What Can Megyn Kelly's Adverse Reaction Teach Us About Vaccine Safety?
Exploring the science of vaccination and autoimmunity

STORY AT-A-GLANCE
Since vaccines seek to provoke the immune system into creating an immune response, unintended immune responses to vital human tissues are one of the most common significant side effects of vaccination
When the COVID-19 vaccine campaign started, many were concerned that the experimental mRNA injections had a variety of unique risks for autoimmunity. Rather than require the manufacturers to properly assess that risk, the vaccines were instead brought to market and then mandated upon the world
Autoimmune complications (like Kelly’s) have become one of the most common side effects of the vaccine, and data shows it afflicts vaccine recipients at a dramatically higher rate than normally seen from a pharmaceutical
This wave of autoimmunity is causing an immense degree of suffering and appears to be inflicting profound damage on the entire economy due to the how many people are being forced into disability because of their new autoimmune disorders
Note: this article was originally published on Mercola.com (a website I’ve read for decades). Since publication there it has been revised and updated (e.g., a new section was added).
There were three highly unusual characteristics of the COVID vaccines:
•From the start, they were highly controversial and opinions on them largely split along partisan lines.
•Despite the previous, they were eventually mandated upon the entire population.
•The vaccines had an unprecedented degree of toxicity, to the point so many were injured that the majority of the population is worried about their side effects, almost half of vaccinated American adults believe they suffered an adverse reaction, and half of America believes the COVID vaccines are causing a wave of unexpected deaths.
This in turn has understandably shaken the lifelong trust many Americans held in our institutions and also has created a tragic political situation for the vaccine injured. Since the left strongly endorsed the vaccines, admitting you had an adverse reaction is a direct affront to their tribe. As a result, many liberals I’ve talked to have told me they’ve had to stay silent about their injury or risk being excommunicated.
Likewise, in the medical field, because the faith in the vaccines was so powerful, stating you had an injury was viewed as being equivalent to medical malpractice since it might encourage others not to receive the "life-saving" COVID vaccine. For example, a California doctor who has treated thousands of vaccine injured patients frequently saw local nurses only discover their co-workers had also been injured because they met each other in his waiting room.
The psychological burden vaccine injured people in those industries face is thus hard to put into words—their bodies and lives are falling apart, no one can tell them what to do (or even how to fix it) and if they speak publicly, they risk economically blacklisting themselves. As a result, I know of many VIPs and celebrities who are vaccine injured and are being treated in private but are not going public with it as they are afraid of losing their careers.
Similarly, for those working in the media (which is largely funded by the pharmaceutical industry), regardless of what they see happening to themselves, their friends or their families, they can’t speak out on the issue because of the professional risks they face for doing so. As a result, the only news hosts I know who have spoken out against the vaccine are those who left the networks to build their own platforms.
Note: the one exception I know was Tucker Carlson—who was fired immediately after giving a scathing critique of the vaccine campaign and the media’s complicity in it. Since then on Twitter, he built one of the largest independent media platforms in the world, and has increased his criticism of the vaccines (where amongst other things he stated he never got vaccinated).
For example:
•Sharyl Attkinson, a renowned Emmy-Award Winning Investigative Journalist left her prime time spot after she became fed up with management censoring her stories to became a truly independent journalist. She has repeatedly reported on the COVID-19 vaccine injuries and is hosting a town hall on treating them next week.
•Jimmy Dore, a popular comic who was featured on many major networks, in 2009 started building his own talk show. After being injured early in the vaccine campaign, he got red-pilled and decided to share it with his audience. For example, see this July 2021 interview describes his injury and discusses the hatred those injured by vaccines face:
•In 2017, Megyn Kelly, one of the most popular news anchors in America decided to leave Fox news and then began building her own platform. Like Dore, she now has over a million subscribers on YouTube and has given a voice to outsiders like Robert Kennedy Jr.
Kelly also initially supported the vaccine (see this tweet and her reply to it), suffered a vaccine injury, got red-pilled and has since had the courage (and economic ability) to share her concerns publicly. These remarks (which I’d recommend watching as they touch on numerous important points) were clipped from her recent show:
Note: to provide more context for Fauci’s remarks in this clip, contrary to what he said there, as detailed in Scott Atlas MD’s excellent memoir, Fauci not only zealously supported the lockdowns, but actively sabotaged any attempts to repeal them from both within the White House and throughout the national media.
Specifically in regards to her injury Kelly stated:
I’m sorry I did to myself. … I regret getting the vaccine.
I don’t think I needed it, I think I would have been fine. I’d got COVID many times, and I — it was well past when the vaccine was doing what it was supposed to be doing.
