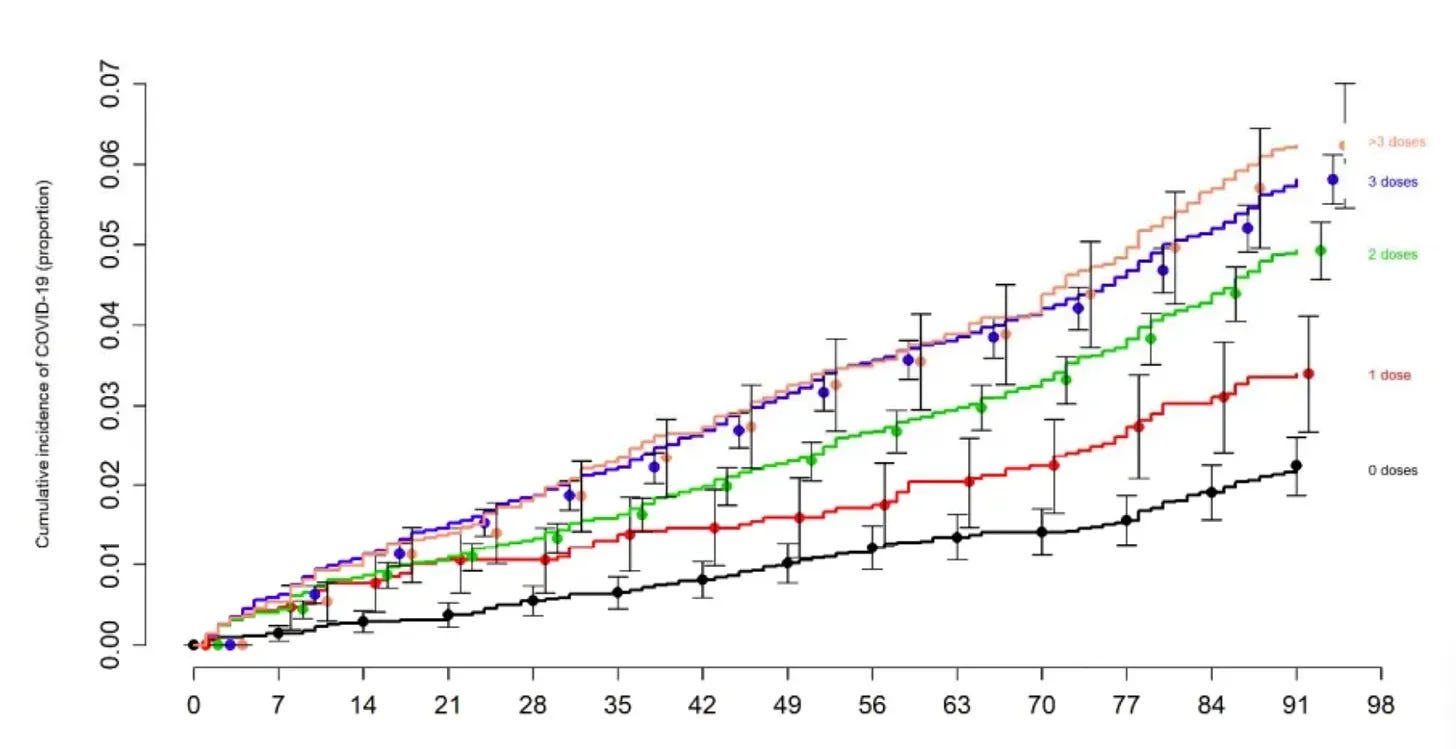
Note: there are many cases you can read online of individuals who have received multiple COVID boosters continually getting COVID (e.g., Igor Chudov periodically compiles them).
One of the most tragic examples of OAS was Peter Aaby’s WHO studies which found childhood DTwP vaccination in Guinea-Bissau (a vaccine which is no longer used in the United States due to its toxicity) caused children to be 5 times more likely to die (3.93 for boys and 9.98 for girls)—something, which in most cases, was due to them succumbing from one of the many lethal infectious diseases circulating in Subsaharan Africa. Sadly, while his data was published, it was largely ignored by the global public health apparatus since it would have required abandoning a practice they were deeply invested in.
Note: While vaccines with a small number of antigens coupled to adjuvants were fairly problematic, Aaby conversely found those with many antigens that did not contain adjuvants (the live attenuated vaccines like BCG or MMR) generally increased immune function, and hence saved lives in areas where people frequently died from infectious disease.
Off-Target Immunity
As OAS shows, it is not always a good thing to hyper-prime the immune system to respond to a single antigen. Unfortunately, there is very little recognition of this within the medical profession. For example, consider Paul Offit’s frequently cited claim that there is no need to space vaccines out because the human immune system has the ability to respond to at least 10,000 antigens simultaneously. While his “calculation” is correct, as shown by the previous examples, it ignores the fact that there is a lot more to a functional immune response than a circulating antibody contacting a target immune antigen and beginning the antibody production (cloning) process.
Similarly, since most vaccines work by excessively provoking the immune system to respond to small amounts of an injected antigen, this frequently leads to the immune system being provoked into responding to things it should not. This, in turn, helps to explain why vaccines are so strongly associated with a variety of autoimmune disorders and allergies (e.g., to the pollens that were circulating at the time of vaccination).
Note: adjuvants (e.g., aluminum) are much cheaper to produce than vaccine antigen proteins, so the industry typically defaults to producing vaccines with small amounts of antigens supplemented with an adjuvant. I believe this is done because it makes the vaccines much more affordable to produce.
Unfortunately, like OAS, off-target immunity leading to autoimmunity is largely ignored (despite a textbook existing on this subject) and most doctors aren’t even aware it’s an issue because they assume vaccines just magically only create the desired immune response and nothing else. Because of this, we are stuck in the unfortunate situation where there has been an explosion of chronic illnesses around the globe, and no explanation existing to account for how this could have possibly happened.
Off-Target Immune Suppression
Because of the previous (e.g., OAS), I entertained a second hypothesis to explain what I was observing with the COVID vaccines—if someone had a latent infection or a developing infection the immune system was keeping in check and the immune system was then diverted to hyper focusing on a specific vaccine antigen, it would lose its ability to keep that infection in check.
This was best demonstrated by the strong association between shingles and COVID vaccination, a condition which occurs when a latent infection (herpes zoster) reactivates due to a weakened immune system (e.g., Steve Kirsch compiled some of the data supporting this link). Furthermore, a variety of types of (increasingly severe) forms of shingles can occur, with the most severe types typically being exceedingly rare. For example, Justin Bieber had roughly a 27/1,000,000 chance of developing the form of shingles induced facial paralysis he developed two years ago, while the even rarer brain infection Senator Dianna Feinstein died from last year is estimated to occur in one out of every 33,000–50,000 shingles cases and is associated with immunologically suppressed patients.
