Puberty Blockers Are Incredibly Dangerous Drugs
Exploring the Dark History of Hormone Blockers

Providing transgendered children “puberty blockers” is currently one of the most controversial areas in medicine (e.g., liberal colleagues of mine have publicly protested Republican state governments banning the practice).
What I find remarkable about this entire debate is how little knowledge exists about the safety of these drugs. For instance, when I’ve asked my liberal colleagues if they are aware of the dangers of these drugs, they genuinely share that they were not aware they had any clinically significant side effects.
Given that the hormonal blockers are amongst the most dangerous drugs on the market, I feel it is important to review all the people who have been harmed by them, and the scandalous 40 year saga that has allowed them to be unjustifiably used for a wide range of medical conditions.
How Hormonal Blockers Work
There are a variety of ways you can block the production of hormones in the body. Since the signal to produce sex hormones (e.g., estrogen and testosterone) begins in the brain, cutting that signal off mostly eliminates the body’s production of hormones. The most powerful hormonal blockers, the GnRH agonists, work by overstimulating the brain’s GnRH receptors so that they becomes “burned out” and no longer respond to the natural release of GnRH in the body, thereby short-circuiting the body’s production of sex hormones (which in many cases is a permanent short-c).
A variety of different GnRH over-activators are sold, such as Decapeptyl (Triptorelin), Lupron (Leuprorelin), Suprefact (Buserelin), Synarel (Nafarelin), Zoladex (Goserelin). Since Lupron is the most commonly used one, henceforth, I will only discuss it, but much of what I will say about Lupron also applies to the others as well.
Note: there are also numerous similar drugs which instead shut down hormone production by directly blocking the GnRH receptor (e.g., Orilissa). Additionally, there are other GnRH over-activators which are only used in animals and have similar side effects to those observed in humans.
Since testosterone fuels the growth of prostate cancer, there was a lot of research on cutting of the body’s testosterone to treat it. Initially the most promising approach was to counteract testosterone with an estrogen analog (DES) which was eventually pulled from the market because it caused a wide variety of issues (e.g., heart attacks, female cancers, and a variety of severe problems in the children of mothers who took DES—which has led many to argue the COVID-19 vaccines may become “the new DES”).
Since Lupron chemically castrates males (and thereby eliminates their testosterone), in 1984, a study was conducted comparing the use of DES to Lupron for patients with prostate cancer which had metastasized to the bones and was hence likely to be fatal. It found Lupron slightly increased their survival rate (although half still were dead within two years of starting the therapy) and it had a slightly different mix of severe symptoms when compared to DES, which in turn was used to argue it was a viable alternative to DES.
When the FDA reviewed this study, the reviewers noted the study had a variety of serious issues so it was difficult to draw any firm conclusions from it. As a result (despite the FDA knowing Lupron had real longterm risks that had not been investigated and other critical aspects of the drug like how the body metabolizes it remaining unknown to this day), Lupron was approved in 1985 as a “palliative treatment of advanced prostate cancer.” Since that time, Lupron’s approval was never updated. For those interested, a detailed explanation of why that approval was overtly fraudulent and unwarranted can be found here.
Note: in addition to Lupron offering a very small survival benefit, a strong case can be made that since it is frequently observed to causes a variety of severe complications (e.g., a large increase in fatal heart attacks or diabetes), its reduction in the prostate cancer death rate is actually an artifact of it killing the patients before a slow growing prostate cancer would. This perspective for example was shared by the Vice President and Chief Scientific Officer of the American Cancer Society.
Once Lupron was approved, it use transitioned from only the most severe prostate cancers to all of them (even though, as shown by a 2009 study of 19,271 men, using Lupron actually increased the death rate). At the same time, a variety of other copycat drugs entered the market. The FDA in turn approved them (or Lupron) for advanced prostate cancer, advanced breast cancer, endometriois (along with its pretreatment prior to surgery), the pretreatment of fibroids before surgery, and preventing precocious (early) puberty.
Note: while I believe the risks of these treatments greatly exceed their benefits, it is also true that a subset of patients exist with those conditions who benefit from Lupron and suffered minimal side effects from the drug.
Additionally, a variety of other off-label uses were concocted, such as:
•“Treating” every imaginable gynecological problem (e.g., large fibroids, difficult menstrual cycles, ovarian cysts).
•In-vitro-fertilization and egg donation protocols.