And then, for the first time, I tested positive for an autoimmune issue at my annual physical, and I went to the best rheumatologist in New York, and I asked her, “Do you think this could have to do with the fact that I got the damn booster and then got COVID within three weeks?”
And she said yes. Yes. I wasn’t the only one she’d seen that with.
Note: some have also suggested the tragic sudden cardiac death of Kelly’s sister in October of 2022 may have changed her perspective on the vaccines, but I was unable to find anything confirming this.
Vaccines and Autoimmunity
The adaptive immune system works by producing lots of white blood cells with a random protein sequence on them, and then waiting until an foreign protein (henceforth termed an antigen) comes into contact with a white blood cell whose random sequence matches the antigen. Once this occurs, a signal is set off for the white blood cell to copy itself, and large numbers of white blood cells matching that cell form which can then bind to the new antigen and thereby protect the body from it.
While this approach has served our species well, it’s not perfect because it takes time (the right cell has to stumble across the antigen), and sometimes the needed adaptive response doesn’t form at all. The theory behind vaccination is that since infectious microbes continually reproduce inside the body, by the time an adaptive immunity forms, the infection may have progressed too far and your immunity can no longer save you (or it does but the disease you go through will be much worse).
Vaccines work by introducing one or more of the antigens from the microbe to the body and allowing you to develop an adaptive immunity to it so that when the actual (reproducing) microbe enters your body, your adaptive immunity can kick into gear before the microbe overwhelms the body. While this sounds good in theory, there are a variety ways where it runs into issue in real life.
One of them arises from the fact that for vaccines to be approved, they have to reliably stimulate an adaptive immune response to their antigen. In order for that to happen, vaccines either need to directly inject a lot of the antigen or cause the antigen to reproduce inside the body (e.g., the measles vaccine is a replicating virus), so that in either case, enough of the vaccine antigen can come into contact with the immune system for its adaptive process to occur.
Since antigens are expensive, it’s often not commercially feasible to produce enough of them for an injection to generate the desired immune response. To solve this problem, vaccines are often mixed with adjuvants which stimulate the immune system into responding to the nearby vaccine antigens. Furthermore, some antigens are more difficult to elicit a reliable response from (the ones from HPV being a classic example) and in turn require even stronger adjuvants to be used.
A major problem with provoking the immune system to produce an immune response to the vaccine antigen is that it can trigger an immune response to other antigens as well—such as those the body needs to function. For example, one study showed that mice developed allergies to pollens that were in the air at the time of their vaccination.
This becomes more of an issue when antigens in vaccines partially match those in human tissue. For example, the hepatitis B vaccine has a significant overlap with myelin (which coats your nerves and thereby allows the nerves to function). Because of this, debilitating demyelinating disorders (e.g., multiple sclerosis) have been associated with hepatitis B vaccination, and one study showed approximately half of its recipients also developed immune reactivity to myelin (which in the majority of cases persisted for over 6 months).
Since autoimmunity is a longstanding issue with vaccines, an excellent textbook has been written compiling the numerous autoimmune disorders known to emerge from each vaccine due to the specific makeup of their antigens. Likewise, many have suspected the epidemic of autoimmunity in this country is due to increasing childhood vaccinations as:
•Autoimmune disorders are dramatically lower in unvaccinated children (e.g., see this study and this study).
•The rise of autoimmune (and allergic) disorders in this country has directly paralleled the rise of the number of required vaccinations.
