How Vaccines Alter Intimate Relationships and Gender Identity
Exploring the links between vaccination, human connection, autism, and sexual orientation


Story at a Glance:
•For over a century, a large volume of evidence has been compiled showing that vaccination can cause a wide range of disorders (e.g., autism and middle ear infections—both of which will be explored in detail here), many of which are neurological or autoimmune in nature.
•What’s less appreciated is the myriad of subtle personality effects vaccination can create, many of which are observed after cases of infectious encephalitis, and previously were labeled as “minimal brain damage” by America’s health authorities.
•In the previous article I reviewed how those changes can give rise to ADHD, impulsivity, and violent or sociopathic behavior. In this article, I will instead focus on how they create many of the disconnections which make romantic partners so difficult to be with and how they can alter one’s sexual identity.
Note: in my initial polling, I found women who were old enough to know men before and after the most problematic vaccine rolled out witnessed the changes I described, and I would thus greatly appreciate if you could provide your input as well.
One of the few things which is more controversial than linking vaccination to autism is linking vaccination to transgenderism, and for that reason, I’ve avoided discussing the topic. Recently however Steve Kirsch (a friend whom I owe for a debt of gratitude to for creating this publication) contacted me and asked me to debate his data which strongly supported the connection between vaccination and transgenderism. After doing so, I then agreed to write an article on it, so here I will attempt to provide a balanced perspective on this complex question.
From my exploration of this subject, I found that there is a large degree of evidence which makes a compelling argument in support of Steve’s contention but very little direct evidence in support of it. As such, this is an area which clearly requires more research, and it is likewise doubtful that will ever be conducted within academia.
Note: I am fully aware of all the memes that make fun of “antivaxxers for blaming everything under the sun on vaccines,” so a lot of thought went into if I wanted to touch this subject and exactly how to approach it.
The Mass Vaccination Of Society
Over the weekend, I published one of the most popular but also profoundly disturbing articles I’ve written in this publication. In that argument, I sought to make the following arguments.
1) Vaccines frequently create “off-target immunity” and pervasive microclots throughout the body which often leaves the body in a permanent state of shock where the cells are unable to return to their normal metabolic function. This in turn creates a myriad of side effects throughout the body, particularly ones of a neurological or immunological nature.
2) In parallel to the mass adoption of vaccination, there has been a massive increase in neurological and autoimmune diseases which spiked each time a particularly dangerous vaccine entered the market. Most conventional authorities in turn insist “correlation is not causation” and that “there is no evidence vaccines are doing this” despite the fact the increase of the diseases has remained a mystery for decades and numerous smaller studies (e.g., the clinical trials for the HPV vaccine) have shown vaccines will cause the same diseases we see exploding in society.
3) A curious embargo exists on testing vaccines for safety. As a result, the basic trials we would expect to have been done to assess whether the CDC’s vaccine schedule is safe have never been publicly conducted. Moreover, no independent researcher has ever been given access to the large databases that could easily demonstrate if vaccines were indeed “safe” or “effective.”
4) Nevertheless, a variety of independent studies have been conducted. Each of these has found that vaccinated individuals, when compared to the minority of the population who are unvaccinated, are many times more likely to develop a wide range of illnesses (e.g., ADHD, asthma, depression, eczema, epilepsy, a variety of learning disorders, middle ear infections, sinusitis, etc.).
Note: since there are a lot of different conditions, in the previous article, I included tables showing the overall increase in a variety of chronic disorders found in each of those studies (with many having over a 10-fold increase in the vaccinated).
5) In medicine, it is difficult to find something unless you know how to look for it. While overt vaccine injuries are somewhat well understood by those investigating vaccine safety, what is far less appreciated is the far more frequent but less overt neurological consequences of vaccination. Many of these in turn mirror what was observed to result in patients who had recovered from episodes of encephalitis (brain inflammation) and hence became much more common once the original DPT vaccine (which frequently caused encephalitis) began being mass deployed upon society in the 1950s.
Note: the original DPT vaccine was also strongly linked to causing sudden infant death syndrome.
6) 34 years ago, a remarkable author (Harris Coulter) made a strong case that these post encephalitic complications of the DPT vaccine were dramatically altering America and were responsible for a variety of social changes we had seen which paralleled DPT’s adoption. Coulter specifically focused on the link between violent crime and DPT encephalitis, but also touched upon the variety of learning disabilities (and physical deficits) that frequently resulted from the DPT vaccine, and which are often seen within violent criminals. Assuming Coulter was correct, this in turn completely upends both the liberal and conservative notions about criminal justice.
The previous article, in turn, as I learned through the comments, was a very sobering read for many of the readers. For example:
“Thank you. As I sit here reading these articles, I realize that without people like you - people like me might just one day die of grief and loneliness. The guilt is incalculable for me. My oldest - a felon, severely ADHD, hyperactive, and always sick. Second child - now permanently disabled by Lyme. My last, now wasting away with UC, major depressive disorder, autism, and worse - was once on his way to being a Navy Seal with a PhD in physics until the suffering became too difficult and caused a complete collapse. Who cares for them when am gone? No answers. Thank you for what you are doing. In light of this link I am sending, I have frequently floated the idea of having community contacts for support - be it food, simple home care, driving to appointments, etc. for aging parents with autistic adult children. Please watch this.”
Note: I specifically wrote the previous article because it provided the evidence needed to support the arguments I will present here. This article hence will make much sense if the context from the previous article is incorporated as well.
Vaccines and Autism
Typically, when the notion that a case of regressive autism in association with a vaccine is mentioned to a member of the scientific orthodoxy, an indignant and patronizing response follows which is some variant of the following:
The only reason people believe that is because Andrew Wakefield wrote a fraudulent paper that falsely claimed a link existed between autism and vaccines and the Lancet made a grave error in not catching this before it published it. That paper was retracted and Wakefield lost his license for scientific misconduct, so you have no basis to believe this thoroughly debunked claim, and hundreds of studies since then have all found that vaccines do not cause autism.
What I find remarkable about this argument is that beyond completely mischaracterizing Wakefield’s paper, it suggests that prior to Wakefield’s paper, it had never occurred to people that vaccines could cause autism. Hence, according to the orthodox, anyone believing that vaccines cause autism was simply being manipulated by a hysteria Wakefield deliberately created (which he allegedly did because he was bribed by parents of autistic vaccine injured children to fabricate evidence to support their case).
The problem with this argument is that it disproves itself (as if parents were willing to fund a study to see if vaccines caused autism, the idea already had to exist prior to the Lancet paper) and because people had been alleging this link decades prior to the Lancet article (e.g., Coulter’s 1990 book cited decades of work linking vaccines to autism). Despite this absurdity however, it’s been remarkably effective at silencing any parent who questions why their child experienced rapid developmental decline after vaccination, and likewise sending a very clear message to every doctor and medical journal to never repeat the Lancet’s “mistake” and publish anything critical of vaccination (whereas in previous decades hundreds, and likely thousands, of critical articles had been published throughout the medical literature).
Wakefield’s story and what he went through is hence extremely pertinent to the current events:
Note: the same neurological issues seen in individuals who have recovered encephalitis (e.g., cranial nerve defects and permanently impaired cognition) are frequently observed in autistic individuals. A critically important point about this is that while a single label “autism” is used, two very different conditions exist. In one (the more common one), the individual has a significant intellectual disability, while in the other (the more commonly discussed one), the individual has remarkable cognitive aptitudes in certain areas accompanied by certain characteristic social and emotional defects that make interpersonal interactions a continual challenge for them. This in turn makes it very unfortunate the educational system treats each type as being equivalent and often houses them in the same classes as this greatly stifles the educational development of the gifted autists.
Recently Steve Kirsch started looking at the link between vaccines and autism, and in an attempt to bring attention to the issue, raised three very important points:
1. Contrary to popular belief, there is actually a great deal of compelling evidence linking vaccines to autism. For example, regressive autism always develops shortly after vaccination—but never before, something that cannot happen unless one causes the other. Likewise, there is a significant amount of evidence correlating vaccine uptake with autism rates.
2. There is presently no accepted explanation for what is causing the explosion of autism we are facing.
3. The explosion of autism is one of the costliest diseases facing our country, so decades of hand waiving that has insisted there’s no scientifically valid explanation for this explosion doesn’t cut it.
You might notice how these three points mirror what we are now seeing with the massive wave of (often unmistakable) side effects from the COVID-19 vaccines.
Note: For those interested in learning more about vaccines and autism, I would strongly recommend reading Kirsch’s article. He does a good job of concisely presenting some of the most compelling evidence (e.g., specific cases where vaccination was irrefutably linked to autism and the hundreds of papers on the subject), and my article on this topic which describes the mechanisms for how vaccinations cause autism.
Interpersonal Dynamics and Vaccination
I have long believed many “psychiatric” issues are neurological in nature due to how rapidly I saw them develop in conjunction with classic signs of brain damage following a pharmaceutical injury and hence believe it is inappropriate to treat these issues psychiatrically (rather the organic issue causing it must be addressed). Sadly, as Coulter showed, that recognition long ago became a forgotten side of medicine:
Researchers such as Samuel Torrey Orton in the 1920s realized that "emotional disturbances" originate in neurologic reality. But this insight was lost after World War I when psychology, psychiatry, and especially Freudian psychoanalysis became overwhelmingly popular medical disciplines, while the link between mental illness and neurology was largely broken.
Since the 1950s American parents and their children have been continuously subjected to psychologizing and psychiatrizing on a vast scale. Geschwind wrote in 1982 that this prejudice "makes it extremely difficult to accept that there are instances in which difficulties in emotional adjustment are the primary result of alterations in the brain.
Another of Coulter’s key points I’d long believed is that in addition to the overt brain damage created by the DPT vaccine, a wide array of more subtle cognitive and behavioral issues were created (e.g., minor learning disabilities or a tendency towards violent behavior). Many of the post-encephalitic “psychiatric” complications in turn were eye opening as they described both what I and in turn, many readers, realized we had been seeing around us.
Note: in the 1950s, after this brain damage started emerging in society, it was widely recognized and before it became normalized a few decades later, the leading medical authorities referred to it as “minimal brain damage.” In the previous article I mapped out the most overt characteristics of MBD as they dovetailed with the symptoms observed in post-encephalitic patients. The most important thing to recognize here is that MBD was a real and widely acknowledged condition before it got buried.
The more subtle “personality” changes created by MBD included:
•A tendency to want to listen to repetitive music since it provides stability and anchoring for their minds.
Note: in Chinese medicine, all phenomena that emerge around us are ascribed to one of the five elements, and in turn, a detailed system has emerged that charts how each of them express themselves under a variety of conditions. One of those elements is “metal” which is characterized by order, structure, and mental energy (e.g., highly intellectual tendencies). I mention this because one of the things I realized is that the repetitive music the vaccine injured men I’ve gotten to know listen to is almost always of the metal element.