Note: many young women are paid thousands of dollars to donate their eggs. Unfortunately, a portion of those donors suffer significant complications they are not warned about beforehand and then are left on their own to address. This is likely in part due to the fact Lupron is frequently part of the protocol. Likewise, significant birth defects (which Lupron has been shown to cause in the majority of pregnancies) are frequently reported following IVF—which may explain why despite Lupron being originally patented as a fertility medicine, it could never be formally approved for that use.
•Chemical castration for sex offenders (e.g., pedophiles).
•Helping children become taller (by delaying puberty so their growth plates take longer to close).
•Preventing puberty in a transgendered youth
.
Note: a more detailed list of the off-label uses can be found here. It is truly remarkable how many different tactics were used to seed these additional uses (e.g., bribing countless doctors and medical charities to promote these drugs) and likewise how many other uses (e.g., for Alzheimer’s disease and Autism) came very close to becoming off-label uses as well.
In turn, there are three important things to take away from all of this.
1. While these drugs were initially developed for men (i.e., prostate cancer), they are frequently given off-label to women. This for example is why Lupron’s FDA insert states its only indication is for the palliative treatment of advanced prostate cancer but it simultaneously warns against pregnant women taking it (even though it’s also used for egg harvesting)
2. Despite having been on the market for decades, there is very little evidence to show these drugs actually benefit those who take them.
3. Given this, along with how incredibly toxic they are (especially to women), it raises a fairly simple question—why on earth are these drugs so popular?
Selling Lupron
Lupron’s manufacturer was stuck with a rather large challenge—how could they got doctors to begin prescribing an incredibly dangerous and ineffective drug? This in turn was accomplished through one of the most overt acts of physician bribery I’ve seen in American medicine.
Since Lupron initially did not sell well, Lupron’s manufacturer took advantage of the existing “standard” which allows chemotherapy drugs to be sold for a very high price and be “forgiven” for their extreme toxicity. This was done by reformulating Lupron into a long acting monthly shot urologists could directly administer to their (prostate cancer) patients and hence directly profit from marking up when they resold it (e.g., Medicare paid 1200 dollars per shot—or roughly 2400 in today’s dollars, and in many cases urologists charged far more, all of which allowed many urologists to make hundreds of thousands of dollars per year administering the shots).
Note: TAP frequently advertised to urologists they could make over $100,000 annually selling Lupron and later cited similar figures to OBGYNs.
To further sweeten the deal, Lupron’s manufacturer frequently bribed urologists and gave them free Lupron samples they “resold.” This was illegal—and eventually resulted in a 875 million dollar fine…but no pharmaceutical executives going to prison.
Because Lupron was immensely profitable, more and more urologists jumped on it, and by the late 1990s Lupron treatments were costing almost a billion dollars per year and accounted for 40 percent of all Medicare payments to many urology practices in the late 1990s. To address this, in 2001, Medicare clamped down on urologists reselling discounted Lupron and in 2003 Medicare lowered the reimbursement for Lupron. In turn from 2003-2005, the rate of inappropriate use of hormonal treatment for prostate cancer dropped from 38.7% to 25.7% and many urologists at the time reported their income had been halved.
Note: one survey found 53% of the urologists who did not believe prescribing Lupron benefitted certain prostate cancer patients still prescribed the drug to them.
Since Lupron was so profitable, many others specialities appeared eager to jump on the Lupron bandwagon, particularly OBGYNs (despite the existing data on using Lupron for gynecological conditions being very poor and in many cases overtly fraudulent). This in turn led to a rapid proliferation of new off-label “uses” for the drug, such as the ones listed above. Remarkably, despite the fact Lupron has been on the market for decades, it is still extremely expensive.
Lupron hence is a very lucrative drug. However it is unclear to me exactly what the current reimbursement is for it (e.g., when I’ve looked online, many patients said they were billed over 10,000 dollars for a single injection).
A recent article exploring the subject found that puberty blockers can cost tens of thousand dollars per year. While insurance typically covers these drugs around 72% of the time, without insurance, according to once source, they cost $4,000–$25,000 per year and according to another source a 3 month Lupron injection is $9500 while a competing 3 month option (histrelin) is $39,000.
Similarly, a 2022 NPR article detailing a man’s prostate cancer experience (where he was given unwarranted Lupron shots) reports he was charged $35,414 for the first shot and $38,398 for the second by a Chicago “non-profit” hospital, and after two years of haggling, was forced to pay the $7,000 not covered by his health insurance.