The most detailed study I found evaluating the reporting of these events after COVID vaccination found the following:
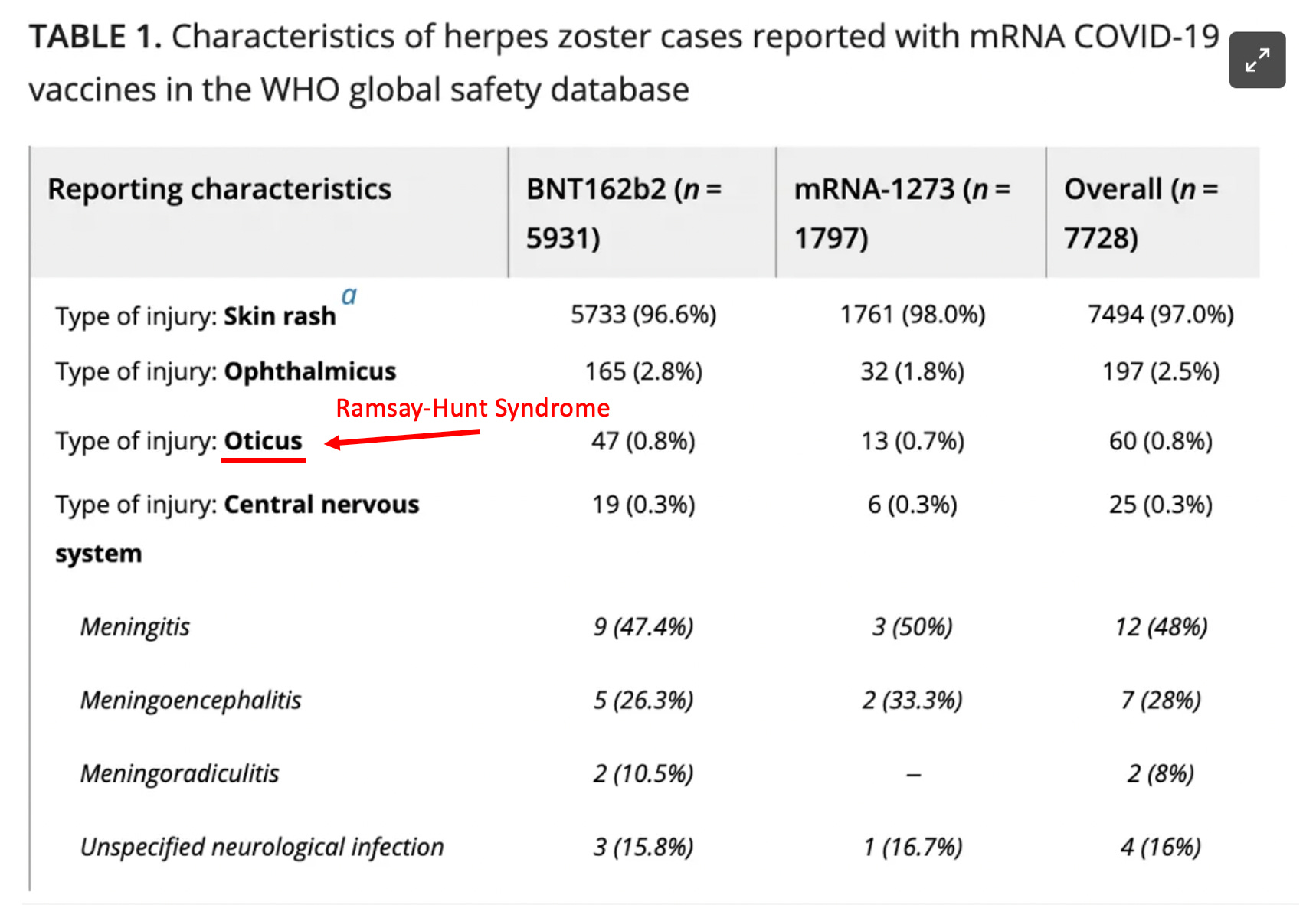
Note: keep in mind that less than 1% of the total adverse reactions that occur from vaccination are ever reported.
Likewise, as documents released by court order showed, many forms of shingles were reported by Pfizer to the FDA:
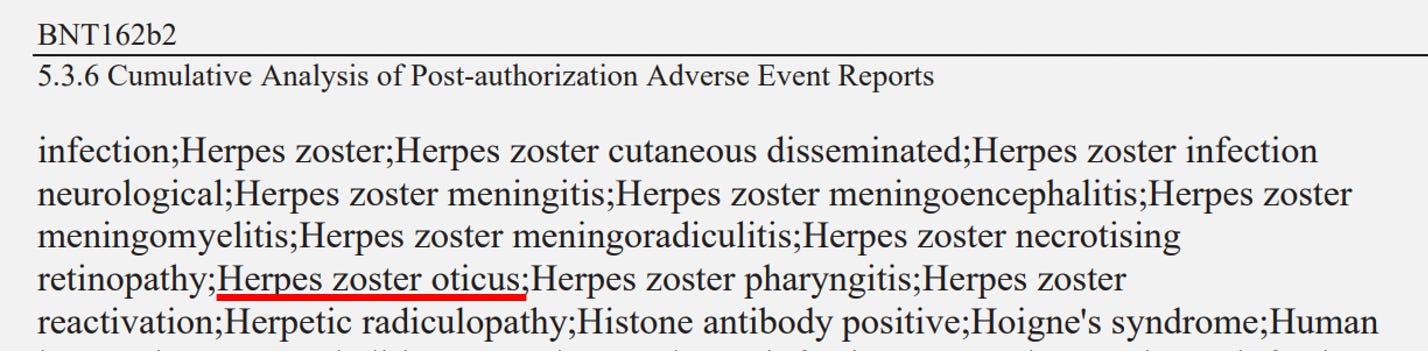
Note: just a year after the COVID vaccines hit the market, Pfizer and Moderna publicly announced they were developing mRNA vaccines for Shingles. Many suspected this was motivated by shingles being a common side effect in their 2020 trials. Similarly, the COVID manufacturers have pushed forward RSV vaccines, another condition which spiked after the COVID vaccines came out.
Another problematic latent infection is Lyme disease, an infection that is quite difficult to treat clinically. This is because it can hide in the body for long periods of time until it is activated during a period of immune suppression (e.g., prolonged stress) and simultaneously the condition has a wide range of symptoms that are often hard to attribute to Lyme disease. In turn, I have come across numerous cases of individuals with chronic Lyme disease who became much worse following COVID vaccination. Likewise, according to MyLymeData (a website that compiles data collected from Lyme patients) 25-28% of them (depending on the vaccine) experienced a Lyme flare after COVID vaccination, although it is difficult to say if this was a progression of their existing infection or simply an exacerbation of pre-existing inflammation.
