Sensitivity, Specificity, and the Art of Seeking Truth
Navigating the Limitations of Knowledge

In this newsletter, my goal is to be as accurate as possible. This is in part because it fits my personality, and in part because I feel a lot of what I’m setting out to do (e.g., being a bridge for new ideas to establish themselves) is only possible if I prioritize that (somewhat analogously to Musk designing Twitter’s AI to be “maximally truth seeking”). This is essentially why I spend a lot of time looking into things I discuss here and why I do not cover a lot of topics people want me to, as in many cases, I ultimately do not know what’s actually true there, and hence can’t see a way to ensure my take is accurate.
The problem, however, with that goal is that 100% accuracy is essentially impossible to ever achieve, and if you place too much of an emphasis on trying to reach it (e.g., spending days going down each possible rabbit hole on a simple idea you are considering) it’s not possible to get anything done, much in the same way readers here would greatly prefer 52 articles, each of which I spent a week on rather than me spending a year polishing and refining 1 of them.
The dilemma I just outlined touches every part of life. For example, to navigate the world, we hold thousands of unquestioned beliefs (axioms) we assume to be true at any given moment (e.g., that the solid ground ahead of you will support you when you step onto it, that it’s a good idea to let your lungs inhale and exhale, or that the person sleeping next to you is indeed your spouse), and were we to instead constantly question each one, it would be impossible to function at all in life.
Conversely, a very strong case can be made that many of the problems people run into in life are a result of the unquestioned assumption they have. In parallel, one of my longstanding observations has been that individuals with the cognitive capacity to turn off auto-pilot and recognize which automatic assumptions or behaviors they carry merit re-examination tend to be much more successful in life.
Note: a major problem with medicine is that from day one, doctors in training are taught axioms which exclude the possibility of natural or spiritual healing occurring and hence become rigidly anchored to the lucrative materialistic medical paradigm our society follows.
Lastly, it bears mentioning that a nihilistic school of philosophy (solipsism) essentially argues that it is impossible to know anything with certainty as a sliver of doubt exists behind virtually every axiom you hold (e.g., consider the examples I mentioned above). That line of reasoning is very attractive and is routinely used in debate to dismiss all types of arguments, but inevitably collapses into an endless abyss of absurdity that is immune to outside criticism. This concept is important to highlight as while we should always question things, one should always be mindful of how probable each contrary claim or argument is and to avoid the strings of improbable ones stitched together which lack any corroborating evidence regardless of how aggressively those who share it promote it.
Note: one helpful framework to examine these claims is that after acknowledging they are possible, to ask if they are probable, as in every circumstance there are an endless number of possible (but highly improbable) claims that could attributed to what happened.
Chain Letters
In the mid-1990s, as the internet was starting to see widespread adoption, the “chain letter” phenomenon took off, where a compelling and shocking story would be found in an email from a friend you’d be compelled to forward to other people. After forwarding a few and someone scolding me, it occurred to me they might not be true, so I began researching the ones I received and quickly realized give or take every one was demonstrably fake.
However, despite pointing this out, friends and coworkers kept sending them to me, as the chain letters were designed to always make you feel emotionally compelled to share the email before you wanted to make the mental effort to think about it and vet it. As such, I soon came to the conclusion that “if the improbable events described are too perfectly lined up for a viral story, it is probably fake.” In turn, no matter how the internet has evolved since, that rule has basically always held true.
Similarly, I found that virtually every social group would have a much lower standard of proof for stories which conformed to (or supported) their existing beliefs than those which questioned it. This is most commonly observed in politics, as individuals will frequently notice instances where members of the other political party do this, but it also exists in many other spheres (e.g., a major problem in medicine is that the medical field readily adopts false narratives which support its prevailing biases while simultaneously reflexively refuses to consider those which affirm a competing paradigm). Finally, members of the group, to fit in, will frequently parrot these stories and narratives to each other and in many cases, also share them outside the group to bolster their group’s social standing.
This dynamic can also be more subtle, as rather than it just being an idea held by members of a group clearly in alignment with the idea, it is also done on an individual level where it’s challenging for an outside observer to see what group the individual is affiliated with. Similarly, in writing this publication, one of the major challenges I’ve run into is discovering that numerous stories or narratives I’ve always believed were true actually aren’t and need to first be vetted. I’d like to think I’ve gotten better at this, but a correspondence from a reader highlighted this is not always the case.