Let’s compare that to how much Lupron costs (this table designates the average price pharmacies pay to acquire the drug):
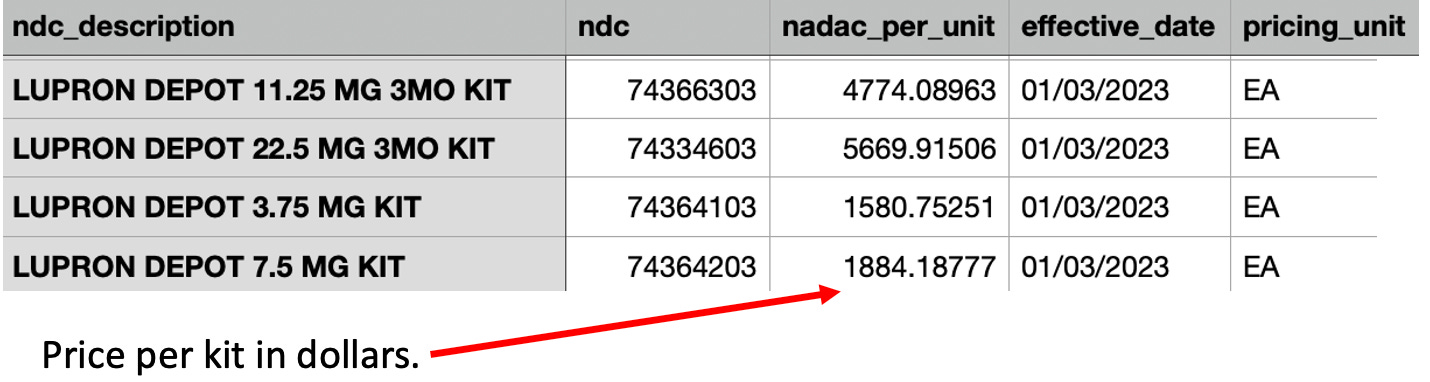
Note: these costs are unusual as they are much higher than what pharmacies typically pay for a drug (especially an older one).
Since all of this demonstrates that Lupron is marked up by 5-10 times its original cost when it is resold to patients, I would argue those who provide these medications may have an ulterior motive in giving them to patients which frequently causes the drugs to be inappropriately prescribed.
Note: one of the most common stories I hear reported from Lupron victims is a tendency for doctors to gaslight them and insist their myriad of health problems could not have come from Lupron, hence making one of their greatest challenges be finding a doctor who can actually help them (or say qualify them for disability since they’ve lost the ability to work). I believe this is partly due to the unusual nature of their injuries and because many doctors have a direct personal investment in believing Lupron is safe and effective (as they aggressively pushed it on their patients—for instance many reported the doctor saying “are you brave enough to try Lupron?”).
Lupron Lawsuits
A curious reality exists with these drugs. To quote Wikipedia:
GnRH analogues [e.g., Lupron] are available as generic medications. Despite this, they continue to be very expensive.
This I attribute both to doctors being heavily incentivized to directly sell these drugs to their patients (rather than cheaper ones made by competitors) and the legal costs associated with producing them.
Since Lupron is so toxic, it had a very high rate of users who were severely and permanently incapacitated by the medication, and hence were willing to go through the arduous process of going to court over it. Since it often took years for the most severe injuries to emerge, this both allowed Lupron’s manufacturer to have the money in place to fight each lawsuit and simultaneously to argue that each injury could not have been related to Lupron. Furthermore, since the legal risk of manufacturing Lupron was so high, I suspect that it scared many competitors away from entering the market as there was a significant barrier towards having enough sales to be able to afford to squash each lawsuit which came along.
In turn, numerous lawsuits have been filed against Lupron’s manufacturer and the doctors who prescribed it, but while some were settled out of court, none to my knowledge were successful, which is extraordinary given that many of the cases revolved about Lupron being used for an experimental (unapproved) use, it causing clear harm to the patient, and it being inappropriately dosed or monitored by the physician (who instead just wanted to give the highly lucrative single injections).
The general sense I have gotten from talking to people injured by Lupron is that they believe Lupron’s manufacturer spent so much on legal defense (e.g., by paying off judges, having the best lawyers or buying gag orders in settlements) that it’s a lost cause to file a Lupron lawsuit regardless of how severe one’s injuries were. In turn, many people have shared they have been unable to find attorneys who are willing take their case.
Note: one of the things we all found remarkable during COVID-19 was how differently the use of “off-label” prescriptions was treated by our authorities. Despite no injuries occurring, nor any money being made, many of the doctors who saved many lives by prescribing ivermectin or hydroxycholorquine were accused of exploiting their patients and faced harsh penalties for their prescriptions (e.g., Meryl Nass lost her medical license).