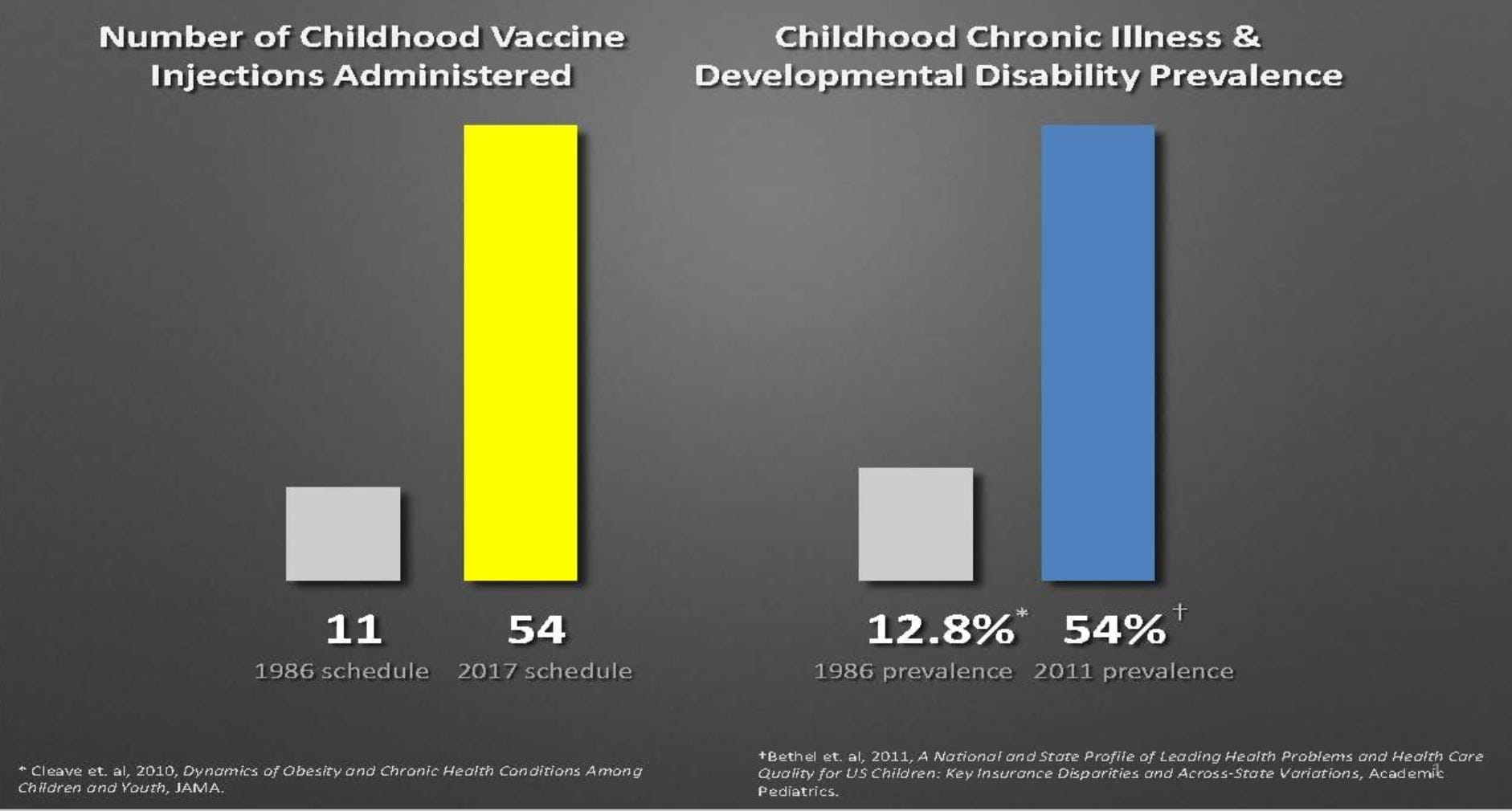
Note: many, but not all, of the disorders listed in the study cited above are autoimmune in nature.
Pharmaceutical Business Models
Over the years, I’ve come to accept that understanding the foundational principles of business is often a far more effective way to predict how medicine will be practiced than understanding the science behind each medical policy—I’ve even had an executive from a major pharmaceutical company (I agreed to protect the identity of) reach out to me and then map out exactly how that happens throughout their industry.
In business, the goal is always to do the following:
•Minimize the risk of each future investment—this is why we see such routine corruption in clinical trials for new medical products (best shown by the recent COVID vaccine trials), and why so many established pathways exist to bribe the government into approving and then often mandating pharmaceutical products upon the country. Bringing a new drug to market is so expensive, that guarantees like this are essential to secure investments in drug development, especially when dealing with a dubious drug fraught with issues.
•Remove any competition from the market that would lower sales of a new drug or reduce the how much it could be sold for—this amongst other things is why we saw such routine and coordinated suppression of existing therapies that could treat COVID-19 but no one could profit off of.
Note: Since we have a pay-to-play approval process, it’s almost impossible to get approval for a therapy unless a lot of money is spent to push it through and that money only becomes available if investors know huge margins exist—something that is not the case for any off-patent therapy. To illustrate, at the start of COVID, I spent hundreds of hours doing volunteer work with one of the many teams that tried to get an FDA emergency approval for a COVID-19 treatment which was already been widely used around the world. The FDA put in a variety of completely unreasonable and prohibitively expensive roadblocks to our project (and in many cases held Pfizer to a radically different standard despite their experimental product requiring significantly more safety testing), which eventually led to us having to scrap the entire project. What I found the most astounding about the whole process was how many people we talked to (e.g., in the FDA) that could not conceive of the idea that we were trying to do this for altruistic reasons.