•A hyperactivity that inhibits their mind from settling and being fully connected with what’s around them.
Note: this symptom was typically observed in men, whereas women were instead more likely to have a refusal or reluctance to eat (anorexia nervosa) or a tendency to eat too much and indiscriminately (bulimia), both conditions prominence in the 1960s.
•Varying degrees of amnesia and an inability to remember one’s past misdeeds.
•A variety of difficulties with emotional expression, empathy, and emotional connection. This goes in parallel with a weakness or paralysis of the facial muscles that cause a "mask-like" appearance or a smile often described as “fixed” or “frozen.”
•A tendency to sometimes have an obsessive focus on a single thing in their environment.
•Being absorbed in their own reality, sometimes losing awareness of what is happening around them, appearing absent minded, and having difficulty looking into another’s eyes.
•A variety of difficulties with their own physical integration (e.g., coordination) and physical intimacy with others (typically defaulting to mentally carrying out algorithmic movements which don’t have any passion, spontaneity or connection behind them).
•A variety of speech issues including oddities of articulation or intonation (e.g., slow, monotone, loud sing-song, incontrollable sounds, unmodulated, sharp, or peculiar syllabilization, and pressured speech), where the voice becomes monotonous and less resonant. The speaker in turn “is unable to modulate his tone of voice in response to the environment.”
•A variety of auditory processing disorders (discussed in the previous article) also occurred. While not mentioned in the MBD symptoms, I’ve noticed many autistic children and neuroatypical adults (which I equate to minor autism) frequently are very sensitive to sound (possibly because the function of the nerve which dampens sounds by tightening the ear drum is impaired). In turn, they often find wearing good quality ear plugs (e.g., silicone ones) makes it much easier for their mind to relax and soften during day to day interactions (as they can still hear what people are saying but the ear plugs create a soothing auditory “dampening”) and much easier for them to sleep.
•An inability to direct their attention within a complex environment and hence react equally to a wide variety of stimuli. This is disorienting for them, and often results in their cognitive processes not being integrated or logically sequenced. In turn:
They are present-oriented, [highly impulsive], matter-of-fact, narcissistically egocentric, rambling, circumstantial, unable to get to the point. They cannot joke, since a sense of humor presupposes a background of abstract knowledge against which the situation described in the joke is seen as funny.
This underdeveloped emotional side is called by various names and described in various ways: "immature personality disorder," emotional "blunting," "diminished capacity for positive and negative affect," "marked impairment in the capacity to sustain lasting, close, warm, and responsible relationships with family, friends, or sexual partners," "lack of capacity to form emotional relations," "diminished capacity to experience pleasure," "lack of empathy," "withdrawn behavior," "inability to sustain affection," "poor peer relations," "no steady friends."
Note: this is similar to a list of changes observed in post-encephalitic patients (e.g., egotism, narcissism, ego weakness, alienation, impulsiveness, emotional lability, flat affect, anxiety, paranoia, impatience with criticism, rage, depression, and suicidal impulses).
Precocious sexuality is another way of coping with ego weakness [and neurologic weakness] and feelings of inadequacy, and, in an exaggerated form, is commonly encountered among the minimally brain damaged….Lack of capacity for genuine emotion generates the need for overindulgence in a purely sexual form of relating. And the resulting hypersexuality is not limited by any emotional ties.
When I learned all of this, it transformed my interpersonal relationships. It made me realize that many of the people I’ve found to be “so difficult” were, in fact, simply brain damaged (and made me feel quite guilty over how I’d treated some of these people in the past). This allowed me to both have compassion rather than frustration for these people and see how to bypass the glitches within their minds so that I could have more productive interactions with them.
Additionally, as I read through Coulter’s list, something kept on jumping out at me. He was listing most of the typical things women find extremely frustrating about men (with men being more likely to develop neurological complications from vaccine encephalitis), particularly within a romantic context.
Note: he also highlighted a few of the things men find frustrating about women, but the correlation was much less stark here.
As I’m too young to have been able to observe this, but I’m blessed to have numerous witty and sharp female subscribers who have been around long enough to notice this, I asked a few of them if they’d noticed the men who were born after World War 2 (as this is when mass DPT vaccinations began) were different from the men before. To quote one reader:
I would hence greatly appreciate your honest answers to these polls.
Note: the above poll is meant to refer to the minority of the population which never vaccinates, as in theory, they should demonstrate the same changes seen in the pre-DPT era.
Note: since what I can ask within these polls is quite limited, I would greatly appreciate reading your more of your thoughts on this in the comments.
Steve Kirsch’s Survey
Recently, Steve Kirsch published a survey of 13,000 people to assess health differences between the vaccinated and unvaccinated.
As shown in the previous article, Kirsch’s survey found a variety of common illnesses were 2-10 times more likely to occur in the vaccinated than the unvaccinated.
I in turn am inclined to believe the survey’s results were accurate as:
•Its results were recently validated by an outside statistical expert who looked at the raw data.
•As shown in the previous article, its results are consistent with what each other survey in this area has found.
•Its results were consistent with what I have anecdotally observed.
I will illustrate the above points with the most common illness children see a pediatrician for, (typically painful) middle ear infections (otitis media), which for context, happens, 30 million times each year in the USA. Kirsch’s survey found vaccination increased the likelihood of a childhood having frequent middle ear infections 5.1X. Another previous survey of 1544 parents found vaccination increased the risk of middle ear infections 900X), while a different survey of 405 vaccinated and 261 unvaccinated found a 3.8X increase.
Similar data was also found from the records of pediatric practices. In one study of 2047 children, vaccination caused a 2.49X increase in middle ear infections. Finally, a pediatrician with a large practice who analyzed his charts found a comparable (3X to 7X) increase:
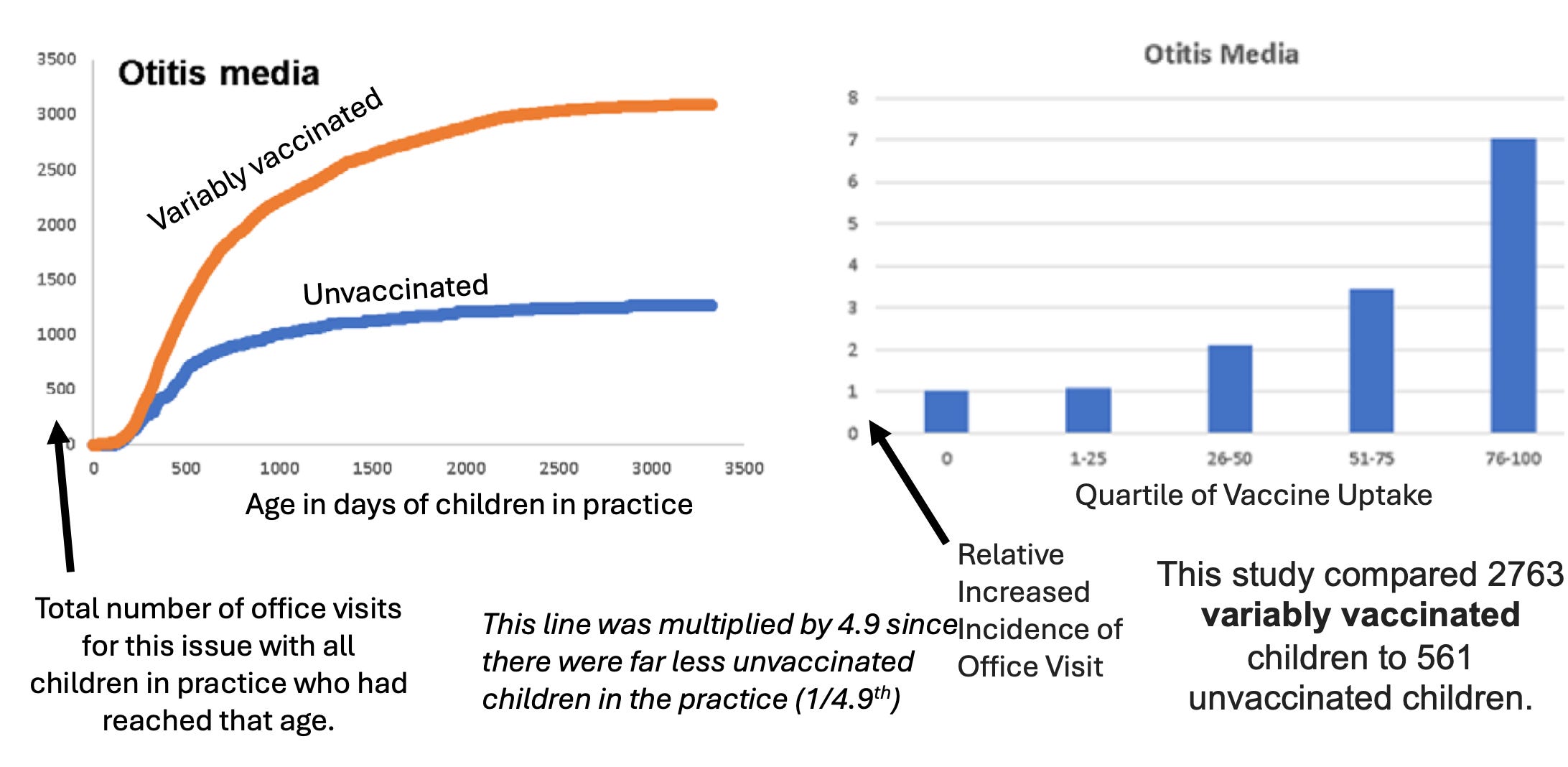
Note: his study likely underestimates the amount of illness caused by vaccination as most children in it were ”variably vaccinated” and hence exposed to a significantly smaller and gentler vaccine schedule.
Conversely, there are also many compelling anecdotes. For example:
•Numerous readers here have shared that their first few children had middle ear infections so frequently needed ear tubes, but when they chose not to vaccinate their youngest child (as they became awake to the vaccine issue), that child did not have any ear infections.
•Many physicians have shared that they have observed that vaccination, particularly the DPT vaccine, frequently causes otitis media.
•A good friend’s relative was a physician who stayed in an Ashram in India. To help the children there, he eventually decided to vaccinate them for DPT (with the original whole cell one). After he did this the majority of the children there developed a middle ear infection. In comparison, he did not recall seeing a case of otitis media in the preceding years he had been there. This story specifically convinced me DPT irrefutably caused otitis media.