Lupron Toxicity
I have had a longtime interest in understanding how pharmaceuticals injure people, so I frequently spend lots of time reading through support groups for people who have been injured by them. From this exploration, I have come to the perspective Lupron is one of the most dangerous drugs on the market due to the sheer volume of injuries patients report, how severe the injuries are and just how much many of them are suffering.
Note: in the late 1990s, a lot of public pressure was building against Lupron, and one group, the National Lupron Victims Network came to prominence as a hub for collecting the evidence of Lupron’s harm and advocating against its continued use. Remarkably, in 2000, shortly before the group was supposed to publish all the data it had collected from surveys on the harms of Lupron, without explanation, it suddenly disappeared. This again illustrates just how far Lupron’s manufacturer went to protect their drug.
Within the Lupron support groups, I find by far the most commonly injured are women. This is followed by individuals who took the drugs to halt a premature puberty, then men, and finally transgendered individuals (as they are a relatively new market).
Note: many of the people who took the drugs during puberty are now having adverse effects decades later (e.g., as discussed in this Kaiser Foundation article). This had led me to suspect the same thing will be “discovered” in the years to come for the transgendered children our society has recently started putting on puberty blockers. Remarkably, a 2009 specialist review of using drugs like Lupron for early puberty or making children taller found “few controlled prospective studies have been performed… and [like now], many conclusions rely in part on collective expert opinion.”
Some of the most commonly reported side effects of Lupron include:
•Numerous studies have found Lupron given at all ages significantly decreases bone density (e.g., many have reported between a 3-10% loss occurring after just 6 months) which often results in fractures (e.g., see this study). Bone loss, in turn, is one of the most commonly reported side effects of Lupron (e.g., many young women report having “bones like an 80 year old,” chronic dental or jaw issues like teeth cracking apart and repeatedly developing unexpected fractures from minor stressors). While this bone loss is often rapid, in many cases, it emerges years after receiving Lupron (e.g., women who went on it during puberty in their 30s learn about it because of how quickly the teeth in their mouth are decaying and being told they are not that far from needing dentures).
•Longterm or permanent damage to female menstrual cycles. For example, Lupron’s clinical trials (revealed through ligation) showed that 62.5% of study subjects had failed to return to baseline ovarian function one year after stopping Lupron (which means, contrary to the manufacturer’s claim, the drugs is not reversible once it is stopped). Many other hormonal issues are also frequently reported (e.g., permanent weight gain, painful and abnormal menses, severe hot flashes and vaginal atrophy)
Note: enlarged ovaries and ovarian pain is a commonly reported symptom of Lupron usage (particularly after egg donation protocols) and there is some data which suggests Lupron causes polycystic ovarian syndrome.
•Sexual dysfunction is commonly reported. For example, one study found 80% of males using these drugs reported being impotent, while another found a 267% increase in impotence was observed after one year of treatment, and another evaluation of a related drug found sexual desire, sexual interest and sexual intercourse were totally annulled.
•A variety of psychiatric conditions commonly follow Lupron usage (e.g., a 2002 study of more than 3,000 women on it found 35.5% reported depression). Some of the effects I commonly see reported include anxiety, severe mood fluctuations, major dysphoria, burning rage, suicidality (which sometimes requires being placed on a suicide watch), and losing the ability to function in social situations.
•Cognitive dysfunction (e.g., brain fog or memory loss) is also frequently reported. One study found evaluating women receiving IVF found 72% showed difficulty with memory while on Lupron, some subjects had significant cognitive deficits, and 11% showed very substantial neurocognitive issues.
•IQ loss in children (e.g., one study found a 7 point drop, while another found an 8 point drop).
•Lupron (and related therapies) are associated with a variety of different heart conditions, as Lupron (when used for prostate cancer), according to one paper, appears caused a 10–50% increase in the risks of coronary heart disease, myocardial infarction, strokes and sudden cardiac death (e.g., this study the paper referenced shows a massive increase in heart attacks). Many other concerning heart conditions have also been linked to Lupron and numerous medical textbooks explicitly warn about them. The FDA in turn eventually issued a warning in 2010 about this increase risk of heart problems (and diabetes) in men and acknowledged that no research existed to assess those risks in women or children.
•A wide range of gastrointestinal disorders (e.g. severe abdominal pain, irritable bowel syndrome, or growths that require excisions) and genitourinary (e.g., frequent urination, incontinence and interstitial cystitis) are frequently reported. Many of these likely result from Lupron disrupting the autonomic nervous system and it cutting off blood flow to tissues of the body, which for example is why it shrinks fibroids.