James Sims
Critiques of Western medicine (along with Wikipedia’s list of unethical human experiments), for as long as I can remember, have frequently included James Sims. This is why in last week’s article I stated:
Another controversial doctor James Marion Sims, who in 1845 began experimental gynecological surgeries on black slaves (without anesthesia—and operated on some individuals up to 30 times) and after roughly 4 years of work, perfected the surgeries enough to use them on white women (with anesthesia) after which, in the 1850s, he opened the first women’s hospital (which was mired in controversy due to how barbaric some of his procedures were, their high fatality rate, and some of the unnecessary brain surgeries he did on black children). Nonetheless, he became one of the most famous doctors in the country (e.g., he was the 1876 president of the AMA) and is considered to be the father of gynecology.
Note: many critiques of Sims are far more scathing and graphic and in 2018, after sustained protest from groups like BLM, Sims’s statue in NYC was taken down.
After publishing the article, I received this email from a reader:
Thank you for the wonderful articles you have written. I have shared them with colleagues who share similar concerns and philosophies. I am a retired Neurosurgeon [redacted]. I appreciate and share your thoughts about organ donation. I was heavily involved in brain death testing, and had a personally traumatic experience with a patient who underwent harvesting post cardiac arrest.
I recently read your article about current OB/GYN health care. Excellent. I have attached an article about Dr. J Marion Sims. Wiki has a brief history of Dr. Sims. There are some nuances to his history.
After seeing that, my immediate thought was “oh dear, have I been telling a lie about James Sims for decades?” followed by “I never thought about it before, but I have been emotionally invested in believing a negative narrative about James Sims because the story I heard was so personally triggering for me that I did not vet it first” (not unlike what compels one to share chain letters).
I then read that article (which you can too here) and found out that:
Most of the above allegations against Sims are not supported by the historical record or the clinical reality of the time (where many things we take for granted now instead were very difficult to do). Rather, they were strung together to support a narrative of white doctors ruthlessly exploiting black slaves.
The gynecologic condition Sims was treating—vesicovaginal fistula (and other similar ones)—were devastating for those who had them and incurable at the time, so the enslaved women he operated on were desperate for relief and willingly consented to the procedures.
Sims didn’t use anesthesia mainly because ether was still brand new, highly controversial, and carried real risks. He (and other surgeons) didn’t think the pain of these particular operations justified the dangers, and he applied the same standard to white patients as well.
The surgeries he developed were the first consistently successful repair for this condition and basically founded modern gynecologic surgery, which is why he rose in the field.
A lot of Sims’s behavior toward these women lines up with someone genuinely trying to help them rather than just exploiting them—he operated at his own expense, got their cooperation (they even assisted in each other’s surgeries), publicly acknowledged his debt to them, and kept going because they pushed him to continue when he wanted to quit.
So, I have to say I never expected to defend someone I despised as much as Dr. Sims, but since my priority is being accurate, I felt I needed to as I lied about him in the previous article.
Note: many other criticisms have been leveled against Sims besides the one I touched upon. They may be valid; my point is only on correcting what I was inaccurate about.
Sensitivity and Specificity
One of my favorite concepts in the philosophy of science is “sensitivity and specificity.” This dyad denotes how likely you are to identify what you are trying to get (sensitivity) and how likely you are to erroneously misidentify your target (specificity). In medicine, this concept is raised to highlight that no diagnostic test is perfect, and if you prioritize one of these, you typically worsen the other (e.g., if a cancer test is too liberal with its criteria, it will cause issues by falsely diagnosing people with cancer whereas if you design a test to avoid false positives, it typically will also have a higher rate of missed cancers).
Because of this, a major focus in diagnostic testing is to identify which tests have the best balance between the two, and to identify which situations merit tests which emphasize sensitivity and which merit tests that emphasize specificity (or a combination of both). Conversely, some of the biggest debacles in medicine result from this principle being disregarded. For example, to ensure the COVID nasal PCR tests did not miss any cases of COVID, their sensitivity was raised to the point they frequently had false positives to the point large segments of the population concluded the tests were a complete joke.