However, what’s less known is that in 1998, a Lyme disease vaccine was brought to the market which was initially thought to be “safe and effective” and was widely promoted on prime-time television. However, within a year, numerous adverse reports began to surface (which the media was willing to cover) and a class action lawsuit was filed on behalf of injured victims (which I believe was possible to file since the vaccine was not on the CDC schedule) alleging that the manufacturer concealed the vaccines risks from the public. Before long, a media storm gathered, so the FDA in 2001 was forced to address the concerns about the vaccine, but despite uncovering significantly more evidence of harm and hearing many testimonies against the vaccine, decided its benefits outweighed the risks. Ultimately, it was withdrawn from the market in the following year due to additional adverse event data emerging and declining sales all of that bad press had generated.
Significant debate arose over why these side effects were occurring, and eventually it was concluded that the susceptible ones were those with a genotype (HLA-DR4+) that was also known for being susceptible to Lyme disease. Since many of the symptoms mirrored those experienced during a Lyme disease flare, this led to those with the extreme reactions being tested for Lyme disease, with that subset of vaccine recipients typically testing positive for Lyme disease.
Unfortunately, the existing testing could not distinguish between the Lyme vaccine triggering a cross-reactivity (which created a false positive) and the presence of an actual active infection. As a result, it remains a subject of debate if those who received the vaccine suffered complications from a pre-existing Lyme infection or the inflammatory response to it, but my colleagues who were treating Lyme patients at the time believed those who reacted to it were those with pre-existing Lyme infections.
Note: More precise testing now exists that could distinguish between Lyme antibody cross-reactivity and a Lyme infection, but it was not available at that time.
Lastly, in addition to these examples, I have also seen other examples of the immune system “failing” once its function is diverted to something else. For example, in addition to eliminating infections, the immune system is also response for repairing damaged tissues, removing cellular debris, and keeping cancers in check. In turn, I’ve seen multiple cases where a patient with an essentially stable cancer had an invasive abdominal surgery (utilizing electrocautery) have their cancer spiral out of control after the operation because repairing the surgery diverted the immune system away from addressing the cancer.
Note: numerous scientific papers recognize that the immune system becomes suppressed when someone is recovering from surgery.
Sir Graham Wilson
In 1967, Sir Graham Wilson, an eminent bacteriologist from the London School of Hygiene & Tropical Medicine (with the help of many anonymous colleagues) decided to publish an exposé of the vaccine industry which showed that, contrary to the widely held belief vaccines were always “safe and effective,” over the last century, many people had experienced severe vaccine injuries and countless vaccine disasters had been covered up (especially within the military).
Wilson supported the practice of vaccination, but felt his profession needed to honestly discuss the risks and benefits of vaccines (as opposed to them all being “safe and effective”) so that past vaccine disasters would stop being repeated. Unfortunately, his pleas fell on deaf ears, and many of the things he described in his book continues to be repeated to the present day.
Note: as Wilson shows (and many others have well as well), there has been a longstanding mentality within the vaccination field to insist all vaccines are always “safe and effective” and that adverse events are “incredibly rare” as for more than a century, they have adamantly believed acknowledging the real issues with vaccination with “give ammunition to the anti-vaxxers.” Likewise, in 1955, Paul Meier, an epidemiology professor from Johns Hopkins, in commenting the government’s polio vaccine fiasco (arising from the release of contaminated lots), gave a scathing criticized the government’s choice to repeat the “safe and effective” mantra despite knowing it was patently false.
Wilson in turn cited private government and vaccine company documents (e.g., from England’s Ministry of Health [MoH]) that were made available to him due to his prestige within the field alongside published literature on the dangers of vaccination. I, in turn, tried to locate the sources he referenced and was able to find about half of them (which are linked to and in each case matched what he attributed to them), was able to find citations referencing about a quarter of them (denoted with a †) , and could not locate a few of them (denoted with a ‡).
Note: many of these links go to the CABI Digital Library. If you wish to view those articles without signing up, search for that article within Google Scholar (by copying the URL in) and then access it through the Google Scholar link.
Because I think this book (which can be read here) is such an important historical record, I’ve gradually been working on condensing it into an article. However, since the initial draft was 20,000 words, I realized it needed to be split into multiple articles (e.g., my next piece about it will focus on the enduring issue of vaccine “hot-lots”).
Through Wilson, I learned that the activation or worsening of an existing infection (which was termed “disease provocation”) is actually a longstanding problem and that certain vaccines were notorious for doing this with a variety of different infections.
Disease Provocation
As far as I know, the earliest experimental demonstration of the disease provocation phenomena was an 1893 study† described by this 1925 paper as follows:
In 1893 Brieger and Ehrlich showed the sequence of events on injecting a previously immunized animal with a bacterial protein. In experiments upon goats injected with tetanus toxin they notice marked drops in antitoxic titres following successive injections and plotted curves showing these depressions. In later studies of A. E. Wright upon the opsonin content in human blood these changes in potency were referred to as phases, an increase being called a positive phase while a decrease was designated as a negative phase. It is largely through the careful work of Wright that the attention of immunologists has been called to these fluctuations in antibody in the course of artificial immunization.
Since the time of these pioneer studies, it has become common knowledge that more or less of a "negative phase" may be noted on injecting a previously immunized animal, and almost everyone engaged in measuring the potency of serums from experimental animals, and human serums in opsonin titrations has encountered this sudden drop in titre after injection, later to be probably followed by an increase in antibody or a "positive phase". Particularly in the case of man this negative phase or depression of immunity has been a cause for apprehension on the part of those carrying on artificial immunization.
Note: a similar observation was made by Ehrlich‡ some years earlier with the ricin (a toxin) antibody count in mice.
Tuberculin Disease Provocation:
Because of his earlier discoveries, Robert Koch (the creator of Koch’s postulates) was a highly regarded scientific figure and viewed as a national asset by the German government. After focusing his efforts on the scourge of tuberculosis, he discovered that a (protein) extract from killed tuberculosis bacteria would provoke a strong immunological reaction where it was injected under the skin if someone had been infected with tuberculosis (which we still use today in the PPD test for tuberculosis). This inflammatory response led him to suspect that his therapy could also trigger a therapeutic response that would eliminate a latent or active tuberculosis infection.
In 1890, to great fanfare, he announced this cure to the world, and because of his reputation, it was quickly taken up by physicians around the world (e.g., patients flocked from all over Europe to attend the press conference where he announced it and doctors quickly began charging exorbitant prices for it). Before long, it was subjected to a large study, where it was found patients who received it were more likely to die than recover and that there were many cases of their infection rapidly progressing.
Owing to the high fatality rate of the therapy, it largely was abandoned within a few years and Koch’s reputation was destroyed. Given that Koch was unsure of the therapy at the time he announced it (as it was still in the experimental stage in his lab) significant debate exists as to why he did this (e.g., he was having a midlife crisis, the German government pressured him to announce it so they could profit off selling it, or because he had personally positioned himself to become rich from it). After the initial debacle, Koch and many other doctors did not give up on this approach, but despite many efforts to refine the product, it never worked therapeutically and was eventually completely abandoned around World War 2 once the initial antibiotics for tuberculosis were invented. Remarkably though, as late as the 1950s, medical textbooks still discussed it as a potential cure for tuberculosis.