•Maximize the profit margins on each drug being sold. For example, early in the pandemic (June 2020), despite highly questionable evidence of safety or efficacy, the US government signed a deal to buy the entire supply of remdesivir (approximately 500,000 doses) for roughly 3200.00 per treatment course. It was estimated the fair price for each course of treatment was around 310.00 (while the production cost was approximately 10.00). That’s a big markup—which was made possible by the fact the NIH’s COVID Treatments Panel insisted remdesivir be the treatment for COVID-19…and it just so happened that its members (who were appointed by Fauci) had personally been paid off by remdesivir’s manufacturer.
•Ensure that the products “manage” but do not treat the condition thereby generating recurring sales (as patients often “need” to be on the medication for life). For example, when the COVID-19 vaccines were designed, a decision was made to have them function by mass producing the (toxic) spike protein within the body. Since the spike protein is one of the most rapidly mutating parts of the virus, it was a forgone conclusion that the vaccine would make the spike protein it targeted become extinct and rapidly create a selective pressure for new COVID variants the vaccine did not work on. Had another design been chosen, the resistant variants would have taken much longer to emerge—and hence made it impossible to sell a new COVID vaccine to the world every 6-12 months.
Note: one of the best proofs of this came from a recently developed drug which cured hepatitis C. Rather than this being viewed as a breakthrough (as Hepatitis C for decades has been a debilitating chronic condition), it was attacked by the financial sector as a terrible business move—to the point those attacks were published throughout the mainstream media.
Autoimmune conditions thus represent an ideal market. New and expensive drugs can continually be made to suppress the innumerable parts of the immune system, and since these only suppress the immune response, those patients need to be on the drugs indefinitely. Furthermore, since untreated autoimmune conditions often immediately have devastating consequences, this both motivates the patients to do whatever they can to stay on their drugs and provides a justification to both the patients and medical authorities to accept the severe side effects frequently caused by immunosuppressive medications as a necessary trade off to prevent the complications of the autoimmune disorder.
When the previous is looked at purely from a medical standpoint, it seems inconceivable we would not look at the underlying causes of autoimmune disorders and try to address them—the patients suffer immensely and our entire society pays a high price for these diseases. Yet, when seen from a business standpoint, it makes perfect sense as identifying the causes of autoimmune disorders rather than just suppressing them threatens an absolutely massive market the entire industry (and the drug regulators it funds) all depends upon.
This I would argue is why we’ve continually ignored the link between vaccines and autoimmunity and have essentially done nothing as an epidemic of chronic autoimmune diseases has overtaken the country.
Similarly, it’s also why so many other viable treatments for autoimmune disorders have never seen the light of day. For instance, in a recent article, I presented the evidence that a key cause of acid reflux is low stomach acidity (since the top of the stomach requires a signal of acidity within the stomach to seal and hence not reflux back into the throat).
However, rather than restore stomach acidity or the function of the stomach’s seal, we always “treat” reflux by using powerful drugs that completely remove the stomach’s acidity, leading to a lifelong dependence on them (as the moment a tiny bit of acid comes back into the stomach, reflux immediately follows). As stomach acid serves a variety of vital purposes, chronic use of the most powerful acid suppressing drugs (which are now sold over the counter) creates serious chronic health problems (e.g., they increase your overall risk of death by 19%).
One of the most common consequences of low stomach acid is a startlingly wide range of autoimmune disorders, and for over a century, a wealth of evidence has existed showing that simply restoring stomach acid (and sometimes a few other simple, affordable and very safe interventions) cures a wide range of autoimmune disorders. Yet, almost no one within the medical field is aware of this.
Likewise, one of the discoveries I and many colleagues have made over the years is that treating the cell danger response (a protective state cells go into after they are stressed by their environment) can permanently remove autoimmunity—including for some disorders that are difficult to “treat” with even the most powerful immune suppressing drugs on the market.
Note: I have also come across a variety of other promising treatments for autoimmune disorders (e.g., ultraviolet blood irradiation, removing certain foods from the diet, low-dose naltrexone therapy, or addressing trapped emotional patterns) over the years that I frequently see offer huge improvements for autoimmune conditions. Yet, my rheumatologist colleagues (even the holistically inclined ones) aren’t aware of most of them, which I believe again speaks to the fact business rather than science dictates the practice of medicine.
Warnings of COVID Vaccine Autoimmunity
When the mRNA vaccines were being developed, a few major concerns emerged scientists tried to sound the alarm on, but were nonetheless ignored. One of those was that the vaccine design had a high risk for autoimmunity. This was because:
•The COVID vaccines worked by causing your body to produce large amounts of the spike protein (either with mRNA or through a virus that was modified to have the spike protein on its surface). One of the major concerns repeatedly raised when the COVID vaccines were being deployed was that the spike protein antigen had an extremely high degree of overlap with human tissue (e.g., consider this early 2021 paper). It is basic immunology that infectious organisms which partially match human tissue frequently cause autoimmunity to the matching human tissue (e.g., this is what happens in rheumatic fever), so it was likely something similar would happen here too.