•Archie Kalokerinos MD who served in the Aboriginal communities in Australia played a pivotal role in proving that the DPT vaccine caused sudden infant death and that it could often be prevented by providing vitamin C to the child (as vitamin C deficiency was rampant there). While SIDS was the focus of his memoir, he also was able to clearly link DPT vaccination to a few other diseases including otitis media.
Note: Kalokerinos’s story is discussed further here.
The Transgender Datapoint
In Kirsch’s survey of 13,000 people, participants were given the option to select 78 different conditions (e.g., “scoliosis”), some of which Kirsch found had no association with vaccination (e.g., a 1.02X increase for COPD) and some of which Kirsch found had a strong association with vaccination (e.g., the stronger were a 10.8X increase for febrile seizures and a 7.09X increase for epilepsy—both conditions which have long been associated with vaccination). This entire series came about because Kirsch noticed a surprising result in his survey—the third largest increase was vaccinated individuals 6.9X being more likely to experience sexual orientation issues than unvaccinated individuals. This prompted him to take a closer look at that data:
From it, he found that when the data pool was restricted to those under 60, the vaccinated were 13.6X more likely to develop sexual orientation issues (which became 14.5X once more data came in), while when it was restricted to those under 24, vaccination made them 10.4X more likely to develop sexual orientation issues. This was such a high odds ratio that it proved to Kirsch vaccination had to be the primary cause of over 90% of transgenderism (for context smoking has a 15-30X odds ratio of causing lung cancer).
My response was as follows:
1. Since the option they selected was “sexual orientation/gender identity issues and/or gender dysphoria,” a gay, lesbian, or bisexual individual might check it, especially if they were not comfortable with having that sexuality, making this question less precise.
Note: if anyone has a suggestion for the best way to word this question (I couldn’t come up with one I was sure about), I will send it to Kirsch so he can incorporate it into his next survey.
2. I felt there was likely an association, but my guess was that it was more in the range of increasing the rates of gender dysphoria by 2-4X rather than 14.5X, and that there were a likely few confounding variables entering the equation, such as:
•Parents who don’t vaccinate likely are more politically opposed to encouraging transgenderism. Likewise, parents who don’t vaccinate are typically much more opposed to providing a myriad of other pharmaceutical drugs that frequently cause significant neurological and psychiatric issues (e.g., statins, puberty blockers and antidepressants).
•There has been a massive spike in gender dysphoria in the last decade but during that time the vaccination schedule (excluding the recently introduced COVID vaccines) has increased to a much smaller degree. At the same time however, it cannot be denied that much in the same way the rates of autism are inexplicably much higher than they were in the past (generally tracking the increase of vaccination), that same pattern has been seen for transgenderism. For example, according to a recent survey, 1.9% of those born between 1997 to 2004 identify as trans, for millennials 1.0% do, for those born between 1965 and 1980, 0.3% do, for those born between 1946 and 1964 0.2% do, for those born between 1928 and 1945 less 0.05 percent do.
•The social pressures creating gender dysphoria need to be taken into consideration (e.g., gender dysphoria is frequently observed to cluster in specific peer groups it rapidly spreads through).
•The effect of endocrine disruptors needs to be taken into account.
In short, I felt that while it was unlikely vaccines were the primary cause in all cases, it was possible vaccines created neurological damage which made individuals more susceptible to other factors (e.g., social pressure) which caused gender confusion.
Note: in the same way autism has two “types” (the cognitively gifted individuals who are socially awkward and the mentally disabled individuals), my friends have noticed the typical transgender individuals they interact with tend to have an above average intelligence and a high degree of perceptivity (with many being savants). One of my favorite examples of this are the Wachowskis, the two siblings responsible for creating The Matrix, V for Vendetta and a few other movies which are both considered to be masterpieces and displayed an unusual aptitude for weaving together a multidimensional plot one rarely sees in movies. Likewise, there are a variety of cultural references to these traits (e.g., the Hirja or “two-spirit people” have long been recognized for their gifts in the arts and music). This I believe in turn folds into the observation neuroatypical individuals (e.g., those with minor autism) often can deduce and recognize critical things that will never occur to their conventional peers.
Kirsch’s Second Survey
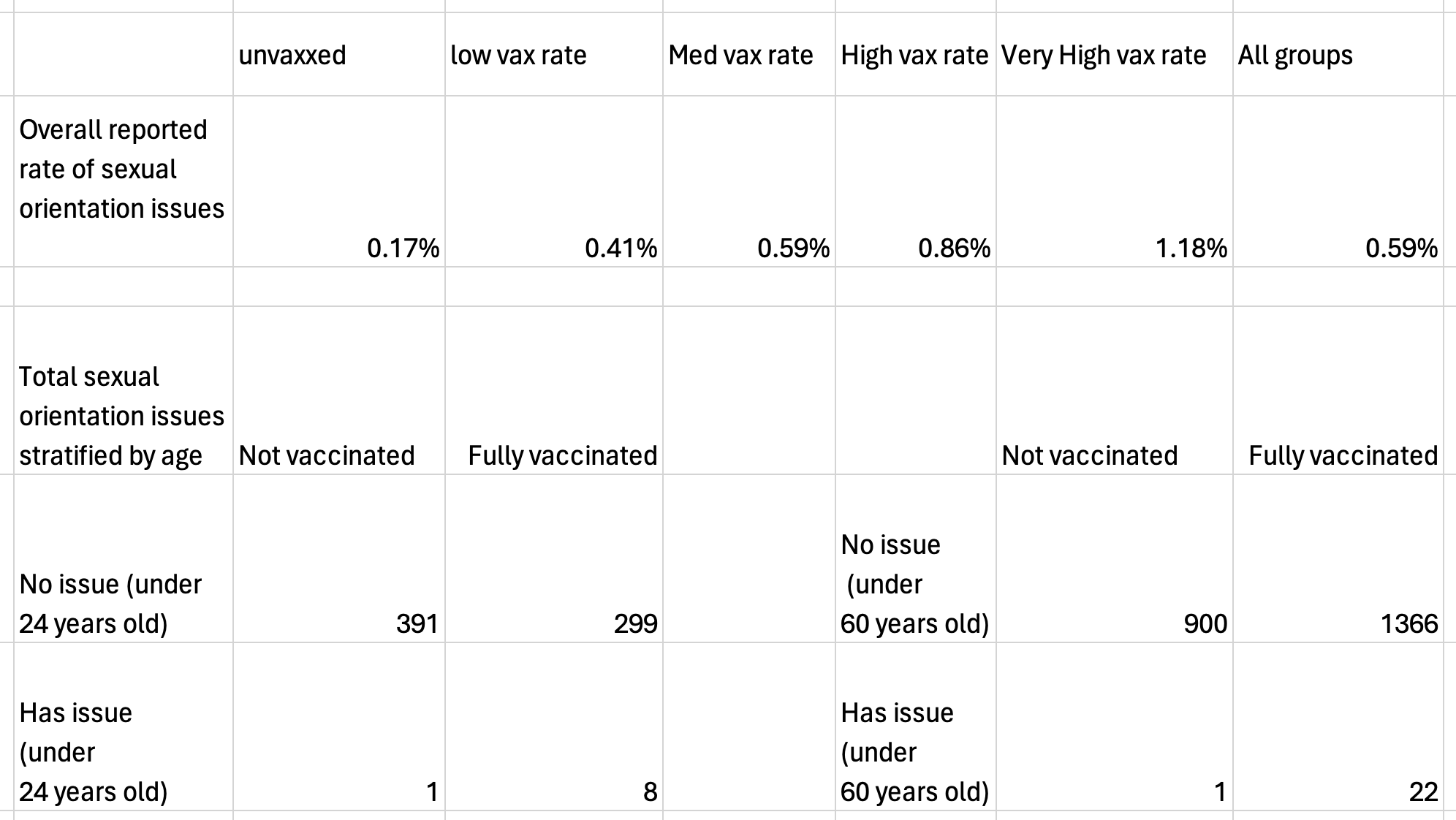
Seeing this compelling data, Steve decided to conduct a second survey specifically aimed at addressing this point. It found:
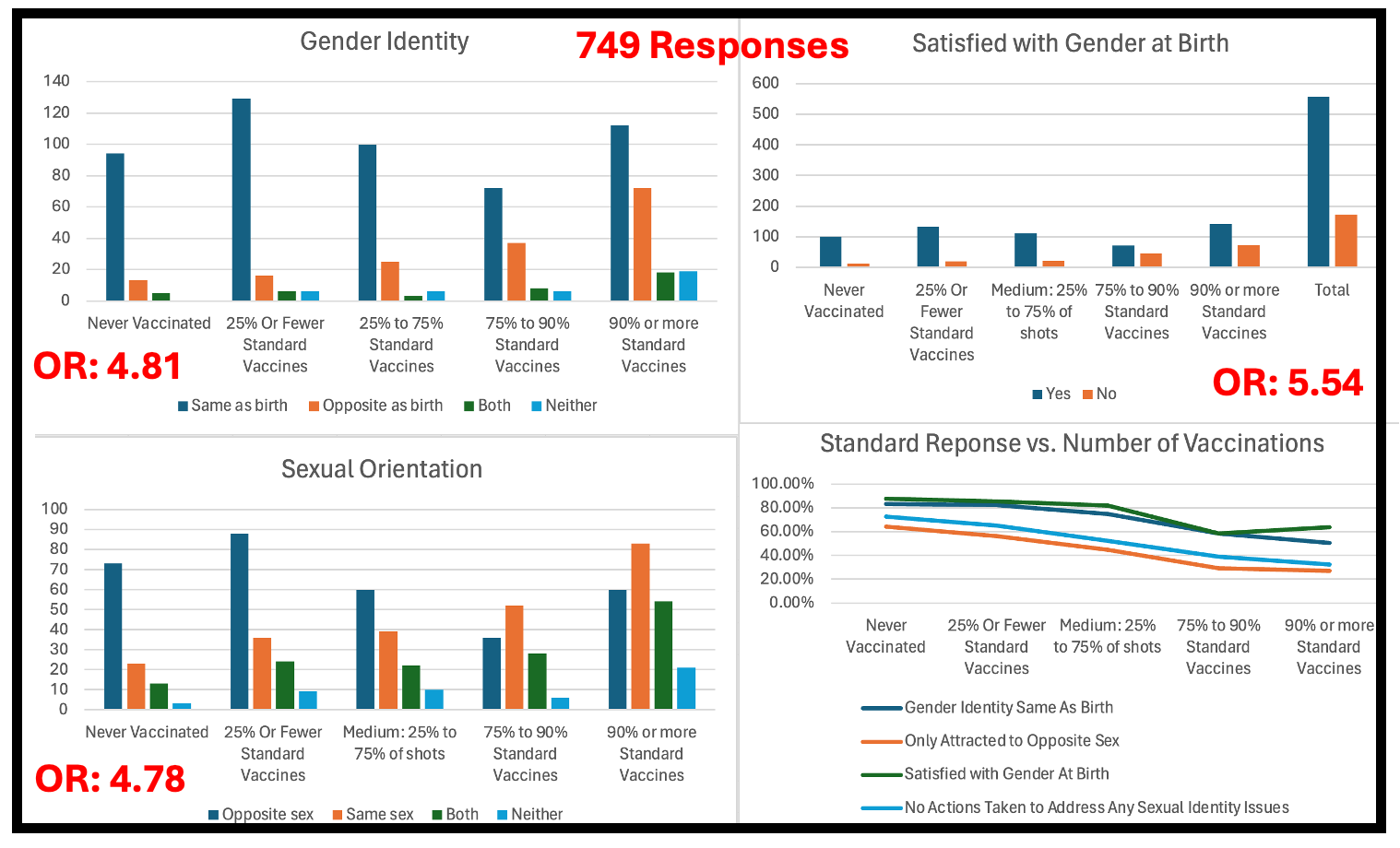
Note: a 4.81-5.54 odds ratio means approximately 80% of these events are due to vaccination.