When I learned of this, I could not help but notice how similar it was to the promotion of COVID vaccines as a treatment for long COVID. As best as I can tell, this was spearheaded by our government (without evidence) promoting it as a way to prevent long COVID:
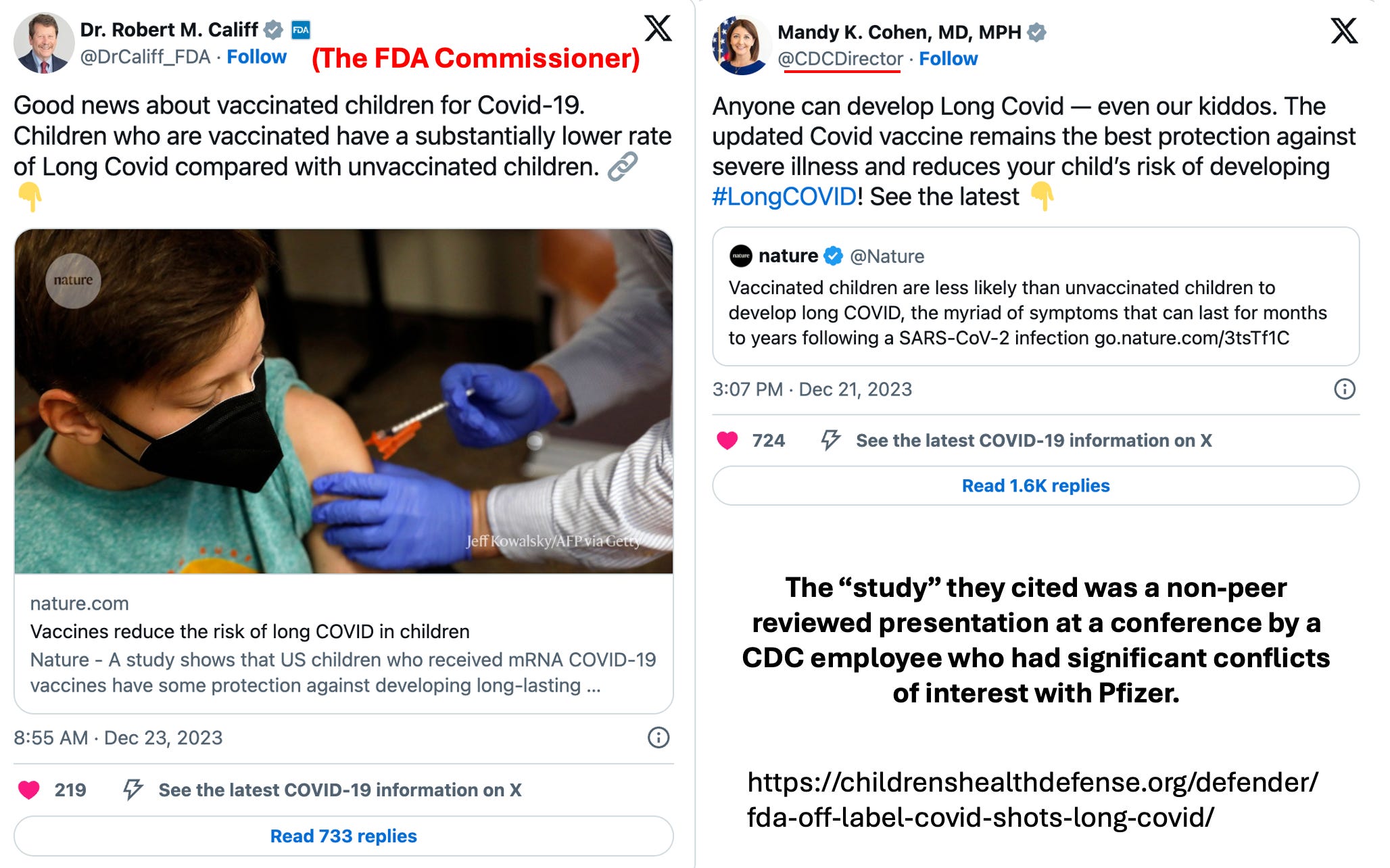
In turn, (despite the fact COVID vaccination frequently created a chronic condition similar to long COVID), the vaccine (without evidence) was widely promoted as a way to treat long COVID. Unfortunately, every person I know with long COVID who did this became much worse after they received their “therapeutic” vaccination—and as far as I can gather, my observation was not at all unique. As a result, like the tuberculin therapy of the past, using the vaccine to treat long COVID has now been largely discarded and forgotten.
BCG Disease Provocation
Note: BCG is the (typically live) tuberculosis vaccine.
•A 1951 paper documented the effect of vaccinating 31 patients suffering from pulmonary tuberculosis with BCG. All 31 had an accelerated local reaction starting 24—36 hours later, reaching its maximum in 5-8 days, crusting over in a fortnight, and healing with detachment of the crusts in a month. Of them 80% had regional glandular reactions, 19% (6) had fairly severe focal reactions, and 32% had general febrile reactions. The six focal reactions were characterized either by hemoptysis (coughing up blood), laryngitis (issues in the throat), a radiological extension of the lung lesion (growth of a tuberculosis pocket), or an aggravation of their tuberculosis infection, while the general reactions included significant fevers, serous polyarthritis (a more severe form of arthritis), hemoptysis, pleurisy (painful inflammation of the lungs), enlargement of existing lung tuberculosis cavities, and an otherwise unexplained maculopapular rashes on the trunk.
Its authors concluded that there is serious danger in giving BCG to patients with pleuro-pulmonary lesions, and that mass vaccination without previous tuberculin testing is inadvisable.
•Another 1951 paper evaluated 30,000 children in Yugoslavia who had received a BCG vaccine, with 100 who appeared to have a tuberculosis disease provocation despite having a negative PPD. They experienced a severe, suppurating, ulcerative reaction at the injection site, a fever lasting for 2-3 days, a rise in their ESR and white blood cell count, and some loss of appetite and weight. In at least three of the children this was followed by a reactivation of their tuberculosis lesions.
Typhoid Disease Provocation:
Note: I believe the strongest evidence for vaccine disease provocation can be found with the typhoid fever vaccine.
•A 1901 paper found that when humans receive the typhoid vaccine, the ability of the blood to neutralize bacteria often first decreases for a time before rising.
Note: I believe this is analogous to the negative phase (of declining antibodies) that follows immunization, which was discussed above.
•A 1915 paper† discussed a typhoid outbreak that struck the German Army in France in 1914 and was responded to by vaccinating them three times against typhus with each injection being 8 days apart. There, it was observed the first and second vaccines could trigger severe typhus cases, but this did not occur after the third vaccination.