•The longer the immune system is exposed to something, the more likely it is to develop reactivity to it (this for example is why repeated exposures to a food allergen can cause food sensitivities). Since the synthetic vaccine mRNA was modified so it would resist being broken down, that meant its spike proteins would be continually produced for a prolonged period, and hence progressively increase the likelihood of an autoimmune disorder.
Note: we still do not know just how long the spike protein persists in the body since this was never properly tested—one study found the vaccine mRNA was still present at 60 days, a study of vaccine induced myocarditis found that in 25% of those patients, the spike protein persisted in the blood for the duration of the study, and autopsies have found spike protein in the tissue long after vaccination (e.g., at 4 months).
•The vaccines contained both lipid nanoparticles and mRNA, both of which were known to stimulate the immune system, but had not been sufficiently tested on humans, so their potential adjuvant induced autoimmunity was unknown.
Consider for instance what Robert Malone, one of the creators of the mRNA technology shared about about the lipid nanoparticles which he began working with in the 1980s. Here he discusses he and his wife’s repeated attempted to make the delivery of lipid nanoparticles (particularly to the lungs) less toxic and the results of those experiments with mice and monkeys:
And what we found was that they [the lipid nanoparticles] were incredibly inflammatory. They acted to recruit polymorphonuclear cells [neutrophils], recruit macrophage and monocytes, and they would cause the destruction by inflammatory process of lung tissue, very very toxic, and we could not overcome that.
The group at Genzyme did the same work that we did with a much larger team, they produced thousands and thousands of different formulations in different positively charged lipids and they also could never overcome the toxicity. They abandoned the technology at Genzyme and we abandoned it in our research lab and went on to doing other technologies for delivery of DNA and RNA…we abandoned the cationic lipid technology because it was just too toxic.Now flash forward to the present and a research group we had known about and interacted with for a decade at the University of British Columbia, excellent liposome researchers, that we had known about going back to the 70s and 80s had developed new formulation technology that apparently worked in animals and they did a number of things that were slightly different…and came up with something that seemed to work much better in animals which they and others believed would stay at the site where it was injected and would not circulate through the body and that they believed were much less toxic and this was the technology that was used in the current mRNA based vaccine products.
We now know that they were wrong.
In essence, this means that the lipid nanoparticles functions as a strong adjuvant that broadly increases the immune response to the vaccine product—something that has been mapped out in many recent papers like this one. I also believe the positive charges of the lipids nanoparticles (and the positive charges their lipids transfer to cell membranes) play a key role in the vaccine toxicity.
This is because the positive charges of those lipids (and more importantly, the positive charge of the spike protein) caused previously separated cells to clump together, a process that had been known for decades in the vaccine safety field to trigger both microstrokes and autoimmunity both which often are a priority for vaccine injuries (e.g., I frequently find patients improve if their physiologic zeta potential is improved).
Note: there were also significant concerns regarding the effects of the vaccine’s synthetic mRNA on the immune response which Malone explains here.
•The mRNA technology worked by having spike proteins be produced in a cell and then migrate to its surface where the immune system would see them and develop an immune response to the spike protein. The problem with this, especially considering how innately inflammatory the spike protein was, was that it might also trigger the immune system to see the mRNA transfected cell as a foreign invader and develop an immune response to it, potentially destroying both the cell and other cells of the same type.
Note: Since the vaccine campaign started, pathologists (especially those conducting autopsies—some of which were compiled here) have repeatedly observed highly unusual inflammation in vaccine recipient tissue. With a special test, some of these investigators confirmed that the attacked tissue had the SARS-CoV-2 spike protein (but not the nucleocapsid always found in a SARS-CoV-2 infection), indicating this could have only have resulted from the vaccine. To quote one of the pathologists summarizing his research:
A massive lymphocytic infiltration of surrounding non-lymphatic organs or tissue with T-lymphocytes.
Lymphocytic infiltration occasionally occurred in combination with intense lymphocytic activation and follicle formation. Where these were present, they were usually accompanied by tissue destruction.
This combination of multifocal, T-lymphocyte-dominated pathology that clearly reflects the process of immunological self-attack is without precedent.
Because vaccination was the single common denominator between all cases, there can be no doubt that it was the trigger of self-destruction in these deceased individuals.