Note: originally, the FDA was extremely concerned about the potential harm which could result from Lupron cutting off the blood flow to critical organs.
•Many Lupron patients report crippling joint pain and severe (early) arthritis. For example, a study of more than 3000 women found that 76.7% reported joint pain and severe pain throughout the body is commonly reported in support forums.
Note: many of these symptoms overlap with what’s commonly reported by patients with ligamentous laxity (e.g., they are hypermobile and have frequently cracking joints). I recently wrote an article detailing how hypermobility is a common characteristic of sensitive patients and its common association with manganese deficiency.
•Immune suppression (e.g., within the bone marrow) and a wide range of severe autoimmune conditions (e.g., Sjogren's, lupus and various thyroid conditions) are frequently reported by Lupron patients.
Note: I have also seen numerous reports of unusual tumors in Lupron users.
What should jump out from this list is how frequent, severe, and wide-reaching these injuries are. This in turn helps to explain why the FDA’s system for reporting drug injuries (which catches 1-10% of those which occur) has received 76,221 Lupron injury reports, of which 41,895 were severe and 11,917 were fatal. Likewise, consider how frequently a myriad of conditions occurred when Lupron was tested in men who had prostate cancer (per Lupron’s FDA package insert):
Anemia (6.6%), Asthenia (7.4-12.2%), Back Pain (5.3%), Blood in Urine (6.6%), Constipation (9.9%), COPD (5.3%), Coronary Heart Disease/Angina (5.3%) Cough (6.6%), Dehydration (8.2%), Dizziness/Vertigo (5.3-6.4%) Edema (5.3-8.2%) Elevated Blood Pressure (6.6%) Fatigue (13.2%) Flu Syndrome (12.2%) General Pain (23.2-32.7%) GI disorders (10.2-16%), Headache (6.4-10.2%), Hot flashes/sweats (46.9-58.9%) Impotence (5.4%), Infection (5.4%), Injection Site Reaction (8.2-19.2%) Insomnia/Sleep Disorder (8.6%), Insomnia/Sleep Disorders (8.5%) Joint Disorders (11.7-16.3%) Joint Pain (9.3%) Libido decreased (5.4%) Muscle Pain (7.9-8.2%) Neuromuscular Disorders (6.1-9.6%) New Cancer (7.3%) Pain While Urinating (6%) Paresthesia (8.2%) Rash (6.6%), Respiratory disorder (6.4-10.7%) Shortness of Breath (5.3%) Skin Reactions (8.5-12.2%) Testicular atrophy (5.4-20.2%) Urinary disorder (12.2-14.9%) Urinary Tract Infection (6%).
Likewise, this is what the FDA reports occurred when Lupron was tested on women for endometriosis:
Acne 10%, Altered Bowel Function (constipation, diarrhea) 14%, Asthenia 8-18%, Breast Changes/Pain/Tenderness 6%, Breast changes/tenderness/pain 6%, Decreased libido 10-11%, Depression/emotional lability 11-31%, Dizziness/Vertigo 11-16%, Edema 5-7%, General pain 8-24%, GI disturbances 7%, Headache 26-65%, Hot flashes/sweats 73-98%, Insomnia/Sleep Disorder 31%, Joint disorder 8%, Memory Disorder 6%, Nausea/vomiting 5-25%, Nervousness/Anxiety 5-8%, Neuromuscular disorders 7%, Paresthesias 7%, Skin reactions 10%, Vaginitis 11-28%, Weight gain/loss 12-13%
Unfortunately, while the above list is terrible (particularly given that the “benefit” of the Lupron in both cases was minimal at best), it should be noted that:
•Pharmaceutical companies always conceal adverse events which occur in their trials.
•This list only includes conditions more than 5% of trial recipients developed while on the drug. In turn, a variety of rarer but much more severe conditions did not make this list.
•This list was not evaluating the long-term effects of Lupron (which are typically the most severe).
Because of how toxic Lupron is, by far the most challenging part of this article was accurately synopsizing the thousands of injury reports I’ve read over the years (as I felt their heart wrenching stories deserved to be heard but simultaneously, there are just far too many for me to fit into any number of articles here).
Generally speaking, Lupron (like the COVID vaccines) causes the body to age prematurely—which in the case of Lupron provides an important insight on the importance of hormones as these victims provide a unique insight into what happens as the body loses those essential messengers (something which also occurs with age). This why in addition to profound bone loss, Lupron also frequently causes other degenerative processes like hairloss, vaginal atrophy, receding gums, and declining vision.