Additionally:
•Kirsch was able to identify a pediatric practice with over 5000 patients who were unvaccinated. It had 0 cases of gender dysphoria in their patient population, whereas given that gender dysphoria occurs in at least 0.5% of the adolescent population (many other estimates are far higher) there should have been at least 25 cases in their population. That is a statistically impossible result that cannot be explained by chance, especially when you consider the expected number of cases is likely far higher than 25.
•One individual who had done extensive work to advocate for vaccine safety stated to Kirsch that they long believed the hepatitis A vaccine being added to the CDC schedule in 2004 is responsible for the surge in female gender dysphoria that began being seen 12 years after it entered the market (as prior to 2016, male to female transitions were 6-7 times as frequent as female to male ones, but now they are just as common). In turn, she argued this could be due to that vaccine being grown in male lung cells, and hence twice inserting male DNA into a developing girl at the very start of her life, which in turn causes them to manifest masculine traits at puberty.
Endocrine Disruptors
There has been a longstanding belief that endocrine disruptors (e.g., estrogen mimicking compounds such as those found in many plastics) are heavily disrupting human physiology (which is discussed in detail in this audiobook).
This for example is illustrated by the observation men for decades have been experiencing a massive decline in fertility and testosterone levels, that a variety of male health problems improve with testosterone supplementation, and that a drug which blocks estrogen signals to the brain (clomifene) can often achieve the similar benefits to testosterone supplementation. Since clomifene works by preventing the signal estrogens create in the brain that block testosterone production, this in turn suggests there is a significant effect being created by environmental estrogens.
A major effect of estrogen disrupting chemicals (EDCs) has been affecting the normal sexual development of animals. For example, Alex Jones’ famous rant of “I don’t like them putting chemicals in the water which make the friggin’ frogs gay” was a reference to a still widely used herbicide (atrazine) and it’s been observed for over 20 years that it caused frogs in the fields where it was sprayed to become hermaphrodites (i.e., they have a combination of male and female sexual organs). This in turn has led many to believe the widespread environmental contamination of endocrine disruptors may be altering sexual preferences.
One of the best reviews I’ve found on this subject was written in 2005 (which illustrates how politically incorrect it has become in recent years) to study this question. That paper essentially showed that:
There is a large body of evidence irrefutably linking animal exposure to EDCs with sexual changes in animals (including some that may affect their gender identity).
There is some evidence (but significantly less) showing EDCs affect human sexuality (as it has not received as much research).
EDCs sexually affect animals at very low concentrations (e.g., the levels we are exposed to in our environment).
The regions in the brain which affect sexuality are altered in transgendered individuals and those regions are also altered by endocrine disrupting chemicals.
A survey of 500 men who had a very strong EDC exposure (in utero exposure to DES—a now outlawed estrogen analog known for causing birth defects and cancer) found that over 150 of them “identified themselves as having any of a variety of gender-related disorders.”
The most recent study I’ve seen assessing this question was conducted from 2017-2020 in China (which has less political pressure to avoid touching this subject). After recruiting 1430 middle school children, over the course of three years, their urine was analyzed for the presence of EDCs in conjunction with a standardized score which assessed their masculine or female traits repeatedly measured and then assessed if there was a correlation between them. It essentially found there was no difference in women, but there was a significant difference in men (as shown below).
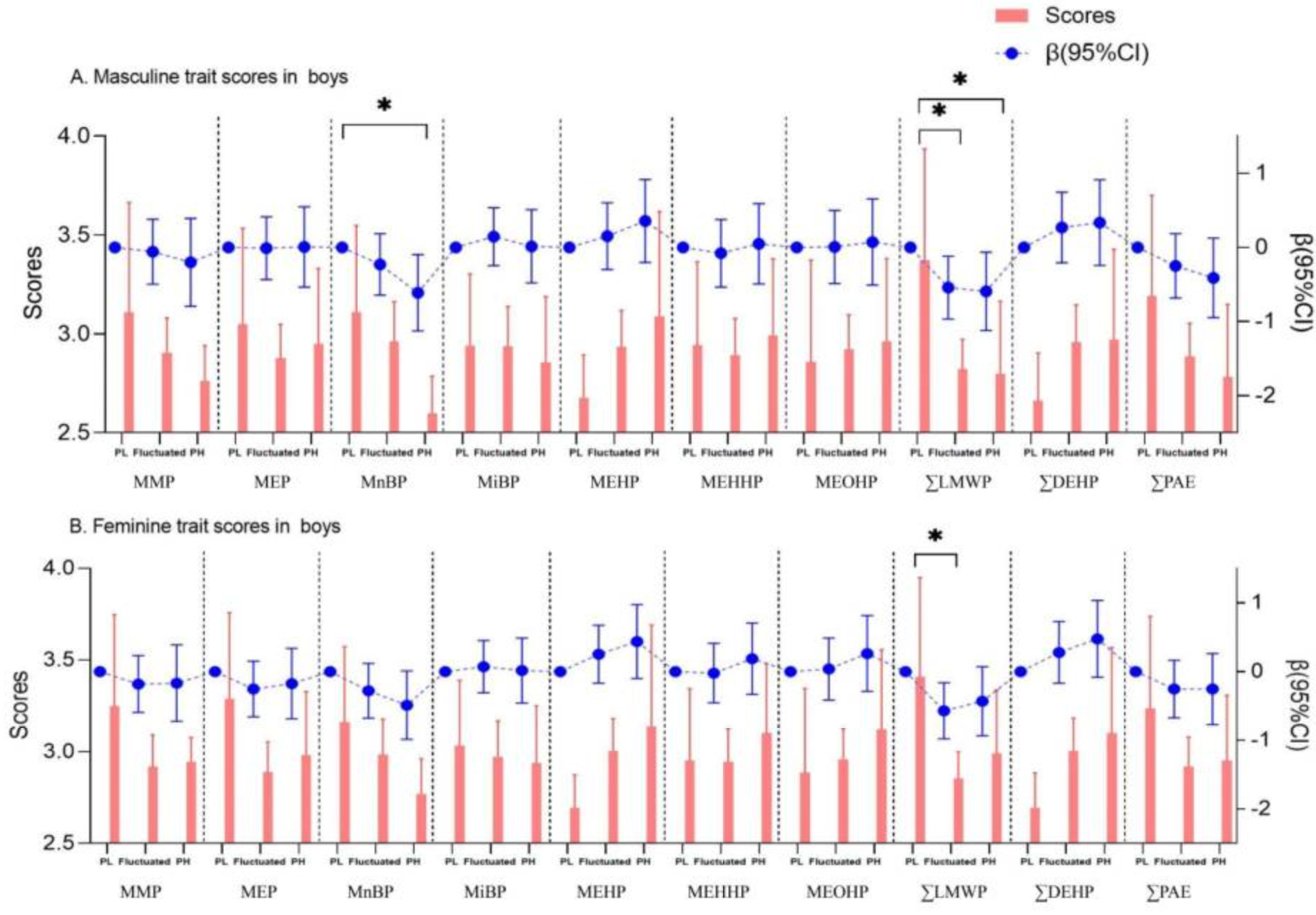
Those results are congruent with the fact most EDCs mimic estrogen, and hence are more likely to feminize men than to masculinize women. This in turn mirrors the existing statistics which show (at least until recently) that men with gender dysphoria (transwomen) are 2-4 times more common than transmen. However, these results do not account for the frequent observation that the frequency of transmen seeking out care has been continually increasing since around 1990. Likewise, they do not account for the massive difference observed in Kirsch’s survey.
Note: there is also an alternative mechanism that ties endocrine disruption to vaccine injuries. Due to their frequent tendency to cause microstrokes throughout the body, vaccination can cause a variety of overt neurological issues (e.g., many of those described in this article and the previous one). At the time the post-encephalitis cases were being observed, there were numerous instances of individuals changing their eating habits (e.g., sometimes they lost the will to eat and eventually wasted away, but more commonly they developed a morbid hunger and had rapid weight gain). Coulter in turn cited many cases from the time that supported his claim that:
Great increases in weight, leading to obesity, were noted, indicating derangement of the pituitary gland, hypothalamus, endocrine system, or other mechanism regulating weight gain. This was called "post-encephalitic obesity" or "pathological obesity.
Likewise, Coulter cited 2 cases where this happened after vaccination, one of which was ultimately attributed to a dysfunctional thyroid.
I found this very interesting because a few of my colleagues believe pituitary dysfunction (often due to poor blood flow) is the root cause of diabetes. They’ve shared cases where addressing this cured a patient's diabetes. This hence makes me wonder if pituitary issues (which are evaluated far less frequently than thyroid issues) caused by vaccination are another important facet of this picture.
Vaccination and Transgenderism
Note: there is relatively little transgenderism in the part of the Midwest I live in, so many of the inferences I am making in this article are based on extrapolating from limited observations and long discussions with perceptive colleagues who have significantly more experience with this demographic. For example, a close friend of mine had a brother who had many signs of a vaccine injury as a child, became partially autistic, and then in his teenage years became fixated on cross dressing. Conversely, no one I knew (be it a colleague or friend) knew of an unvaccinated transgendered individual.
Kirsch putting the gender dysphoria question into his survey was reflective of a longstanding suspicion many had, that vaccines cause transgenderism. As far as I know, there are three existing explanations for why the two may be linked.
1. Vaccines contain foreign DNA, and by having foreign DNA (especially from the opposite gender) contaminate your genome and partially turn you into a hybrid, it confuses the body, which may make you think are actually the opposite gender.