After I was introduced to the concept of sensitivity and specificity, it dawned on me this concept extended far beyond medical diagnosis, and underlies many different challenging situations faced by our society. For example, much of the debate with criminal justice and police boils down to prioritizing sensitivity (preventing as many criminals as possible from harming the population) or specificity (not falsely arresting and harming innocent individuals), and once one goes too far to either extreme, clear issues happen on the other hand (e.g., a culture of lax policing and prosecutions spikes violent crime whereas authoritarian societies that believe in guilty until proven innocent have populations who are terrified of the police and many innocent prisoners).
Unfortunately, once these debates become contentious issues, rather than the goal being to find the best way to maximize sensitivity and specificity, one side will typically identify with the sensitivity position, the other with the specificity position, and then each will be excellent at arguing for why greater sensitivity (or specificity) is needed but simultaneously incapable of seeing the downsides to their position on the other end of things. Ultimately, things typically settle out in a compromise position where the way sensitivity and specificity are addressed is “good enough” (rather than a rationally designed one aimed to maximize both), and in times when the society becomes more polarized, shifts more towards one or the other, and then later inevitably goes back in the opposite direction once the flaws of the previous became clear, and either societal polarization decreases or the opposite side comes to power.
Cognitive Sensitivity and Specificity
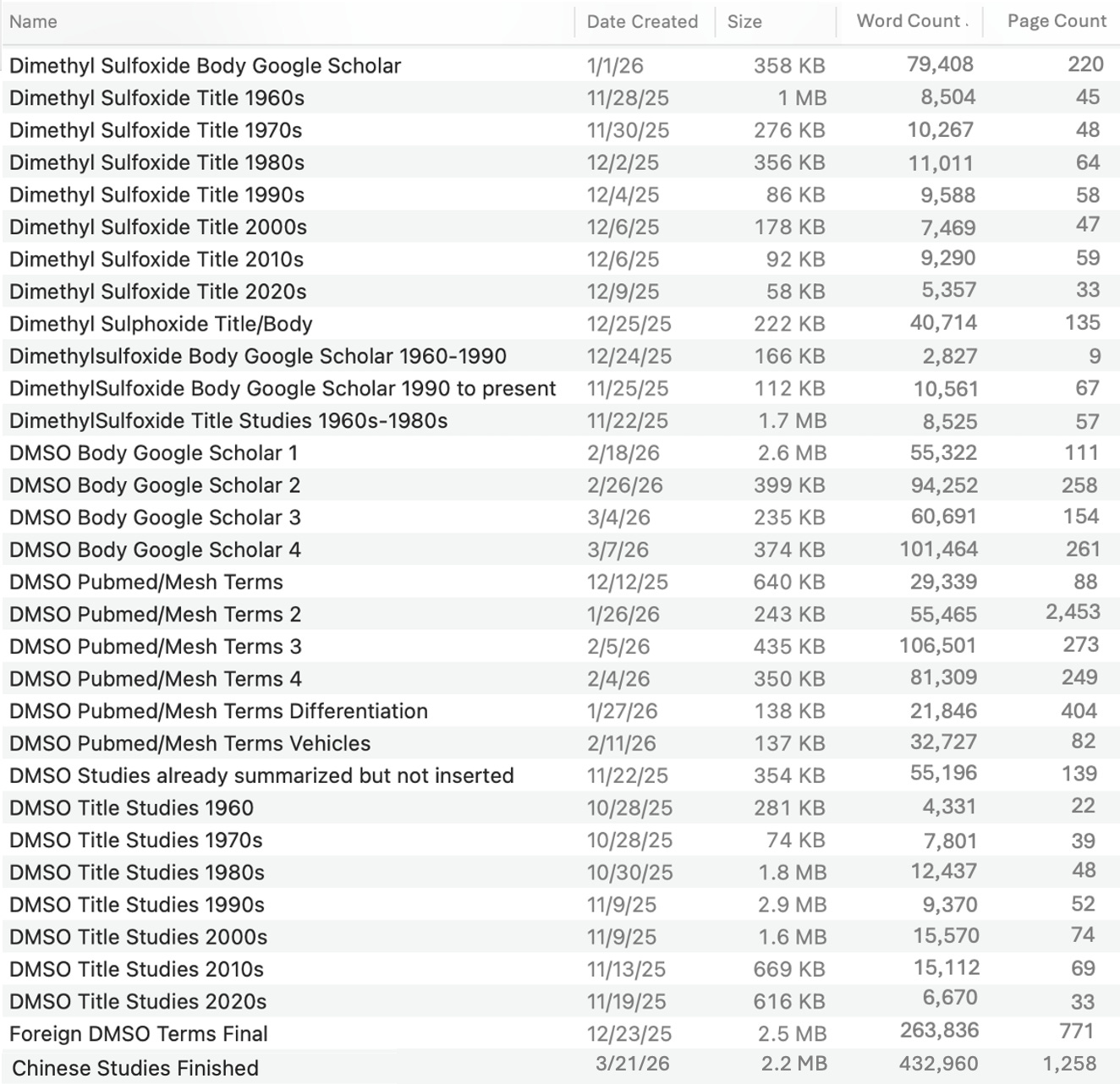
Likewise, sensitivity and specificity play a critical role in shaping our own cognition and how we navigate the world. For example, in the DMSO research project I’ve been doing full time since October, I essentially concluded that to do what was needed for DMSO, I would need to go through every applicable database, search each one for the terms used for DMSO, and filter those results to identify all the medically relevant studies, and then summarize them so I could sort them by subject (which I am currently doing for a requested DMSO neurology series).