For each of those symptoms (and many others), I’ve read countless testimonials describing the anguish of having their body rapidly age in front of their eyes and the general despair that accompanies decades of suffering with these ailments and the fact there is no one who will help them.
Additinally, one of the most common stories I hear in the support groups are women who profoundly regret taking it for endometriosis as beyond it permanently debilitating them, it frequently did not help (or worsened) their endometriosis.
Note: endometriosis is another condition which is poorly treated by the medical system. Typically the best option within the conventional paradigm is to have it be surgically removed, but unfortunately, there a very few surgeons competent surgeons who do this (e.g., the person we use is an 8 hour drive away from us) and there is also a surprising lack of knowledge within the OBGYN field of how to appropriately manage endometriosis.
Like the COVID vaccine injured, many of those injured by Lupron report not a few, but rather dozens of debilitating symptom. Furthermore, there is often a significant overlap in these symptoms (e.g., both frequently experience fibromyalgia, severe neuropathies, chronic fatigue, headaches, insomnia migraines, hypersensitivities to everything, seizures, and lightheadedness or fainting).
WPATH
Evidence based medicine was created so that harmful and irrational dogmas within the medical field could be overturned by scientific evidence proving there was no justification for doing them. While this was initially helpful, the process gradually became corrupted as the pharmaceutical industry realized doctors could be made to believe only the “best” evidence should be trusted, and the groups purveying the “best” available evidence (e.g., the premier medical journals) could be easily bought out.
Note: Pierre Kory gives an excellent synopsis of the state of our medical journals in his recent interview with Tucker Carlson.
A key part of the push to buy out the “best” evidence has been to create authoritative guideline committees who are tasked with evaluating the existing scientific evidence and coming to a consensus over what constitutes the best practice of medicine—a process which is fairly easy to corrupt since the industry can simply pay off each member of the “expert” committee.
This for example is why Anthony Fauci was allowed to appoint the members of the government committee which decided the standard of care for COVID-19 and Fauci chose individuals who were both his friends and had significant financial ties to his pet drug Remdesivir. In turn, that committee concluded only the extremely expensive COVID-19 treatments (e.g., remdesivir—which was repeatedly shown to worsen rather than improve COVID-19) should be used to treat COVID-19, whereas the safe and effective (but non-commercializable) therapies (e.g., ivermectin) were never allowed into the treatment guidelines despite dozens of trials from around the world proving they worked.
Note: corrupt committees are a recurring problem. For example, the government committee which created the statin usage guidelines we all follow that erroneously concluded everyone needed to be on the statins was filled with people taking money from the statin industry.
In the field of transgendered medicine, much of what is being done is a result of physicians following the existing guidelines that have been created by the World Professional Association for Transgender Health (WPATH). For this article, I reviewed exactly what their guidelines had to say about giving puberty blockers (GnRH analogs) like Lupron to children.
First, they strongly endorsed administering these drugs:
•The moment transgender children begin the earliest signs of puberty as this provides a greater benefit that administering them later on.
•As a stopgap measure for children who have mostly gone through puberty and are considering starting opposite sex hormones but are not yet sure they wish to begin hormone therapy (e.g., due to a disagreement with their parents over doing it).
•For adolescents who are distressed by their body’s menstrual cycles (since the blockers stop menstruation) or penile erections since Lupron suppresses both of them. This is similar to how the guidelines emphatically cite the benefit of these drugs creating “a vast reduction in the level of distress stemming from physical changes that occur when endogenous puberty begins.”
•To help males hoping to achieve a female’s hormone levels do so (as Lupron and its ilk suppress testosterone).
Note: they also acknowledge there are other “individualized” circumstances where someone who has completed puberty may benefit from these drugs.
Second, they advise against using them when:
•The child and their family cannot attain or afford them (in which case specific hormones like progestins are instead used).
•Prior to the earliest signs of puberty. This is because it can potentially interrupt a critical part of their psychological sexual development (however, this logic only applies to very start of puberty and not the rest of it). They do however advise regularly monitoring these children to detect when they start puberty so the blockers can be immediately initiated and provide for a few exceptions where the drugs can be administered prior to the start of puberty.
Third, while repeatedly claiming these drugs are safe and their effects are rapidly reversible, they do lightly acknowledge a few issues in a few specific categories might exist (e.g., “[the use of puberty blockers] is generally safe with the development of hypertension being the only short-term adverse event reported in the literature”).