Note: while I have spent hours discussing this point with people who sincerely believe it, I still do not know how one could prove or disprove it, so I will abstain from discussing the hybrid theory henceforth.
2. Vaccines cause autism, and autism causes transgenderism, so it is fair to argue vaccination causes transgenderism.
3. Transgenderism is another complication of encephalitis.
Note: the final point is by far the least frequently mentioned point (e.g., I only looked for evidence to support this because I suspected it might be the case and in doing so, I had to look quite far to find any research on the subject).
The second point builds on a longstanding observation that autistic children are dramatically more likely to be “gender-diverse” (e.g., transgender). To illustrate:
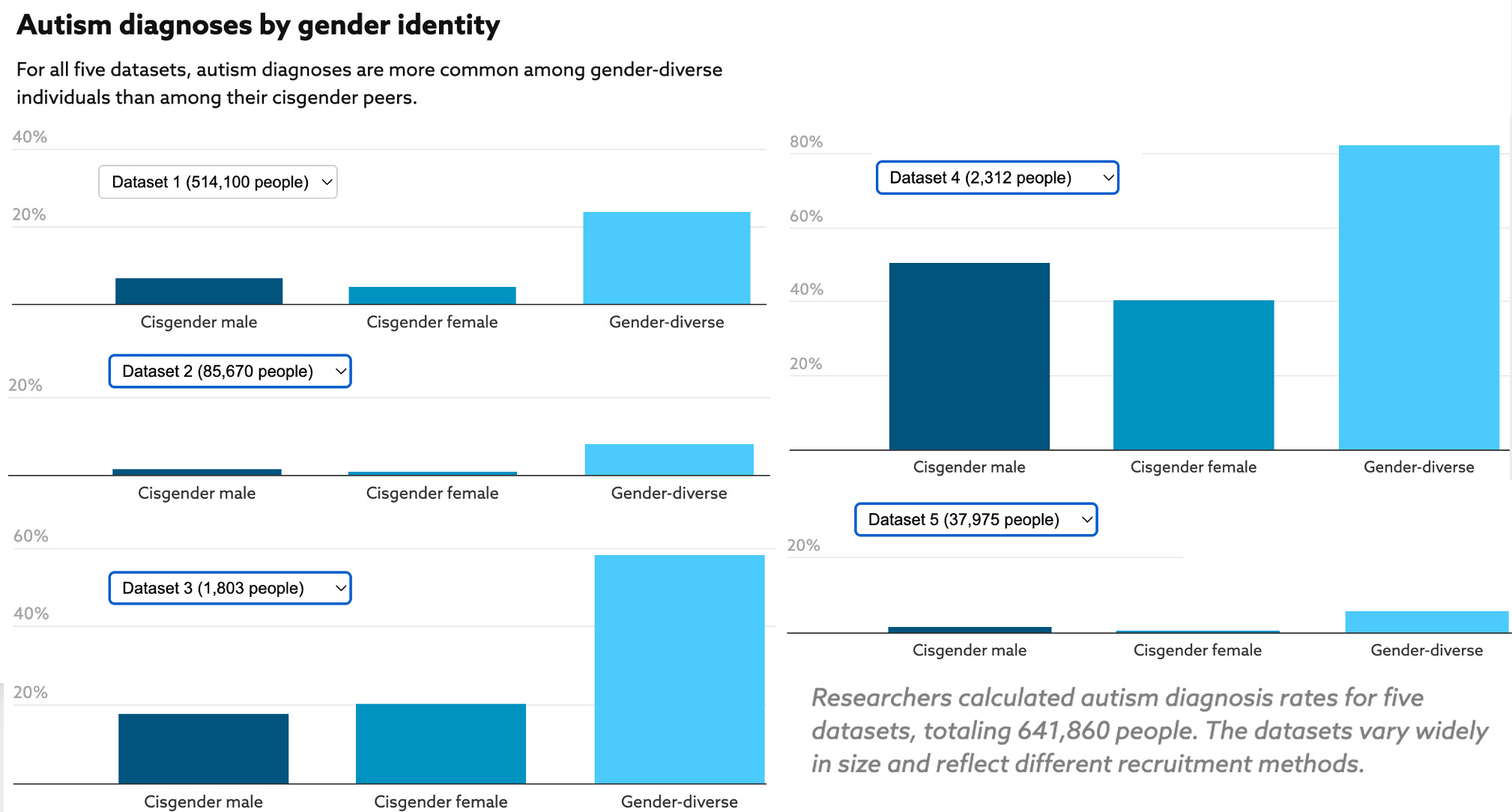
Conversely, transgender individuals are also much more likely to be autistic (e.g., the existing studies have found it occurs at a rate of between 6 – 26% compared to a 1.85% rate in the general population). Additionally, most of the existing studies have found that a higher proportion of female autistics are “gender-diverse” than male autistics (at approximately a 2:1 ratio), whereas men are more likely than women to become autistic (occurring at approximately a 4:1 ratio).
Presently, the correlation between autism and transgenderism is well-recognized (e.g., all my friends who frequently interact with transgender individuals either medically or professionally agreed the high prevalence of autism within the demographic is unmistakable). However, despite this being recognized, it’s much less agreed upon why this happens (which I suspect is in part due to this entire subject being a political minefield and no one wanting to risk their careers by publicly endorsing an “insensitive” position). Some of the most commonly publicly cited reasons include:
•Autistic individuals are more resistant to social conditioning, so they are more likely to recognize and embrace their gender dysphoria (whereas members of the general population are more likely to suppress it).
•Autistic individuals have a tendency to get fixated on something, so if they are introduced to concepts from the opposite gender, a fixation can build which eventually results in them wanting to embrace the opposite gender identity.
•The rigid thinking observed within autism could cause misinterpretation of (typically) passing interests they have which are not typical for their gender.
•The intolerance to change frequently observed in autism could cause them to reject changes in their body associated with puberty (e.g., menstruation or having an erect penis)
•Autistic individuals often are hypersensitive to external stimuli, which I believe is in part due to nerves or brain structures that typically dampen external signals being damaged (frequently as a result of the pervasive microstrokes they cause throughout the body). This hypersensitivity, in turn, causes them to perceive or prefer things which result in them adopting a habit of the opposite gender (e.g., choosing clothes of the opposite gender because they are more comfortable).
While I think some of the above may play a role and could create some increase in the rates of gender dysphoria and transgenderism in autistic individuals, I believe it’s really pushing it to say they can account for the 7 to 14-fold increase which is seen in Kirsch’s data. This, I in turn would argue is because no one wants to publicly discuss the other potential links. For example:
•Autistic children are particularly vulnerable to abuse—we’ve seen some pretty sad cases in the ER and my friends who care for autistic children believe this being swept under the rug is the biggest problem with how society addresses autism. Existing data shows autistic children (and intellectually disabled children) are roughly 3-4 times more likely to be bullied, 2-3 times more likely to experience physical or sexual abuse, and 2.4 times more likely to experience abuse they were referred to childhood protective services (but 50% less likely to have CPS investigate what was going on). As a result, autistic children are 8-10 times as likely as their peers to have PTSD..
Transgender individuals likewise experience high rates of childhood abuse (1.8X for physical abuse and 2.0X for sexual abuse), and have high rates of the conditions associated with sexual abuse (e.g., they are 10 times as likely as their peers to have PTSD). As many transgender individuals are sexually assaulted before they realize they identify with the opposite gender, this has led many to suspect that the abuse could have triggered the gender dysphoria (while others deny the link and consider it highly offensive to suggest it).
•Many groups will try to promote their ideology by reaching out to unhappy people and telling them their ideology is the solution to everything that is wrong in their lives (regardless of whether it is). Because of this, many younger people receive the message all the unease and discomfort they are experiencing (much of which is neurologic damage from pharmaceuticals) is in fact due to an unrecognized gender dysphoria and will all get better once they transition. Yet, once converted, if they get worse (which frequently happens) and decide to transition, that same community that lovingly embraced them will reject and attack them—something not all that different from how liberals who developed COVID vaccine injuries were attacked by their peer groups just as harshly as the gay men who came out of the closet in the 1980s.
Note: one of my female friends who had a difficult anxiety ridden adolescence remarked that if she had been alive now, she likely would have been convinced to undergo a gender transition she could never take back.
Encephalitis and Gender Identity
One of the points Harris Coulter repeatedly emphasized in his book which attempted to lay out the profound consequences of large numbers of people developing vaccination encephalitis was that the brain damage it created was responsible for the changes in sexuality being seen in America:
The unintegrated sexuality of the minimally brain damaged [MBD] can also take the form of "gender identity disorders," meaning confused sexual identity, homosexuality, and bisexuality.
Of course, the sexual revolution of the past three decades has seen the emergence of homosexuality as a major social and political influence in American life.
I hence wanted to see the references he used to make that claim. Unfortunately, he only published half of the references he used to write the book—so I was essentially left to trust Coulter on the basis of the fact he was otherwise quite meticulous in exactly what he claimed (but conversely could have been fairly biased on this issue).
Nonetheless, he did provide some evidence to support his case. It was as follows:
•He emphasized that those with MBD or who had recovered from encephalitis were widely recognized to become hypersexual. Modern research in turn now recognizes that hypersexuality is significantly elevated in LGBTQ individuals.
Note: the second most common type of dementia, vascular dementia (another condition where the blood supply to the brain is interrupted) is also characterized by triggering hypersexuality.
•The individuals also often have difficulty making sense of themselves or their environment (e.g., beyond the points mentioned earlier in this article, in the previous one, I discussed how they often were observed to have difficulty telling left from right or up from down).
•The classic 1931 treatise on post-encephalitic syndrome discussed this issue:
Confused sexuality, bisexualism, and homosexualism are further features of the post-encephalitic syndrome. Von Economo noted that post-encephalitics "indulge in sexual misbehavior of every kind and make themselves willing partners to such. . . Sexual delinquencies... remain the common practice of these patients." In general, their attitude toward sexual matters is impulsive and superficial, their sex life "impersonal, trivial, and poorly integrated.”
Coulter also cited one of Von Economo’s cases where this happened:
N.N., age twenty years, male... At the age of four, in January 1918, he suffered with acute (epidemic) encephalitis leaving no immediate sequelae. Behavior difficulties became apparent a few years later. He constantly stole from other people, ran away from school, was sexually delinquent, stopped strangers on the street and asked them for money. . . . He admitted performance of perverse sexual acts in another hospital.... He showed aggressive, impulsive tendencies, was emotionally over- reactive, unstable, irritable, and unpredictable. Occasional homosexual trends were noted early in the course of his admission. . . conduct continues to be abnormal and he has a strong homosexual trend. He will prowl through the wards at night for the purpose of [having sex with men] and requires very careful and continued supervision, both day and night. At times, he will try to assault the weaker patients who resent his advances.