The problem with this is depending on the query, that the results got thousands, tens of thousands, hundreds of thousands or millions of results, and while I can consciously process large bodies of data, the larger results greatly exceeded anything my mind could do. Because of this, a lot of the project was essentially trying to find a way to achieve sufficient sensitivity (so virtually no medically relevant study was missed) while simultaneously having a hard enough filter that the final outputs didn’t overlap and were constrained to tens of thousands of results (which was possible to manually review). Likewise, when manually reviewing those outputs, I was continually trying to consciously calibrate my mental filters and cognitive algorithms so I didn’t miss anything relevant but simultaneously could move at a past enough pace through the lists (by not spending time or focus on non-relevant results) and that the project could be completed in a timely fashion that I had enough cognitive energy to sustain completing it.
Ultimately, while very challenging, I was able to pull it off, and am truly grateful there was a way to do this (as I am doubtful it will ever be done again and hence felt an obligation to do it properly), but at the same time, will likely never undertake a similar endeavor because of how much it took out of me to do it.
Note: I initially thought ozone would be a much harder topic than DMSO (due to the larger volume of search results) but in the process of figuring out how to do this task, realized that ozone is actually much easier to do as the medically relevant results are much easier to separate out at the start (and hence is next in the queue after this project).
All of the previous may sound a bit abstract, but the reality is that every day, we are continually making the choice to screen out or ignore large pockets of data we are exposed to, while simultaneously devoting our limited cognitive resources to focusing on the things our mind prioritizes.
However, unlike the process I described above, this filtering is typically not conscious (or only partly conscious such as when deciding who in a group we want to approach and who we want to avoid), and in many cases, is externally hijacked (e.g., marketing and propaganda revolves around getting people to focus on specific things and ignoring others). I mention all of this because my consistent experience has been that people who consciously choose how they want their mind to filter reality tend to be much more successful (and happy) in life, particularly if they extensively deliberate on the merits of cognitive sensitivity and specificity in each situation and look for the most appropriate balance that best helps them.
Note: it’s impossible to ever be perfect at this, and a lot of life is being willing to recognize how your sensitivity or specificity was poorly calibrated. For example, even though I actively try to do this, as the case with James Sims showed, my choice to embrace and take the negative narrative about him at face value illustrates I had poor specificity there which caused me violate my core priority (not publishing inaccurate information).
Medical Philosophies
The way one chooses to see or practice medicine is also heavily shaped by how they prioritize sensitivity and specificity in a variety of contexts (e.g., many doctors fixate on the rare diseases vaccines sometimes prevent but simultaneously ignore the common side effects of vaccination and hence religiously support vaccination).
With medicine, I essentially believe that:
•Most medicinal interventions, due to the nature of how medical science interacts with the body, cause harm (that is sometimes obvious and sometimes subtle).
•Many medical interventions transformed humanity, and there are many problems we never think or worry about now which were major issues prior to medical science solving them.
•The relative risk of medical therapies greatly varies, but rather than view them as distinct entities, they are frequently seen as all being good or bad. Likewise, many conventional therapies, while not ideal, are often the best option many people have.