Note: feel free to skim this section—I wrote it because I felt it was important to accurately depict every single “warning” WPATH provided against these drugs.
Bones:
“While GnRH analogs have been shown to be safe when used for the treatment of precocious puberty, there are concerns delaying exposure to sex hormones (endogenous or exogenous) at a time of peak bone mineralization may lead to decreased bone mineral density. The potential decrease in bone mineral density as well as the clinical significance of any decrease requires continued study.”
“For adolescents older than 14 years, there are currently no data to inform HCPs whether GnRHas can be administered as monotherapy (and for what duration) without posing a significant risk to skeletal health.
“The rate of bone mineralization, which decreases during treatment with GnRHa’s, rapidly recovers.”
“Based on scientific evidence currently available examining the use of GnRH agonists in transgender adolescents, it is unclear whether or not using puberty blockers in adolescence will increase the risk for future fractures in transgender adults.”
“[They] can result in osteoporosis if doses of estrogen given concurrently are insufficient.”
“A prolonged hypogonadal state in adolescence…due to..iatrogenic causes such as GnRHa monotherapy..is often associated with an increased risk of poor bone health later in life. However, bone mass accrual is a multifactorial process that involves a complex interplay between endocrine, genetic, and lifestyle factors [so] all contributing factors should be considered [and] a multidisciplinary team and an ongoing clinical relationship with the adolescent and the family should be maintained when initiating GnRHa treatment.”
Fertility:
They “may also result in menstrual suppression.”
“GnRHas may also be used for menstrual suppression. GnRHas impact the maturation of gametes but do not cause permanent damage to gonadal function. Thus, if GnRHas are discontinued, oocyte maturation would be expected to resume.”
“GnRHas inhibit spermatogenesis. Data suggest discontinuation of treatment results in a re-initiation of spermatogenesis, although this may take at least 3 months and most likely longer.”
“Pubertal suppression and hormone treatment with sex steroid hormones may have potential adverse effects on a person’s future fertility [thus] the potential implications of the treatment and fertility preservation options should be reviewed by the hormone prescriber and discussed with the person seeking these therapies.”
Adversely impacting a gender transition:
The potential negative psychosocial implications of not initiating puberty with peers may place additional stress on gender diverse youth, although this has not been explicitly studied.”
“Treating an TGD adolescent with functioning testes in the early stages of puberty with a GnRHa not only pauses maturation of germ cells but will also maintains the penis in a prepubertal size. This will likely impact surgical considerations if that person eventually undergoes a penile-inversion vaginoplasty as there will be less penile tissue to work with. In these cases, there is an increased likelihood a vaginoplasty will require a more complex surgical procedure, e.g., intestinal vaginoplasty.”
Hopefully, as the previous section showed, WPATH’s depictions of the dangers of these drugs (Lupron etc.) is highly misleading as a large body of evidence exists which overtly contradicts what WPATH put forward. Given that I was able to compile that evidence in a week, it is surprising a team of experts who have spent years working to producing these guidelines were unaware that literature (and likely much more) existed.
The thing I found the most remarkable about WPATH’s guidelines was that while they were unaware of the dangers of Lupron (and its related drugs), they repeatedly referenced certain dangers of giving specific hormones, and in numerous cases characterized the Lupron as safe and effective alternative to the more dangerous hormone therapy. I in turn suspected this is because the blockers cost far more than artificial hormones, and once administered, often require the lifelong purchase of artificial hormones (e.g., to prevent some of bone loss).
All of this led me to believe that like many before them, those involved in writing these guidelines (and some of the authors they referenced) were paid off to promote Lupron and its ilk, but as I have not had the time to do the investigation to confirm this, I can’t state it with certainty.
The WPATH Leaks
Since WPATH has continually publicly advocated for transgender care to be made available to everyon that organization has received increasing scrutiny from the public.
Recently, this resulted in internal documents and correspondences from WPATH being leaked. I reviewed those leaks to see exactly what WPATH’s members were saying in private about puberty blockers. From reviewing all of it, I learned that much like each other group which has promoted the off-label usage of Lupron, WPATH was:
•Not entirely sure what the long-term consequences of this push for those drugs was and in essence, much of what they were doing was a large experiment.
•Recognized that a variety of significant side effects would occur in children who took the blockers (e.g., some would permanently lose their libido or the ability to have an orgasm and many children would lose the necessary emotional developmental process that occurs during puberty).
•Despite claiming otherwise, they knew the effects of Lupron were often not reversible.