Note: I was unable to get a copy of the original 1931 text, and hence had to assume Coulter’s synopsis of it was accurate.
•Coulter accurately cited an authoritative article on temporal lobe epilepsy (one of the seizure disorders associated with encephalitis) which contains the following:
Table 1. Commonly cited interictal behavioral manifestations of temporal lobe epilepsy.
Sexual Dysfunction: Global hyposexuality, sexual hypoactivity, altered affinity and interests.
Clinical evidence firmly asserts that global hyposexuality is prevalent among patients with TLE, symptomatically presented as cyclic impotence and frigidity, weakened libidinous interests, and sexual hypoactivity. In some cases, the cathexis for a love object may deviate to bisexuality, transvestism, or fetishism. Erotic fantasies and dreams may be eroded, and there is a persistent, less than ardent desire for sexual engagements.
I then looked through the modern literature to see if I could find anything similar to what Coulter had described and found this remarkable 2022 case report:
Limbic encephalitis (LE), a rare cause of encephalitis, generally presents with neuropsychiatric manifestations, memory deficits, seizures, and movement disorders. The case of a 41-year-old female patient with LE involving the left amygdala is presented. The patient was admitted to the emergency department with complaints of unconsciousness and seizures. Paraneoplastic and limbic markers were negative. This case was diagnosed as seronegative LE. Three to four months after the diagnosis, it was observed that her sexual preference changed to the female sex. No report has been published so far, concerning any case of LE associated with changes in sexual behaviour. The patient was treated with intravenous methylprednisolone (IVP) and triple antiepileptic therapy. After treatment, changes in sexual behaviour returned to the previous state.

Note: the only other thing I’ve come across which can cause a rapid change in sexual preferences like this are heart transplants where the recipient takes on the sexual preferences of the donor (numerous documented cases of that happening are listed in this article).
However, as I did not feel Coulter provided enough evidence to establish the link, I then looked at this from the other direction—do transgender individuals have higher rates of the disorders commonly associated with MBD?
Unfortunately, this has been surprisingly understudied in the scientific literature, as almost all the literature on conditions associated with gender dysphoria tends to focus on associated psychiatric conditions such as depression, anxiety, suicide and post-traumatic stress disorder, likely since it can be argued the suffering one experiences from these conditions justifies transitioning them to their true gender identity.
However, while surprisingly little research exists on the other conditions (besides that previously mentioned for autism), I did find two pertinent articles. The first was a small study:
Ninety percent of the cases with gender dysphoria had at least one psychiatric diagnosis. Attention-deficit/hyperactivity disorder (ADHD) (75%) was the leading comorbidity, followed by major depressive disorder (25%).
The other psychiatric comorbidities are oppositional defiant disorder (ODD): 10%; social phobia: 5%; specific phobia: 5%; general anxiety disorder: 5%; separation anxiety disorder: 10%; enuresis: 25%; encopresis: 5% and substance abuse: 5%.
Along with a systematic review:
All of these studies found elevated left-handedness among those with GD, including both transmen and transwomen. In alphabetical order, Green and Young (2001) found that transmen exhibit elevated levels of non-right-handedness, Watson and Coren (1992) found that 35% of male-to-female transgender persons were left-handed, as compared with 11.6% in a control sample, and Zucker et al. (2001) found that 19.5% of boys with GD were left-handed compared with 11% among controls but did not find a significant difference for girls.
I considered this finding noteworthy as ADHD was the condition by far the most commonly associated with MBD (to the point that the two terms were used interchangeably at one period), and likewise no longer being right handed was frequently associated with MBD (and something I have personally witnessed occur after vaccine injuries). Additionally, three of the more unusual conditions listed (oppositional defiant disorder, enuresis, and encopresis) were also conditions characteristically associated with MBD.
Note: I suspect detailed research on left-handedness exists because it’s not a “stigmatizing condition” whereas almost every other one is, and hence people are reluctant to research it.
Since the data I was looking for did not exist online, I decided to try and find it from Kirsch’s data and see what patterns emerged. After searching the sheet for “sexual orientation,” I found 62 entries, of which one was not actually reporting the issue and 3 of which reported it in the absence of vaccination. Of those 3, one discussed a history of sexual abuse by her pediatrician which made the individual become a celibate, a younger woman discussed a variety of disorders including PANDAS (which I believe can cause encephalitis) along with receiving a newborn vitamin K shot (which can sometimes cause issues), and the final one (an older man) stated his only other condition was arthritis.
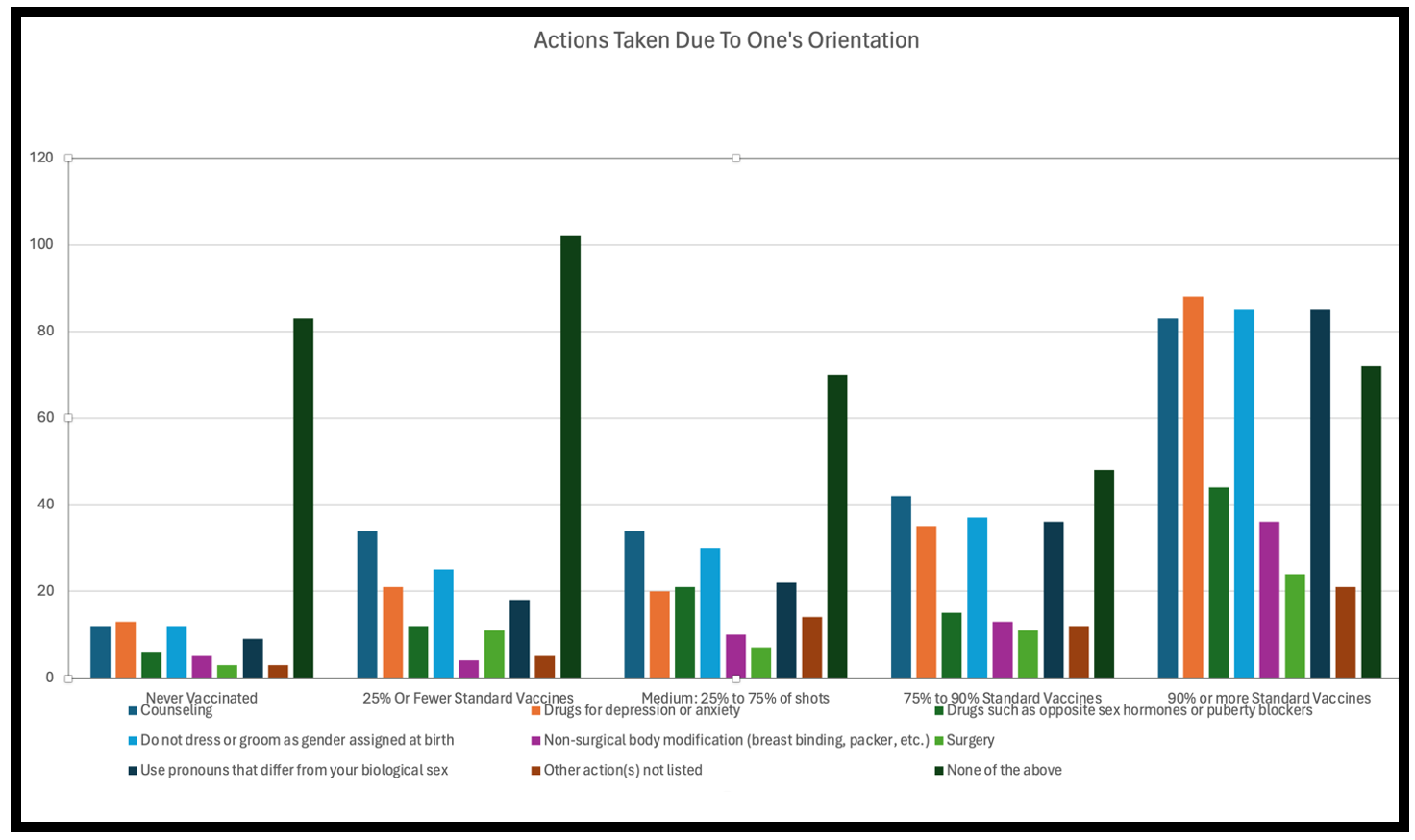
With the remaining 56 entries, 21 characterized their lifetime vaccine use as “very high,” 12 as “high,” 11 as “medium,” 12 as “low.” 43 were from the United States and with each state represented roughly proportionally to its population. 27 were women, 28 were men, 1 had an unspecified gender, and the ages ranged from averaging 37.9 for everyone, 31.1 for women (the youngest of whom was 15) and 45.1 for men (the youngest of whom was 18). 35 were from parents describing their child, 19 were self reports, 35 were for a child, 1 was for a spouse, and 1 was an unspecified relationship.