The above illustrates why it was not a good idea to have cells express an antigen that would trigger the immune system to destroy the cell, especially since many of the nanoparticles could be expected to travel through the circulation and end up in the heart.
•As discussed above by Malone, the lipid nanoparticles traveled throughout the body, which means they could cause the body to develop a variety of different autoimmune conditions depending on which tissues they ultimately arrived at. Later it was discovered (through a Japanese FOIA request) that Pfizer had found the lipid nanoparticles circulated through the body and concentrated in certain organs such as the ovaries (since the ovaries regulate menstruation, this may explain why menstrual abnormalities are one of the most common side effects of the vaccine—affecting almost half of female vaccine recipients).
So, given all of this, you might think that the regulators would have been quite concerned about the potential autoimmune risk of this technology. However when I read through leaked regulatory documents between Pfizer and the EMA (Europe’s FDA), I noticed that very little was done to evaluate autoimmunity and this did not appear to be a priority for the EMA.
Thus, vaccination with modRNA is expected to induce robust neutralising antibodies and a concomitant T cell response to achieve protective immunity. Nevertheless, no further discussion was provided regarding the possibility of autoimmune responses induced by the ModRNA. The Applicant is invited to further discuss the risk that the mRNA vaccine can trigger potential autoimmune responses and how they plan to possibly evaluate their occurrence.
Safety pharmacology programme
No safety pharmacology studies [a more detailed form of toxicology] were conducted with BNT162b2. The Applicant refers to that they are not considered necessary according to the WHO guideline (WHO, 2005). In addition, no findings on vital organ functions have been recorded in the repeat dose toxicology studies. Thus, the absence of safety pharmacology studies is accepted.
Although it is difficult to provide clear cut numbers as it depends on the sought outcome, as a general principle the ETF agreed that for reactogenicity it would be sufficient to test around 300 subjects per age stratum. Serious rare events could be disproportionately represented in children vs. adults e.g. narcolepsy [this was an issue with the 2009 swine flu vaccine] or other autoimmune disorders that are more likely to occur in adolescents than adults. However, such events would require sample sizes larger than 30,000 individuals to be able to detect anything. As this would be unfeasible, especially for a paediatric study, we need to rely on post-authorisation surveillance.
All of this is similar to how they gave Pfizer a pass on evaluating if the vaccine would cause cancer, which, leading into the vaccine rollout was understandably one of the largest concerns with an experimental gene therapy.
Genotoxicity: No genotoxicity has been provided. The components of the vaccine formulation are lipids and RNA that are not expected to have genotoxic potential. That being said, the novel lipids possess an acetamide moiety which is classified as possible human carcinogen (IARC Group 2B) with debated genotoxic mechanism, which should be discussed further.
Note: regulators also oddly failed to require the vaccines to be sufficiently tested for their effects on fertility the other major concern with the vaccine—a subject Arkmedic has done great work to expose.
Experiences With the Vaccine
Since I knew a lot of people were going to ask me about the vaccine, I did my best to research it before it was released. From doing so, I gradually came to suspect that the failure to test the vaccine’s greatest theoretical risks meant it was very possible issues had been already been discovered and that the manufacturers then decided it was better to just not officially test them so the regulators would not have a reason to veto their application and plausible deniability would exist once the adverse effects were eventually discovered. In turn, I concluded the most likely problem with this vaccine would be chronic complications (e.g., cancer) that took a while to show up and would only be recognized once everyone had long since been vaccinated.
As the vaccine started to hit the market, three red flags jumped out at me:
•All of the PR and marketing stated that if you felt awful after the vaccine, that was a good thing and it meant the vaccine was working. I had never seen a vaccine be presented in this way by the media before.
•Pfizer’s study (which was published shortly before the vaccine got approval) had a rate of acute adverse effects which was dramatically higher than I’d seen with any other vaccine (e.g., 59% experienced fatigue from Pfizer's vaccine, whereas around 10-15% experience fatigue after an influenza vaccine).
•Many of my colleagues (who were first in line to receive the vaccine—something I suspect was done to market it to the general public) reported feeling absolutely awful after COVID vaccination.
All of this suggested that the vaccine was extremely effective at provoking the immune system, and given the other issues, that autoimmunity was a real risk of the vaccine.
Once the vaccine entered my community (it took a bit longer to get into my corner of the midwest), I immediately began to have a lot of patients show up with issues from the vaccine. A few things were very striking about what I heard:
•Patients said they had never had a similar issue with any other vaccine (e.g., their annual flu shot).
•Areas of pre-existing immunity flared. For example, joints that for years had occasionally experienced an aching arthritis suddenly felt as though they were on fire. Likewise, old injuries and scars suddenly began to flare and hurt greatly (something I had previously learned to associate with severe inflammatory conditions like Lyme disease).