•Another 1915 article† about those events stated that 28 out of the 707 men who received 3 injections developed typhoid fever shortly after injection. Conversely, the author also looked at 202 patients who had developed typhoid fever and discovered that 34 of them had become ill within three days of vaccination (but had no signs of typhus at the time of their vaccination).
•Another 1916 article† stated that since the typhoid vaccine provoked latent infections, the German army used it to detect who was carrying a latent infection (which was implemented by revaccinating everyone once an outbreak occurred).
•A 1920 article discussed a 1918 typhoid outbreak in a small (occupied) German Town which British authorities responded to by vaccinating 14,343 of the 21,248 civilians for typhoid (with two doses given 10 days apart). Prior to the vaccination campaign, the outbreak was declining, but after vaccination, a fresh crop of cases appeared and 16 persons came down with Typhoid immediately after the first dose, 7 became ill between the two doses, and 6 immediately after the second dose, and 2 two days after the second dose.
•A 1927 article† about a 1926 outbreak said that many of the cases came on directly after typhoid vaccination. A 1928 article stated that 2,200 typhoid cases occurred and that 117,000 persons were vaccinated. That article’s author was in charge of 800 of the typhoid patients and was of the opinion that 38 of them were cases of provocation disease (33 typhoid and 5 paratyphoid fever). Of the 33 typhoid cases, 13 came on after the first, 17 after the second, and 3 after the third injection; 14 of the 33 cases had their onset on the following day. In some the disease started abruptly with a rigor (fever and chills); in others the reaction to the vaccine passed insensibly onto the disease
•Another 1927 paper† provided evidence that vaccination during the course of a typhoid outbreak was liable “to activate latent infections and render them manifest” and cited an instance where the vaccinated fared worse than the unvaccinated during a typhoid outbreak.
•A 1932 paper that studied the reactions of 2,500 patients who received the typhoid vaccine to treat an underlying condition (e.g., arthritis or a vascular disease) commented on the provocative nature of the Typhus vaccine and discussed 14 unusual reactions (e.g., appendicitis, cholecystitis, enteritis, pleurisy, pericarditis, iritis, glaucoma, adenitis, thrombosis, or renal insufficiency) which it attributed to the vaccine unmasking an underlying disease.
•A 1938 article affirmed the existence of typhoid disease provocation and to explain this phenomenon suggested that the existing data indicated there was a period of immunological impairment following vaccination.
•A 1950 study found that that in a large typhoid epidemic (from 1945-1947) on the whole, vaccination lowered the death rate from 19.0% to 11.2%, but in one city (Greifswald) where people were vaccinated in the middle of an outbreak, numerous very severe and often fatal cases followed injection in a few hours to a few days and that individuals who developed typhoid fever within 48 hours of vaccination had a high (19%) death rate. Furthermore, of the 1702 people who became ill during this period, 35.2% followed the first injection, 27.8% the second, and 14.7% the third. From this data, the author concluded that vaccinating while infected shortened the incubation period of a typhus infection and increased one’s likelihood of dying.
•In a followup to the 1950 paper, the author (Raetteig) in 1959 infected mice with typhus and then vaccinated them with a (killed) typhoid vaccine during the incubation period of their typhus infection, which in turn caused a number of the mice to die prematurely.
•In a second 1959 paper, Raetteig then found if he instead gave them a different vaccine during the incubation period (e.g., one for S. enteritidis or Escherichia coli), the mice were again more likely to die, but not the same degree as the typhus vaccine.
Note: as this and other studies showed, certain vaccines had a stronger provocative effect.
•In his third 1959 paper he was able to demonstrate dangerous disease provocation also occurred in mice with a latent infection and that when he recreated the situation of an outbreak (infecting a mouse with typhus and then putting it in a cage with other mice), if he then vaccinated some of the other mice, those mice died faster and in greater numbers than the unvaccinated exposed mice. Finally, he showed that if the mice were vaccinated prior to a typhus exposure, the provocation effect either did not occur or was much weaker. In Raettig’s words:
It is suggested that some recorded human epidemics have shown curves of the type described for a " provoked " epidemic (Provokationsepidemie). Thus the curve of poliomyelitis in Chicago in the first year of vaccination, 1956, contrasts with a curve based on the epidemics of previous years, in much the same way as the author's experimental and control mouse typhoid epidemic curves.
Note: all of Raettig’s 1959 papers (including ones where he showed Polio vaccination also could provoke Polio) can be found here through a Google Scholar search for everything he published in 1959.
•A 1966 paper† discussed five army recruits who came down with an attack of typhoid after receiving a typhoid vaccine.
Miscellaneous Disease Provocations:
•A 1929 survey sent out to American doctors received 5 reports of deaths from tuberculosis after receiving a stock (locally made) mixed vaccine and 7 deaths following “the injudicious use of tuberculin.” In all these cases, like those discussed earlier, the death appeared to result from a latent or mild tuberculosis being activated by the injection.
•The author of a 1933 paper on disease provocation stated that he had observed frequent relapse of malaria and the less frequent relapse of tuberculosis that occurs in patients treated with the antirabies vaccine.
Note: Wilson also cited a case he observed of tuberculosis activating after someone came down with an acute Brucellosis, which I believe was done to illustrate any type of immunological diversion can trigger disease provocation.
•Wilson discussed the activation of tuberculosis by typhoid vaccine given intravenously to a patient suffering from spondylitis reported by Cecil in 1935.‡
•Wilson reported an unpublished record at the MoH of a patient in whom miliary dissemination of BCG (the live vaccine form of tuberculosis) followed smallpox vaccination.‡
•Trench fever is a now forgotten bacterial infection that was transmitted by lice and was a major problem during World War I. A 1949 paper discussed the experience of Polish labworkers who fed the lice (by being repeatedly bitten by them). 30% of those workers were infected with the trench fever bacteria (R. quintana), while others developed an immunity that prevented them from becoming infected after being bitten by an infected louse. However, after they received a typhoid vaccine, the number of them who had R. quintana circulating in their blood increased. Furthermore, the paper’s author cited a case of someone who had had trench fever five years before who had a relapse of it a few days after typhoid vaccination.
•A 1957 paper showed that in mice who had had a multi-month infection of Mycobacterium fortuitum, intraperitoneal injection of killed BCG or pertussis vaccine converted their latent or chronic infection into an acute and sometimes fatal disease. One of the researcher’s most common observations was the appearance of a large microbial population in the liver, whereas in normal mice, M. fortuitum is rapidly cleared from the liver.
Note: I believe this observation is very important because many chronic disease states are associated with blood sludging (stasis) in the liver, something that both vaccination and certain infections (e.g., malaria) frequently trigger throughout the body. Data like this, in turn, begin to illustrate why a significant overlap between blood sludging, immune suppression, and autoimmunity is frequently observed.