Most of the respondents suffered from a variety of other chronic illnesses (almost all of which are ones classically leaked vaccine injuries—hence why Steve included them in his survey). Once I excluded the conditions that weren’t appropriate to include (e.g., Down’s Syndrome or a COVID vaccine injury), the total number ranged from 0-12 for the respondents and averaged 4.5 in total. Those illnesses (listed by what number and percent of respondents had them) were as follows:
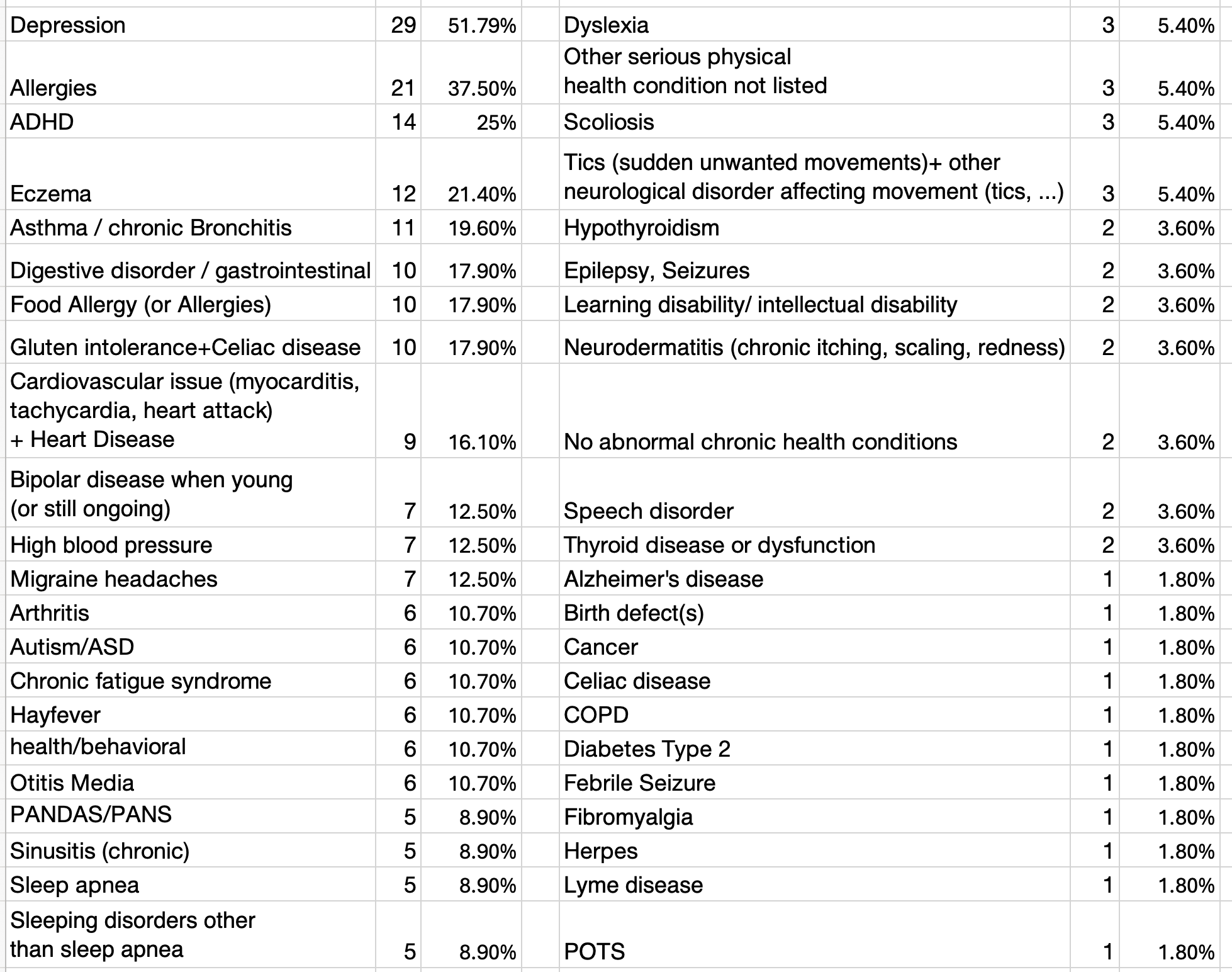
As the top findings match two of the things most commonly associated with MBD (ADHD and food allergies) this supports the argument gender dysphoria is linked to them. At the same time, however the developmental disabilities commonly seen with MBD were fairly rare in this list and the clustering I saw was not of the magnitude I had expected to observe. Assuming gender dysphoria is indeed correlated with vaccine brain damage (which it might not be), I could see two explanations for this discrepancy:
•Kirsch’s survey did not ask about many of the subtle neurological issues associated with MBD (as it’s a relatively unknown subject—even within the vaccine safety movement).
•”Sexual orientation issues” are a more subtle (less overt) manifestation of MBD, so they aren’t necessarily correlated with the issues observed in more severe brain injuries.
Note: the thing that would have really helped settle this was a clearer understanding of exactly what changes occur in transgendered brains and what changes occurred in vaccine encephalitis. The challenge I ran into was this being fairly specialized knowledge that lay outside my knowledge base (as I am not a neuroradiologist or a pathologist) and that in the past (when vaccine encephalitis brain autopsies were frequently done and reported—something which never happens now), MRIs did not exist (which are typically what is used to evaluate transgender brain differences), so all the histology reports I’ve read were quite difficult to mentally translate into what was being described in the transgender MRI imaging.
Lastly, if you look at the symptoms list, you will notice that 5.4% had a movement disorder like tics (i.e., Tourette’s syndrome). This builds upon a longstanding association between gender dysphoria and Tourette’s syndrome (a condition many have linked to vaccination) which recently came to prominence after at least 294 children developed the condition during the pandemic after seeing others talk about it on TikTok (those videos received almost 10 billion views). Since 87% of the children who were afflicted were girls and had many of the conditions associations with gender dysphoria (e.g., two-thirds had an anxiety diagnosis, one-quarter had depression and one-quarter had ADD or autism), along with 12%-43% (depending on the sample) being transgender or nonbinary, this led many to suspect the same underlying social contagion which gave rise to the tic disorders was also creating the clusters of gender dysphoria frequently being seen now.
Likewise, there is an infamous 1996 case report of an adult male patient with a borderline learning disability who presented with cross-dressing and a strong wish to undergo a sex change that disappeared immediately after he started the medication typically used to treat Tourette’s syndrome but then returned a year later immediately after the medication’s dose was halved. As pimozide is also used to treat a variety of delusions or hallucinations, a psychiatrist suspected this case represented a true case of autogynephilia (which is not the typical cause of gender dysphoria), something they sometimes see in patients with severe schizophrenia and declining cognitive function (as these patients will have delusions about their genitalia).
Note: a reader recently sent me a compelling study which effectively showed that mast cell activation (a common side effect of vaccination) would cause female rats to develop male sexual behaviors, while mast cell suppression would cause male rats to become feminine and lose their sex drive. Given that women appear to be more likely to develop mast cell activation from vaccination, that study potentially supports this thesis.
Sensitivity vs. Specificity
In a recent article about my views on governance and politics, I shared my perspective that many of the challenges people face ultimately come down to trying to find an acceptable balance between two conflicting positions on a public policy—something not all that different from the need for any therapy people take to have an acceptable balance between risk and reward.
Note: for decades, there has been a longstanding embargo on allowing vaccine skeptics to publicly debate vaccination (as each time it happened the “expert” was humiliated and the public further lost their desire to vaccinate). Peter McCullough recently was allowed to debate the vaccine on a podcast, and did a masterful job refuting the pro-vaccine host by showing the risks of the COVID vaccines clearly outweighed their benefits [which has since gone viral on the internet].
Often this balance is a question of how consistently you can accomplish your stated goal (e.g., removing a violent offender from society by sending them to prison) vs. how often you overshoot your target (e.g., imprisoning an innocent person), and in medicine, this concept most frequently comes up with screening tests (e.g., you want to catch a dangerous cancer early on, but simultaneously, you don’t want someone to suffer going through the whole process when what was there would have never caused any issues in the first place).
This balance between sensitivity (consistently getting your target) and specificity (not overshooting your target and creating collateral damage) is often a very difficult balance to strike because each is in opposition to the other. Because of this, many of the institutions within society essentially are the compromise that has been reached after years of debate and political activism between the side that wants sensitivity to be prioritized and the side that wants specificity to be prioritized.
In the case of transgendered medicine, this same question again shows up. On one hand, there are many transgendered individuals who go through an immense degree of suffering and distress from being in the wrong body, and an even greater degree of distress from their circumstances being marginalized or attacked by society rather than receiving the support they need. On the opposite end, there are many individuals who come to believe they are transgendered (when they are not), and by the time they realize they aren’t, nothing can be done because they already have permanent alterations from the gender transition.
Typically, when this question is debated, it ignores the situation of the other side (e.g., many of those opposed to transgendered medicine are largely oblivious to the extremely challenging lived experiences of many transgendered individuals or the fact some people who transition have a very positive experience from it, while many in support of it deny or attack the existence of the countless individuals who have de-transitioned). While unfortunate, this is typically what one witnesses in highly contentious political debates.
Predatory Business Practices
Frequently to address poor sensitivity or specificity, politicians will enact laws to increase one or the other (e.g., recently 19 Republican states enacted laws restricting gender-affirming care, something which in essence was aimed at improving specificity). In many cases, these approaches end up overshooting their target.
For example, Obama’s 2010 healthcare law contained a provision that prohibited health facilities, programs, and activities receiving federal funding from denying insurance coverage or care on the basis of gender identity and expression. This provision in turn supported those who had previously run into those denials but simultaneously also created a massive industry overnight because it was now illegal to refuse to pay for the fairly expensive services frequently offered to transgendered individuals.
Note: the finances of this industry were discussed in this recent interview.
In turn, I would argue that while “good enough” balances between sensitivity and specificity can be found, once money (and thus corruption) enters the equation, the balance is rapidly lost (e.g., consider how the corrupt FDA approved the COVID vaccines and then kept them on the market despite a tsunami of evidence showing they were not effective and extremely dangerous).
Note: I’ve also noticed how often a societal message will be chosen which allows one bad actor to be excused for their conduct while another profits from a “solution to it.” To illustrate—many infectious disease outbreaks are ultimately due to toxic chemicals being put into the environment by industry, but the narrative we always hear is how dangerous the disease is and how important it is to find a vaccine for it (e.g., ten years ago this happened with the Zika outbreak in Brazil as everyone ignored the contribution of the mosquito pesticide which had recently been sprayed in the area).
The pharmaceutical industry is one of the worst actors in this area as it both sells the “treatments” to a myriad of diseases other industries are creating, and simultaneously sells the treatments to the conditions it creates (which amongst other things has led many to argue the actual business model behind vaccines is selling drugs for all the other chronic issues they create).
I personally believe this issue is particularly egregious in the field of mental health, as psychiatric medications are given out indiscriminately for the side effects of many other pharmaceuticals (e.g., birth control pills and vaccines) create which then create a whole host of other even more severe psychiatric issues.
In a recent article I discussed the story of Lupron which concisely illustrates this dynamic. Briefly:
•Lupron works by (to varying degrees) permanently disabling the body’s ability to make sex hormones. Since hormones are essential for life, this frequently causes the risks of the drug to greatly outweigh its benefits.
•Since it had such a bad risk to reward ratio, its initial approval was as an alternative to the now banned estrogen analog (DES) as a palliative treatment for advanced (likely fatal) prostate cancer. Not surprisingly, no one wanted to touch it.
•To solve this problem, Lupron was priced so that doctors made thousands of dollars each time they gave it to someone, and before long, it was widely used (e.g., for fairly minor prostate cancers) and frequently accounted for half of a urologist’s revenue, with 53% who did not believe it benefited their patients admitting they still used.
•To further increase sales, a variety of other uses were concocted for it (e.g., stopping children’s puberty, making children taller, harvesting eggs, or treating a variety of female issues such as painful and excessive menstrual bleeding).
•Due to its inherent toxicity, Lupron (and the related GnRH agonists) has one of the highest rates of severe complications of any drug on the market, and as a result, a lot of people (particularly) have had their lives permanently ruined by the drug—including adults who took it as children for precocious puberty. However, because so much money is made off selling it, the industry has successfully buried almost every lawsuit and the harms of Lupron are still relatively unknown.
Within transgender medicine, one of the current pushes is to give a GnRH agonist (e.g., Lupron) to children who are considering a gender transition since it is a “safe and reversible” way for them to initiate the process while they are trying to make their minds up and might prevent them from developing sexual traits that could interfere with their ability to have a cosmetically satisfying gender transition later.