•With most medical issues, numerous viable approaches exist to treat them which have different upsides and downsides. Unfortunately, since there is not an open discussion on this, clearly suboptimal therapies are routinely chosen for patients (with significant consequences frequently following).
•I have seen many people be harmed by unnecessary medical procedures (who in many cases were warned by friends or family that harm could occur beforehand) but I have also seen people who were ideologically opposed to the medical system be harmed or die because they refused standard care for an issue which is straightforward to treat with conventional medicine.
Or, taking a step back, what this essentially means is that correctly engaging with medicine is a sensitivity-specificity issue, where you have to understand the subject well enough to be able to gauge where this best lines up in each instance.
In my own case, my own philosophy leans strongly towards avoiding harm, so I hold the position I would rather do nothing than something I feel holds a potential risk of harm.
Note: this is also why I will not give quick answers here on how to use therapies I think need to be well understood to avoid some people having negative experiences with them and why I have not promoted a number of compelling popular alternatives therapies as I am still not sure if they are satisfactorily safe.
Generally, this philosophy has served my goals well, as I’ve avoided making patients worse (with most of the exceptions being instances where the chronically ill patient had a partial improvement, then they desperately wanted more and were leaving the area for a while, so I did more than I was sure they were ready for which then set them significantly back). However the downside to my approach is that for a lot of people there is a massive cost to going slowly into a protocol and waiting much longer for a treatment response that far outweighs manageable adverse reactions they could have to therapies (but conversely, in many cases, there is an even greater cost if a protocol is done too quickly for it to ever have a chance to work).
Likewise, while my philosophy and personality is well suited to outpatient (non-emergent) issues, it does not work for more serious and pressing issues where you have to routinely utilize therapies with inherent degrees of harm to save people’s lives, so I have immense respect for the doctors who practice differently from me in those high-stakes contexts and were I there now, I too would adjust how I prioritized the risks and benefits of medical therapies.
Note: in many cases, I find appropriately utilized natural therapies can prevent hospitalizations (sometimes even when given in the ER shortly before admission), but at the same time, I do not like to rely upon this, as bad things will happen if hospital care is delayed for emergent conditions.
Cancer Treatment
One of the most challenging areas where these competing priorities converge is with cancer treatment as:
•Many conventional therapies have horrendous, unacceptable side effects and poor efficacy.
•Other conventional therapies work fairly well, and make previous death sentences survivable (however these therapies are often extremely expensive and their side effects significantly impair one’s quality of life).
•Many safer and cheaper natural therapies exist which sometimes independently treat cancer.
•If conventional cancer treatment is delayed (e.g., due to exploring non-toxic alternatives or a waitlist already existing for conventional care), it can worsen the condition to the point an acceptable outcome with conventional care is no longer possible.
Because of this, cancer patients frequently run into a “lose-lose” situation where there is no clear answer on what to do, alongside a great deal of stress and conflicting voices clamoring in their ears for them to prioritize either sensitivity or specificity with conventional or alternative treatment options (to the point one of the most helpful things you can often do for a cancer patient is have a friend serve as intermediary to field all the people who are bombarding them with advice and worry).
My “solution” to this dilemma mirrors how I approach emergent conditions.
•If time exists, I try natural therapies before conventional care.
•I always keep an eye out for the cases which are likely to fully respond to a natural therapy or safe pharmaceutical protocol (e.g., around 10% of cancer patients have incredible responses to protocols that use repurposed drugs like ivermectin), which cases have a clear underlying issue precipitating the cancer (e.g., estrogen dominance, key micronutrient deficiencies, or retained emotional trauma) that must be treated in tandem with whatever protocol is chosen, and how to optimize the chosen natural therapy (e.g., ivermectin can create neurologic issues at higher doses, but the need for high oral doses can be bypassed if ivermectin is mixed with a paste and applied directly to the skin above a tumor—where it frequently works much better than any oral protocol).
•In most cases, I default to the natural therapies supporting the conventional ones, as conventional cancer outcomes and side effects can be greatly improved with the correct holistic therapies (e.g., UVBI is excellent for mitigating chemotherapy side effects, and in most patients we see cancer outcomes significantly improve if therapies like the repurposed drug protocols are used in conjunction with them).
•When possible, I try to help make the conventional cancer protocol be more targeted to the specific patient (so lower doses and more effective regimens are used).