•A variety of other symptoms were reported which I gradually concluded could be linked to either an inflammatory process or microclotting.
Note: I also began seeing very similar symptoms to what my patients were reporting on a variety of online forums. This recent posting is the most comprehensive summaries I’ve seen of those reports.
Seeing this made me very uneasy, as I felt that if I’d underestimated the vaccine’s acute reactions to this degree, it meant I’d likely greatly underestimated the chronic ones as well.
Before long, I started having more and more friends from around the country reach out to me sharing that someone they knew had died suddenly after the vaccine (most frequently from a heart attack) and wanting to know if it could be linked to the vaccine. At that point I realized I needed to start documenting everything being reported to me (which essentially matched what I was seeing reported online), and a year later I published that compilation, which went viral and made this Substack become part of the vaccine safety debate.
Note: after the vaccines were launched, I also began to hear unusual reports of heart attacks from my colleagues I’d never heard before, but it didn’t occur to me they might be linked to the vaccine until my I started hearing the reports from my friends.
At this point, I began to suspect the primary issue with the vaccines would be autoimmune in nature and or due to the previously mentioned alterations of physiologic zeta potential which led to complications like microclots.
To investigate this, I started contacting rheumatologists and neurologists I knew to find out if they were seeing anything unusual (these would be the two specialities most likely to have patients show up with challenging autoimmune conditions). A few privately confided that something was amiss, but most did not seem open to the possibility there were potential issues with the vaccine and instead kept going back to COVID-19 having a high risk of causing a wide range of complications like autoimmunity.
I then tried a different tactic and contacted medical students and medical residents I knew to find those who were rotating under a neurologist or rheumatologist. I received more candid answers from them; many believed they were seeing far too many patients reporting autoimmune complications from the vaccine.
I then decided I needed to find the time to shadow one of these doctors and was able to do so with rheumatologist. What I saw was very striking—it seemed that around 25%-30% of her patients (some of whom were my coworkers) had either developed a new autoimmune condition after the vaccine or had a long existing (and stable) autoimmune condition become much worse (e.g., one was hospitalized and didn’t remember most of the hospitalization), and frequently required the rheumatologist to change them to a stronger medicine.
Simultaneously, I also began to see unusual autoimmune conditions in my co-workers and social circle (e.g., multiple cases of ALS—something which typically affects only 1/50,000 people per year). One of the most telling stories happened at the very start of the rollout when a close friend received the Moderna vaccine and developed polymyalgia rheumatica (this condition typically emerges in 1/1900 people over 50 each year). I found her story noteworthy because when she saw her rheumatologist, she was told he’d already seen quite a few other patients who developed PMR following Moderna.
Note: I also saw certain autoimmune conditions which appeared to have a delayed onset after the vaccine. This started after I began receiving consultations for multiple sclerosis and noticed they were all either cases that had long been stable and then gradually worsened after vaccination or new ones that emerged months aftewards. After investigating more, I found quite a few other physicians who were also seeing the same thing.
Oddly however, despite a great deal of evidence linking the vaccine to autoimmunity, I have thus far only come across one doctor who was willing to publicly acknowledge this:

When I asked Pierre Kory about this (who specialized in treating vaccine injured patients) he shared that:
I think autoimmunity is one of the key pathologies that underlies many of their symptoms but they don’t always meet the classic criteria for a specific autoimmune disease with the standard autoimmune panels, although more specialized autoimmune tests consistently detect a wide range of auto-antibodies.
Note: the other key pathology is pervasive microclotting. Additionally, one common autoimmune disorder which frequently follows vaccination is antiphosopholipid syndrome, a very rare condition known to dramatically increase one’s risks of blood clots, infertility, strokes and heart attacks. I believe this risk is at least partly due to cell membranes (where the spike proteins end up being seen by the immune system) being largely composed of phosopholipids.
The Data on Vaccine Autoimmunity
Numerous datasets exist suggesting there is a high risk of autoimmunity from the vaccine. These include:
•An Israeli government study which found that 24.2% of those receiving a booster developed an exacerbation of a pre-existing autoimmune condition.
Note: COVID vaccine side effects typically worsen with each successive vaccine dose, something consistent with an immunological sensitization or a cumulative worsening of the physiologic zeta potential.
•A rheumatologic database published in the BMJ showed that 37% of patients had an adverse response to COVID vaccination, and 4.4% of those vaccinated experienced an exacerbation of a pre-existing autoimmune condition.