Lastly, Wilson noted various authors (e.g., the authors of this 1965 paper) had observed the exacerbation (disease provocation) of an existing tuberculosis infection following the injection of the diphtheria toxoid (the diphtheria vaccine), and that the diphtheria vaccine had also been observed to trigger rheumatism or the onset of an attack of serofibrinous pleuritis (which could have been autoimmune in nature rather than being disease provocations).
Poliomyelitis Disease Provocation:
Attacks of poliomyelitis were frequently observed to follow vaccination campaigns, with the paralysis disproportionately affecting the injected limb. Because of the frequency of polio disease provocation, the medical community appeared to have begrudgingly accepted it was a real thing.
The application of epidemiological surveillance and statistical methods enabled researchers to trace the steady rise in polio incidence along with the expansion of immunisation programmes for diphtheria, pertussis, and tetanus.
— The Lancet (2014)
Documented instances of polio disease provocation included the following:
•A 1937 case report† discussed a 1-year old infant who came down with the symptoms of poliomyelitis (paralysis of all 4 limbs and facial paralysis) a week after injection of the APT vaccine.
•A 1950 paper describing 82 cases between 1941 to 1949 of poliomyelitis 7 to 21 days after diphtheria or pertussis vaccination. This paralysis was observed to affect the left arm (the typical site of vaccination) four times as often as the right.
Note: Wilson also identified 31 cases of this happening reported to England’s MoH between 1941-1946 and suspected many of these overlapped with those 82 cases.
•A 1950 paper noted that in England’s 1949 polio epidemic, 30 out of 182 paralytic patients under five years of age had been immunized against diphtheria, pertussis, or both within four weeks of contracting poliomyelitis. In all of these cases, the limb last injected was paralyzed; in another 7 cases a different limb was affected. In 21 of the 30 cases, a combined diphtheria and pertussis vaccine had been used, APT was used in 8, and pertussis vaccine alone in 1. The author calculated that 1 in 1800 children became paralyzed after immunization.
•A 1950 statistical analysis was conducted of 410 poliomyelitis patients under five years of age from 33 areas of England and Wales during the 1949 epidemic. In 164 of these cases, a closely paired control child was available. Analysis revealed an excess of poliomyelitis cases in children who had been inoculated within the previous 28 days with APT, combined APT and pertussis vaccine, or pertussis vaccine alone. In these cases the arms were affected as often as the legs, and the left arm more often than the right. In those that had not been vaccinated within a month the legs were affected 2-3 times as often as the arms. In the recently vaccinated children, the limb of injection was paralyzed much more frequently than the corresponding limb in children not recently inoculated. Comparing the inoculation history in the cases of poliomyelitis with measles and 'birthday' controls, the authors found an excess of poliomyelitis cases in children inoculated within the previous month, suggesting that inoculation favored the development of clinical paralytic disease. In most of the provocation cases the onset of paralysis was 8-17 days after vaccination.
Note: one of the authors of this paper was Sir Austin Bradford Hill, an epidemiologist widely credited with determining the modern standards for establishing causality.
•Another 1950 paper investigated 375 cases of poliomyelitis during the polio epidemic in Victoria (England) in 1949, and found that 31 of the patients had been vaccinated against diphtheria or pertussis, alone or in combination, within the preceding three months, all but two of them within the preceding 5-32 days. Paralysis was most frequent in the inoculated limb.
•In 1951, the author of that paper published a second report which increased the total number of evaluated polio cases from 375 to 675. For the patients in whom exact information was available, 53 had been vaccinated for diphtheria or pertussis within three months of developing polio, with 40 of those 53 having been vaccinated within 28 days of their symptoms. In turn, he provided evidence that vaccination increased the severity of polio paralysis and that the pertussis vaccine, alone or combined with diphtheria toxoid, was more potent in provoking paralysis than diphtheria toxoid by itself.
Note: assuming the DTwP vaccine (which is no longer used in richer countries but still mass administered in to poorer ones) is a significant cause of polio, that significantly undermines the justification for many of the global vaccination campaigns.
•A 1950 paper determined that the suspected cases of polio being provoked by vaccination were indeed polio (rather than some other paralytic order) as he was able to isolate the polio virus from the stools of five children who had contracted paralysis 5-17 days after inoculation with APT or pertussis vaccine.
•A 1950 paper showed that at one London hospital,14 out of 111 patients suffering from paralytic poliomyelitis had paralysis of a limb that had received one or more vaccines within the previous two months, mostly within the previous 9-14 days. The vaccines concerned were APT (4 cases), pertussis (1 case), and combined APT and pertussis (9 cases).
•A 1951 paper evaluated a 1946 polio outbreak in Minnesota. Of 85 confirmed cases occurring within six months of an injection, 33 had had their most recent injection of diphtheria, pertussis, or tetanus vaccine—mostly combined—within the preceding month. The injected limb was paralyzed in 19 (58%) of these 33 cases, whereas of the 52 cases coming on within two to six months the injected limb was paralyzed in only 8 (15%). There was a suggestion that the first-month cases were more severe than those occurring later, and that injection was more likely to predispose to paralysis in the younger than in the older children. The interval between injection and the onset of illness in the 33 cases was mainly 5-19 days.
•A 1952 study† examined the vaccination histories of 1300 children of five years of age or under who had suffered from poliomyelitis in New York City in 1949 and 1950. A significantly greater proportion of children were paralyzed in the injected limb when the last injection had been made within the preceding month than within the preceding 1-12 months. The ratio of leg-to-arm paralysis changed from about 3:1 to about 1:1 in those injected within the preceding month. The vaccines used were those against diphtheria, pertussis, and tetanus; no attempt was made to distinguish between the effects of single and of combined vaccines.
•Another 1952 paper reviewed 2137 New York poliomyelitis patients, 6055 members of the patients' households, and 14,170 controls from adjacent households. It found poliomyelitis patients were twice as likely to have received a vaccine during the preceding two months as controls of a similar age. There was also a close association between the site of injection and the site of paralysis and the severity of the paralysis was more severe in the immunized than in the non-immunized group of patients. Additionally, unlike the other studies, they did not find the risk differed 1 month after injection versus 2 months after injection.
•Another 1952 paper† calculated that during England’s 1949 outbreak, the risk of contracting poliomyelitis was nearly four times as high in children of 9-24 months who had received an injection of combined diphtheria and pertussis vaccine within the previous six weeks when compared to a control unvaccinated group.
•A 1953 paper studied a small series of cases occurring in the south Tyneside area in 1952 and found that paralysis was more frequent in children who had been recently inoculated with APT or PTAP, alone or combined with pertussis vaccine, than in children not recently immunized, and that paralysis was commonest in the injected limb.