Given my previous familiarity with Lupron, I immediately interpreted this as the current approach being developed to unscrupulously market the drug, and after I read through all the current guidelines used in transgender medicine discovered that:
•They liberally recommended giving puberty blockers in a wide range of circumstances and continually emphasized their effects were temporary and reversible (which is not true)
•While the dangers of hormone supplementation (which is far less profitable) were mentioned, the dangers of the GnRHa’s never were. As a result, the widespread physical and emotional damage these drugs are doing to the transgender population is still relatively unrecognized.
Note: additionally, leaked correspondences also showed the people making these guidelines had no idea what they were doing or what the long-term consequences of giving the puberty blockers are, and that they were intentionally choosing to greatly prioritize sensitivity over specificity in their recommendations for them.
As the Lupron example shows, I feel the money involved has caused this industry to prioritize sensitivity (making sure every child who needs gender-affirming care receives it) over specificity (making sure children who aren’t actually transgender don’t get it and making sure the medical approaches utilized don’t have harms which greatly exceed their benefits).
Note: in a recent article on the secrets behind healthy clothing, I discussed the long history of women being pressured by society to wear extremely unhealthy clothing (or footwear) so they could conform to the society’s current standard of beauty (e.g., I discussed how bras are a very new invention and have a variety issues such as being strongly linked to breast cancer). A strong case can be made that the current push to suppress the natural features of one’s body arising from their biological sex is the current manifestation of that trend.
The current mismatch between sensitivity and specificity in this field was illustrated by a recent (brief) segment of Dr. Phil with a whistleblower from a gender-affirming care clinic in St. Louis where she witnessed groups of children rapidly being approved for gender-affirming care and then regretting the choice (e.g., she had numerous children call in begging for their body parts be put back on). Yet, when she pointed out these issues, she was silenced by her supervisors (who likewise refused to stop giving puberty blockers after parents demanded to stop them because of their devastating side effects)
Note: in the past, parents who could not accept their child being gay would often send them to “therapy” to cure it. These programs were often highly abusive, ineffective and traumatic, so many liberal states moved the pendulum in the other direction by outlawing conversion therapy. However, arguably, the pendulum swung too far in the other direction as those laws also made it illegal for therapists to not affirm a child’s gender dysphoria by providing an alternative explanation for it (e.g., unresolved trauma from childhood sexual abuse), which in turn has led to numerous anonymous therapists stating they are mortified by the fact they are signing off on children they sincerely do not believe should be going through the gender transition process. Ironically, many LGB activists (who are organizing into an every growing group) consider the push gender-affirming care in minors to be the new conversion therapy, as many of those children would have likely just become homosexual or bisexual had they not been transitioned and suspect the push is in part due to the fact LGBT equality has largely been earned in the country, so the existing LGBT advocacy groups need a new justification for fundraising.
In the same way that therapists often can’t do what they feel is in their patient’s best interests, I’ve also heard similar accounts from physicians. For example, a colleague spent some time at a few of the premier gender-affirming clinics on the East Coast. She shared with me that with the older endocrinologists she observed, some were unscrupulous individuals who were profiting off of selling expensive drugs (e.g., Lupron) to patients who were clearly being harmed by it, while others were aware what was happening wasn’t right, but were unable to do anything as younger activist doctors training with them to become endocrinologists would aggressively pressure everyone to transition the children who came in (e.g., a developmentally delayed girl who had no opinions either way on her gender).
Note: I have long suspect that the pharmaceutical industry is funding the current push for gender affirming care as many of the things I’ve observed (e.g., the sudden massive media coverage of anything which advances this message that is very similar in style to the PR messaging pharma uses to promote its interests or the fact a lot of people will spend a lot of time on the internet trying to convince unhappy children they are actually transgender) suggest someone is paying a lot of money to fund this. Likewise, one “expert” in this area, Toby Rogers (who has done a lot of LGBT activism) reached the exact same conclusion as me (discussed further here in his excellent article). I’ve tried to find a financial link between the pharmaceutical companies and this push, but thus far I have not. However, it has been possible to link a group of activist billionaires to it (which is discussed further in this thread).
The Pendulum Swings Back
In the previous article about natural and unnatural political systems, I shared my perspective that if you force an unnatural situation to occur, it is often quite damaging and will inevitably create strain which will require more and more force to prevent it from snapping back. Unfortunately, since humans always want to control things (and foolishly believe that they can), this mistake has been repeated again and again throughout human history (e.g., in the previous article I gave the argument that modern medicine revolves around dominating the body and hence creating unnatural strains throughout it).
Note: for this reason, as much as possible, I’ve tried to live my personal and professional life by seeking out situations which flow naturally and do not entail large amounts of strain being created (e.g., I primarily write here because it felt as though the universe gave me the opportunity to and a variety of things somehow “went right” which allowed me to become far more widely read than I ever imagined would be possible). This methodology has been very helpful in my life, as while I often can’t chart exactly where I will end up ahead of time, I am ultimately able to get far more done than if I had tried to rigidly control my path from the start.
Normally, “nature” keeps things in an equilibrium where both sides hold each other in a state of balance. However, when an ideologically focused group assumes too much power or too much money is at stake in the issue, we will frequently see them rapidly shift things to that unnatural state full of strain. For example, because of the climate that was created during the pandemic, it made it possible to push forward a variety of policies and vaccines that were harmful, nonsensical and highly ineffective. This in turn has created an unprecedented situation—they were so over the top policies that it woke many people up to the dangers of the pharmaceutical industry and we are now seeing a historically unprecedented increase in the number of parents rejecting vaccines entirely.
In the case of gender-affirming care, the degree to which its advocacy and increased sensitivity has been promoted has led to poor specificity and cultural strain being created which is creating a significant backlash against it. For instance, as mentioned before, Republican states are now banning the practice and many providers are now getting sued—which is causing the medical malpractice rates for it to skyrocket, which is making many doctors no longer able to afford to continue doing it. In turn, I feel that this swing will likely develop its own momentum, and eventually create a situation which is the opposite of what its activists wished for when the push began during Obama’s presidency
Most recently, a comprehensive report (which was 4 years in the making) was released which has already radically shifted how transgender medicine is being approached by England’s national health service (it paused the practice). Briefly, this report found that:
There is no simple explanation for the increase in the numbers of predominantly young people and young adults who have a trans or gender diverse identity, but there is broad agreement that it is a result of a complex interplay between biological, psychological and social factors. This balance of factors will be different in each individual.
An appraisal of international guidelines for the care and treatment of children and young people with gender incongruence found that that no single guideline could be applied in its entirety to the NHS in England.
There are conflicting views about the clinical approach, with expectations of care at times being far from usual clinical practice. This has made some clinicians fearful of working with gender-questioning young people.
While a considerable amount of research has been published in this field, systematic evidence reviews demonstrated the poor quality of the published studies.
The strengths and weaknesses of the evidence base on the care of children and young people are often misrepresented and overstated, both in scientific publications and social debate.
The controversy surrounding the use of medical treatments has taken the focus away from what the individualized care and treatment is intended to achieve for individuals seeking support from NHS gender services.
The rationale for early puberty suppression remains unclear, with weak evidence regarding the impact on gender dysphoria, mental or psychosocial health. The effect on cognitive and psychosexual development remains unknown.
Clinicians are unable to determine with any certainty which children and young people will go on to have an enduring trans identity.
For most young people, a medical pathway will not be the best way to manage their gender-related distress. For those young people for whom a medical pathway is clinically indicated, it is not enough to provide this without also addressing wider mental health and/or psychosocially challenging problems.
Conclusion
I have long believed the ruling class controls society by erecting pyramidal hierarchies everyone is forced to follow (e.g., you can only trust news from “credible journalists” in the mass media) and the buying out the top of the hierarchy so that for a relatively small cost, most of the society can be controlled.
A curious situation hence exists within the medical literature; prior to the days of the major academic publishers monopolizing the industry (many of whom are now tied to the WEF), physicians around the world regularly published a large amount of compelling data on controversial medical subjects—something we almost never see now.
Because of this, I frequently find that to get the answers I am looking for to our present dilemmas, I have to search far into the past—which is a fairly sad statement for the state of science today.
Much of this in turn has arisen from the belief the pharmaceutical industry has managed to impose upon society: scientific papers should be taken at face value and their raw data should never be available for outside scrutiny—which as you might expect, continually lends itself to fraudulent publications (something for example many are gradually coming to realize characterized the clinical trials for the COVID vaccines).
Fortunately, information wants to be free, and regardless of the efforts the ruling elite used to protect the vaccine cartel (e.g., in 1997 Clinton allowed the pharmaceutical industry to buy out the mainstream media—at which point the news stopped covering them), they are always temporary and fail.
Most recently, the pharmaceutical industry recognized a free and open internet was one of the largest threats to their business model as it allowed the truth to be rapidly disseminated and it was nearly impossible to constrain it. Nonetheless, they truly tried, especially after 2016, and as a result, the industry was able to inflict numerous medical atrocities upon the world (e.g., the lockdowns, the suppression of effective COVID-19 treatments and mandating vaccines that were not fit for human consumption).
However, like each party who tried to enforce their unnatural will upon the world, these measures were temporary and created a strain that has moved things in the opposite direction.
At this point, the public has lost a significant amount of trust in the academic press, as many can now see something being published in a peer-reviewed journal does not mean it should be reflexively trusted, but rather that it conforms to the existing narratives and interests of the peer-reviewers. In turn, a window has now been created for independent research and science to be done which bypasses the chokehold on information the academic press was able to create through its monopoly, and we are fortunate more and more individuals (like Steve Kirsch) are leveraging their resources to fully utilize this window.
Note: A complete index of the articles published here on the Forgotten Side of Medicine can be found here.
In all the polls, the majority of respondents (who could respond) noticed a difference. Since the poll results may not show to readers, in a week or two I'll put them all into a graph everyone can view.
Oof.
Direct hit, sir. I kept my own son from taking all but the very first Hep B shot( I was pressured into it, but afterward always refused) and was blessed with a strong, brilliant,and thoughtful child who grew into adulthood.
In his early 20s , he wanted to finish his education at state University,and pressed by his girlfriend, became up-to-date on his vaccines in s very short period.
There followed depression. Then a diagnosis for ADHD , from which he never previously shown signs.
Mid 2022 he and his new wide ( same multi year gf) get covid shots.
Less than a year later, at 26...he's decided he's Trans and he's a girl. She agrees, because she thinks she's non binary.
They both live with me now and I can daily see the personality changes that weren't part of his psychology at age 22.
All this I'd claimed to his dad a couple months ago.
I had hopes that a couple years might see him heal.