•Recognized that the children they were giving the blockers to were too young to fully comprehend the dangers of these drugs but nonetheless were seeking to initiate their use as early as possible.
It’s relevant at this point to note that the puberty suppression experiment began because transgender adult males were dissatisfied with the results of their medical transition because they did not “pass” well as women due to a “never disappearing masculine appearance.” Therefore, the Dutch researchers came up with the idea to use gonadotropin-releasing hormone agonists (GnRHa) to block the testosterone surge of male puberty in the hopes of achieving more feminine appearances in adulthood. The increased risk of false positives due to early intervention was noted, but the cosmetic advantages to adult natal males who identify as women were deemed more important.
Note: WPATH members also routinely discussed puberty blockers being administered to developmentally delayed children (e.g., those with autism), who due to their conditions had an even greater inability to consent to these drugs.
Given all the things I’ve seen the pharmaceutical industry repeatedly do to make money during my lifetime, very few things surprise me these days. Nonetheless, even I was a bit taken aback when I discovered through these documents that there has been a push to affirm “plural identities” (multiple personalities) within WPATH. In turn, there are numerous cases which have been presented at WPATH conferences (e.g., under the umbrella of UCSF—one of America’s premier medical institutions) where each personality of an individual with split personalities was assessed for its sentiments on beginning a gender transition and at least one instance where some of the personalities did not consent but the transition was nonetheless deemed “ethical” and proceeded.
Note: I have compiled numerous cases which demonstrate that the one consistent principle in medical ethics is that whatever makes money will inevitably been seen as the “ethical” choice.
{kind=link}
Conclusion
When you consider the entire Lupron saga, it is truly remarkable that a drug this dangerous has managed to stay on the market for decades, particularly given that it still demands an exorbitant price despite there being numerous significantly cheaper generic formulations which could be used instead. Even more remarkable is the fact that there is no evidence to support most of the things its used for, and now almost 40 years later, that the FDA has still not updated its 1985 approval.
In many ways, the Lupron situation is analogous to what we are seeing with the COVID-19 vaccines. Like Lupron, they are extraordinary toxic and in 1-2 injections, often permanently destroy someone’s health in a myriad of ways—but nonetheless are relentlessly defended by the FDA.
In my eyes, the one bright side to the COVID debacle was that the sheer egregiousness of it (mandating an experimental, dangerous and ineffective vaccine while simultaneously suppressing numerous safe and effective treatments for the disease) opened many people’s eyes to the rot within our healthcare system. In turn, people are now seriously open to ideas like how many young women were severely injured by the Gardasil (HPV) vaccine, the century of evidence that childhood vaccines cause sudden infant deaths, or the notion the vaccines cause autism.
Like Lupron, the people who have suffered from those previous vaccines had done everything they could for decades to alert the public to how dangerous they were, but by and large, their pleas had fallen on deaf ears. However, in the same way the COVID-19 vaccines became heavily politicized (which in turn caused half of America to begin seriously scrutinizing all vaccines), the use of Lupron has also become heavily politicized due to the medical industry’s greedy decision to push the drug on our children.
Because of this, we are now seeing leaks (e.g., the recently WPATH one) emerge which are exposing how reckless and unwarranted certain uses of Lupron are. More importantly, since the issue has been politicized, a lot of people are willing to listen and major groups (e.g., numerous Republican states and England’s National Health Service) are now responding the public pressure and prohibiting this use of these drugs. Similarly, certain states are making it easier to sue doctors who give puberty blockers to children and many lawsuits are now being filed. This in turn is causing the cost of their medical malpractice insurance to skyrocket and in many cases be more than what the doctors can afford, hence is making them be unable to continue giving these drugs to children.
This in turn is what those injured by Lupron had fought for decades to make happen and it is my sincere hope that our newfound public scrutiny on these drugs will make it possible to at last bring awareness to how incredibly harmful its other uses are too. I thank each of you for reading this and your help in bringing awareness to this medical atrocity and everyone (e.g., the forgotten women) who has suffered from those drugs.
A complete index of the articles published here on the Forgotten Side of Medicine can be found here.
The estimated annual amount of money made in the gender industry is about 200B.
What's the big pharma creed? Profits over people.
Thank you for taking the time to write this. I have seen various bits of information in other articles and documentaries, but you do a great job of pulling it all together with history and sources in a very thorough manner. What a travesty that these monsters in medicine have managed to convince some people that medical mutilation is "care" and that exposing our children to these ideas is some sort of ideal "inclusivity". It's a sure sign of a civilization in decline that child sacrifice is considered acceptable.