•Finally, in 1956, a committee of the Medical Research Council investigated the degree of risk incurred by children submitted to immunization in England and Wales. Between 1951 and 1953 all cases of paralytic poliomyelitis in children under 15 years of age were individually investigated to see if the patients had had an injection of diphtheria or pertussis or smallpox vaccine within the preceding twelve weeks. Of these 355 cases falling into this category, 222 had completed a primary course of immunizing inoculations or had received a reinforcing dose. In 132 of these 222 patients, paralysis had come on 1-28 days after inoculation, mainly in 11 to 17 days.
In certain areas of the country, the medical officers of health kept a record of the number of inoculations given in welfare and school clinics. From these it was calculated that about 1 in 37 000 vaccinations precipitated an attack of paralytic poliomyelitis and the provocation effect at most lasted a month. From this, they found the following:
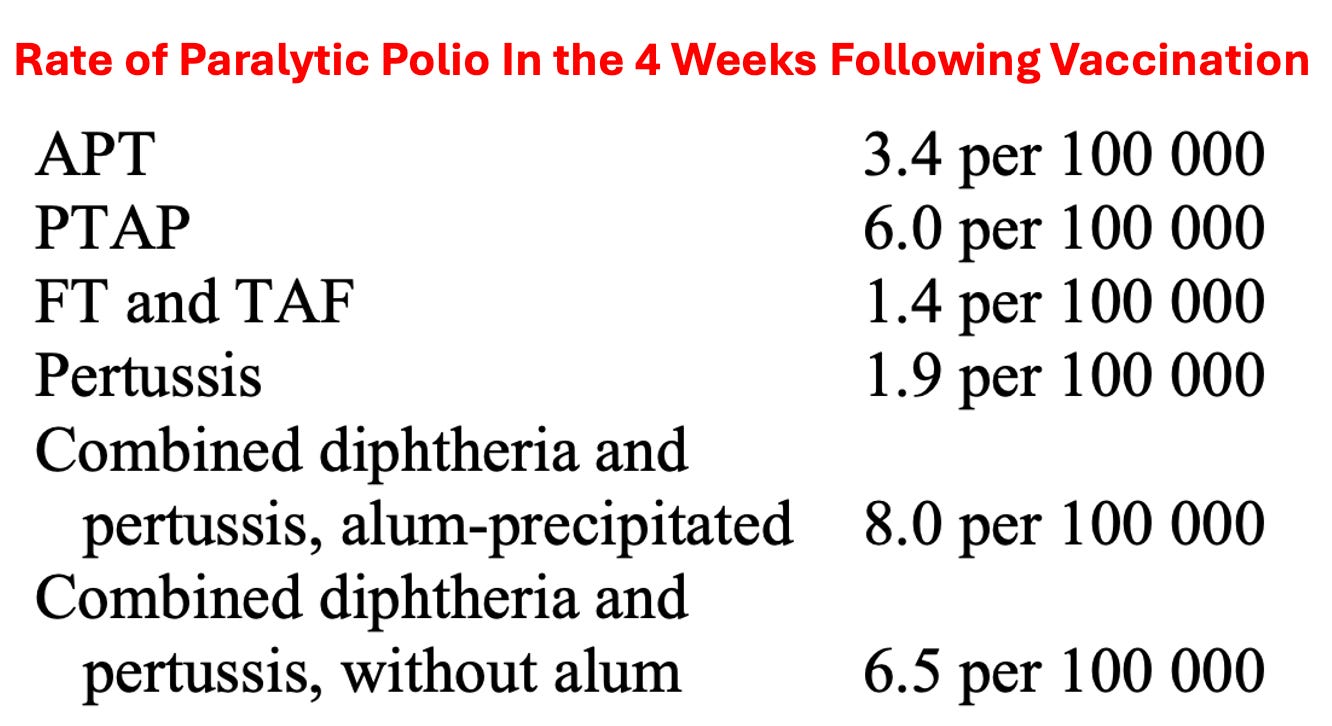
In total, it was estimated that about 13% of paralytic cases in children aged 6-24 months were causally related to vaccination. A clear relation between the site of injection and the site of paralysis was demonstrated. These findings were then substantiated by a modified investigation conducted in 1954 and 1955.‡
•A 1957 Lancet study determined that guinea pigs injected with diphtheria toxoid vaccines could then develop a hypersensitivity to the toxoid four weeks later. Interestingly, the formulations with the greatest sensitizing power (those with aluminum) were also the ones previous authors (e.g., those of the 1956 report) found were the most likely to provoke paralytic poliomyelitis. This pattern was supported by other papers as well (e.g., a 1954 one).
Note: aluminum is one of the most effective agents at impairing the physiologic zeta potential and creating blood sludging throughout the body. As discussed here, I believe this is a key mechanism that underlies many vaccine injuries. Additionally, the SARS-CoV-2 spike protein has also been shown to be highly disruptive to the physiologic zeta potential.
•A 1953 reported noted that a campaign against treponematosis (something similar to syphilis) was followed by an epidemic of paralytic poliomyelitis. Specifically, 6.2% of the children who received an intergluteal injection of arsenic, bismuth and mercury developed it, whereas only 0.5% of those who did not receive the injection did. Likewise, another 1953 report made a similar observation for intramuscularly injected quinine.
Note: I know two people who had a relative who developed polio after receiving a polio vaccination. Additionally, one of my patients had a sibling who had polio as a child and experienced a return of some of those symptoms after receiving the COVID vaccine.
Causes of Polio Disease Provocation
Despite an abundance of literature (e.g., that which I cited in this section) showing that vaccination could be immunosuppressive, the cause of provocation myelitis remained a “mystery.” To quote the Lancet:
During the summer of 1951, a medical mystery in the USA erupted into a crisis, stimulating professional debate and public anxiety. The issue was polio provocation, a health risk facing unvaccinated children in polio endemic regions. Leading specialists were at a loss to explain the condition. As the poliovirus was widespread before the discovery of an effective vaccine in 1955, evidence that some paediatric injections could incite polio infection and paralysis led to extraordinary shifts in health policy and calculated efforts to mitigate the risk. At the core of this discussion were physicians and public health researchers, whose efforts to formulate a clinical theory drove both policy and the impetus for scientists to unravel the underlying mechanism.
Eventually, the medical community settled upon the hypothesis that tissue injury caused by a needle puncture made it easier for circulating polioviruses to enter the nervous system (as those nerves were no longer protected from invasion). This argument was supported by five primary pieces of evidence:
1. Provocation poliomyelitis typically only occurred in areas already experiencing polio outbreaks and largely disappeared once polio vaccination began in the late, 1950s. At this point, the knowledge of this issue was erased from our collective memory—which in turn led to the remarkable situation where after the condition re-emerged in the 1980s due to vaccination campaigns in countries where polio was endemic, health authorities were baffled over what was happening and suspected they were witnessing a new phenomenon.
Note: I suspect the widespread resistance to routine vaccination resulting from fears of provocation poliomyelitis was a major reason why the American government chose to rush a risky (and subsequently disastrous) polio vaccine to market in spite of their own scientists warning them against doing it.