Therapeutic Precision
In many cases when an impossible balance has to be struck between sensitivity and specificity, an out-of-the-box solution exists which solves it. In the case of medical approaches, I gradually realized the following:
•The side effects from medical therapies typically result from them affecting areas besides the intended target (e.g., since most pharmaceutical drugs work by inhibiting enzymes, they will frequently either inhibit necessary functions of the target enzyme or inhibit other similarly structured enzymes in the body) and the body having a pathological compensation to the unnatural shifts the pharmaceuticals create (e.g., if an enzyme or receptor is chronically impeded, the body will try to fix this by upregulating that protein, while if it’s chronically stimulated, the body will downregulate it—which frequently creates addiction as higher and higher doses of the drugs are needed).
•The higher a dose of a therapy is used, the more likely it is to accomplish the intended effect and reach the desired target, but simultaneously the more likely it is to also hit unintended targets and cause issues (particularly in sensitive patients). While there are many ways to navigate this dilemma, the most common approach has been to simply ignore or dismiss the downsides to overdosing and focus solely on creating the desired effect.
•Natural therapies tend to be much weaker than conventional therapies. As such, they rarely create the same significant side effects, but also do not create the immediate significant shifts observed with pharmaceutical drugs. However, you can also overdo natural therapies (e.g., we see tons of people who are on large numbers of poor quality supplements that are not benefitting them, and they feel significantly better once we cut them down to the 20% that are helping).
As such, on one hand, I held a strong bias towards avoiding pharmaceutical therapies in favor of natural ones (along with minimizing prescriptions). However, I also feel it’s important to never be dogmatic, and from exploring pharmacology, I gradually discovered some drugs (e.g., ivermectin) have excellent risk/benefit profiles for illnesses that clearly justify their use, and that with many borderline drugs, lower doses of them frequently made it possible to get key benefits without significant side effects.
More importantly, as I pondered the dilemma of when to utilize the stronger conventional therapies, I realized a completely different solution to the question existed: if therapies are precisely targeted to the needed issue, much lower doses are needed to create the intended effect.
As such, one of the reasons why I can get away with using “weaker” natural therapies for difficult conditions which frequently require much stronger measures is because I found ways to ensure the therapy went directly towards addressing the root cause of their issue. Likewise, since pharmaceuticals are not my default approach, I can more easily recognize the cases where a specific pharmaceutical is likely to directly target the patient’s issue (at which point lower doses and shorter courses of treatments can be utilized).
Sadly, in contrast to this mindset, medicine revolves around creating standardized protocols everyone is subjected to, with the fraction of people who react poorly to that being seen as a necessary cost of doing business and then largely ignored.
Note: many different approaches have been developed over the years to improve the selection and targeting of therapeutics (too many to cover here). Generally speaking, the ability to do this is one of the key skillsets which distinguishes renowned healers from other physicians in the integrative medical field.
Conclusion
This newsletter has always been an exercise in pursuing accuracy within an imperfect world where complete certainty is impossible but the best attempt towards it must nonetheless be made. As such, I’ve tried to share some of the strategies I’ve found which are the most useful for bridging that divide and moving from reflexively believing emotionally provocative information to one that tries to calmly assess the sea of information around you and find the best path forward as you navigate the sensitivity and specificity challenges life throws at you.
In many cases, I find the greatest obstacle to doing this is within the person, as from birth, we are trained to prioritize protecting our ego and being right—even if that forces us to commit to an incorrect position or keep repeating the same counterproductive mistake. When I wrote this article, I did so in part because I felt obligated to correct the mistake I made with Sims, but also to illustrate the importance of having a paradigm that prioritizes truth and accuracy over being right and how in many cases (regardless of how much your ego lies to you) that is not something you can ever fully achieve, but rather simply a destination you keep gradually moving closer towards.
I thank each of you for your support which makes this newsletter possible, and hope this gives you some useful ideas to ponder.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.
I appreciate your thoughtful and thought provoking posts. As an accidental drug safety advocate, I wish more doctors had your more cautious approach to treatment. Less is more. Harms from medicine is more prevalent than we have been told.
I used Ivermectin cream with a little added DMSO to treat a bcc spot on my nostril successfully. My dermatologist had pushed me to get a MOHS procedure which can be disfiguring. I'm glad that I questioned the need for a treatment that radical for a tiny red dot........which was not life threatening.