Eventually, the forgotten literature from a few decades prior was uncovered, and similar debates to those seen in America in the 1950s about the immunization campaigns happened in those nations (e.g., India). Eventually, as best as I can gather, the solution decided upon was to excessively vaccinate against polio. Unfortunately, from 2017 onwards, more cases of polio have resulted from the polio vaccine than polio itself. One of the most tragic examples occurred in India where Bill Gates diverted their health budget to aggressively vaccinating against polio, which resulted in 491,000 children developing a “polio-like” illness.
Note: the live polio vaccine contains a weakened virus that can still cause polio (and hence accounts for the majority of polio cases we see now). In turn, vaccination was also shown to provoke the vaccine strain of polio into causing paralysis.
2. A specific type of polio (bulbar polio) that led to respiratory paralysis in the respiratory tract was frequently observed to follow tonsillectomy surgeries.
Note: as discussed above, the immune system frequently becomes suppressed when someone is recovering from surgery.
3. In 1998, it was observed experimentally that injury to a nerve induced a retrograde flow, which brought the poliovirus up the nerve. This, in turn, was concluded to constitute definitive proof that this was indeed the mechanism of action.
4. Provocation poliomyelitis most frequently occurred on the same side of the body as the vaccination (and frequently on the same arm).
Note: as Wilson shows in his book, there were also decades of evidence that vaccinations could trigger paralysis through autoimmunity, so it is entirely possible some of the cases attributed to polio were instead vaccine-induced autoimmunity.
5. Provocation poliomyelitis had been observed with other injections (e.g., the previously mentioned mercury ones).
Note: mercury is immunosuppressive.
Conversely, these observations failed to account for the different rates of provocation poliomyelitis seen from different vaccinations (e.g., aluminum containing ones more frequently triggered it) or the known immunosuppressive effects of vaccination. Because of this, I am inclined to believe local tissue injury was a contributing factor in provocation poliomyelitis but it was also used as an excuse to detract from the existential risk acknowledging vaccine-induced immune suppression posed to the vaccination industry.
Conclusion
One of the major challenges with science is that nature is immensely complex, so in many cases it’s extremely difficult to precisely model—especially with a simplistic model. That reality in turn is at odds with two of the major driving forces behind science:
•The need for the human ego to feel that it can rigidly define (and hence control) reality.
•The need to use the existing scientific knowledge base to create functional products (as the sales of those imperfect products essentially "fund” science).
Because of this, time and time again, I see situations where an incomplete or inaccurate idea (e.g., a product) is forced onto the marketplace with great fanfare, but once the rubber hits the road, problems that were glossed over within the simplistic model that birthed the idea inevitably arise. In these cases, the typical response of the company that created the idea or the government that promoted it is to dismiss those issues and use its power to force the society to nonetheless accept the idea. Whenever I observe this, I perceive this situation as a square peg being created for a round hole, and the government then making the choice to leverage its power to try and pound the peg into a hole rather than get a peg that actually fits into the hole.

In the case of vaccination, there is still a great deal we simply just don’t know about the immune system, and the model we use to “treat it” is to expose the immune system to a target antigen until it develops the desired immune response. In many cases, this either doesn’t work or creates problems, and to “address” those issues, the solution is typically to expose the immune system to more and more of the antigen (e.g., with boosters), use propaganda to cover up the inevitable injuries that occur, and use mandates to deal with anyone who doesn’t fall for the propaganda.
When vaccines were originally created, modern sanitation did not yet exist (which led to many now-forgotten infectious diseases spreading like wildfire) and the options for dealing with many of the deadly diseases of the era were quite limited (e.g., antibiotics did not yet exist for diphtheria). Because of this, the public health officials of the time had fairly limited options for stopping those deaths, and hence had to utilize imperfect tools such as vaccinations or horse-derived antiserums. When you review the early history of those interventions, it’s clear they frequently failed and had a massive number of (sometimes) side effects, but at the same time—it was arguably the best option they had, so the duty of public health officials was to persuade the public to use them and eliminate anything which could create doubt in the vaccination efforts.
My belief is that led to those beliefs becoming rigidly patterned into the public health field, even when it was clear many of the previously “necessary” vaccination approaches could no longer be justified (e.g., while measles had been a problem in the past, at the time the measles vaccine was introduced, herd immunity existed in the population and measles deaths had virtually disappeared). This need to justify forcing vaccines upon the population in turn because intertwined with a “wishful” thinking vaccination would always work, and a lack of critical thinking when a major vaccination initiative was being considered.
During COVID, we in turn saw many examples of this. For example, from the start, many said that releasing a vaccine once a rapidly mutating virus (SARS-CoV-2) had already infected most of the world could not stop the pandemic and rather was guaranteed to simply promote the evolution of COVID strains that didn’t match the vaccine and hence were resistant to it—which was exactly what happened.
Sadly, because of the “wishful” thinking that surrounds vaccination, each of the past lessons is ignored and the immune system is assumed to be a magical black box that just works better each time it is forced to respond to a synthetic antigen (something which could be analogized to repeatedly kicking a horse that simply doesn’t want to move until it does). As a result, our society now faces an epidemic of “off-target immunity.”
It is thus my sincere hope that the increased scrutiny COVID-19 has brought to the practice of vaccination will force the medical field to begin acknowledging these issues so they can be addressed. Without this, it is likely we will continue to witness the mistakes of the past continue to be repeated and the warnings many, like Sir Graham Wilson, gave us will continue to fall of deaf ears.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.
I live in Melbourne Australia. We were locked up for almost two years. When there was NO covid in Melbourne and we were told that we wouldn't be allowed out until 90% were jabbed, I know of two people who went to get their jab and within a few days were sick and tested positive for Covid. One had got a drive-thru jab so exposure to anyone else was almost nil. The other had only visited a vax super-centre. Both lived alone and were not socialising with anyone else. It was clear to me then that many of the Covid cases being reported overseas were likely full of recently jabbed people who either got Covid from the jab or got a reaction that tested positive for Covid.
Louis Pasteur admitted on his deathbed that the terrain was more important than the disease. Healthy cattle grazing in a field next to unhealthy cattle...did not become infected. A healthy immune system is derived from the RIGHT NOURISHMENT in the bloodstream. The Science of Vaccines...was strewn with injured and dead people from the get-go! Starting in the 1950s vaccine promotion began. People trusted their educated doctors. They paid them for these 'vaccines.' I was one of the moms who did so. Doctors did not divulge or did not know, what items were in them? It was a 'Witchdoctor's brew' hidden by PATENTS that should never have been injected into the body of people! Aluminum and mercury. were known to create brain damage. Formaldehyde is embalming fluid. Animal viruses injected into little humans? There were many more foreign elements in these vaccines that should not be in the human body. Then the coup de grace Covid-19. which contained even more toxic substances ...and it decimated multi-millions. This was The Science of Vaccines.