Note: This database only sampled patients with a pre-existing rheumatologic condition and it is not possible to know what fraction of the adverse events (reported in 37% of those patients) were autoimmune in nature.
•Heart surgeon Dr. Steven Gundry performed a test that utilizes inflammatory markers to predict the risk of an acute coronary syndrome (e.g., a heart attack) in the next five years on 566 patients and found that before vaccination their risk averaged 11%, while afterward, it averaged 25%.
I must emphasize that these are all massive and unprecedented increases. The only two pharmaceuticals I can think of that had a similar ability to create autoimmunity were the HPV and anthrax vaccines.
Conclusion
While I feel terrible for Megyn Kelly’s adverse reaction, I hope that this article serves to illustrate that her development of a new autoimmune condition was not all that uncommon and that doctors should have been aware of these risks before they pushed their patients to vaccinate (especially for patients with a tendency to autoimmunity due to pre-existing autoimmune disorders). Sadly the opposite happened, and those with pre-existing autoimmune conditions were instead told it was urgent for them to vaccinate since they were immune suppressed and at a higher risk of getting COVID-19.
One of the things that’s difficult to appreciate about autoimmune conditions (unless you have one) is just how incredibly impactful and debilitating they can be for one’s life. For example, my friend who developed PMR couldn’t function for months and two of the doctors I worked with when the vaccines were introduced suffered debilitating (and life-threatening) complications which caused them to have to leave the facility because they simply could no longer work.
Ed Dowd and his team has been attempting to quantify the economic impact of these injuries. Large numbers of life insurance claims filed (for sudden deaths) and large numbers of people exiting the work force due to vaccine induced disability have massive costs to the society, and most importantly, these costs are big enough to threaten the profits of upper class (which may in turn motivate those in power to fix the problem).
Dowd’s (conservative) estimate was that 18% (26.6 million) of the American workers who received the vaccines were injured, 0.93% (1.36 million) were disabled, and 0.05-0.1% (300 thousand) died. One database they identified, which shows England’s monthly disability clearances sorted by the cause of the disability helps to illustrate how vaccine injuries are affecting from the workforce. Specifically, when compared to the existing trend prior to the vaccines being introduced, autoimmune conditions resulting in a disability approval increased by between 100%-400% (depending on the condition). This represents 4-10 standard deviations from the mean, something that is statistically impossible to have happened by chance.
Note: the specific autoimmune conditions in England’s dataset were lupus, vasculitis, Sjogren's, antiphosopholipid syndrome, systemic sclerosis, "other autoimmune diseases," and "other diseases of the immune system."
Having worked in the disability approval process, I can share that it is quite hard to get disability, and that the majority of people seeking disability sincerely wish they could work instead. While my experience is in only in America, I suspect a similar situation exists in England, which again underscores the immense human cost of the COVID vaccine’s autoimmune complications.
I tried every way I could to convince my wife not to have more than the two initial Pfizer shots we had at the end of Jan 2021 ending in Feb 15, 2021. Forced her to sit down and watch successful early treatments in Imperial Valley CA and Honduras. To no avail. She went ahead and got 2 more shots.
Now she is suffering from bursitis and tendonitis. Extremely painful. She heard from a friend that taking boron helped so she just started taking it.
I will forward this substack to her but even thought she is extremely well read on many diverse subjects including medicine and nutrition. She is so aligned with the safe and effective narrative that she would deny that the vaccines could cause injury.
This means that when I again suggest that vaccines might be involved in her current condition, I expect to be facing a blank stare. Even extreme pain in her own body is not enough to break through the ideology of the medical monopoly.
I was a medical student on clinical rotations during 2021 and 2022. The most memorable neurologic case I followed was a 36-year-old man who was hospitalized in February 2022 for evaluation of new onset neurologic symptoms causing significant weakness and functional impairment, such as limb weakness and balance problems as well as some sensory changes. These symptoms had been ongoing in previous months and resolved with steroids, but returned, precipitating his hospitalization. He had no personal or family medical history of neurologic or autoimmune disorders. Of note, he had received his first booster 3 weeks prior to his presentation at the hospital.
The patient had a mixture of neurologic findings localizable to different tracts, which is common with autoimmune demyelinating disorders such as MS. And his MRIs showed demyelination. However, a full autoimmune workup yielded no positive results. The neurologists following him figured that there are so many different proteins/antigens in the body and nervous system that one could develop antibodies to, that someone could have illness from antibodies towards a self antigen not included in the usual autoimmune or neoplastic panels. The patient consistently responded well to high dose steroids (which suppress the immune system) and plasmapheresis (which removes antibodies from the system), further supporting an autoimmune origin. He often asked if the Covid booster could have been related to his symptoms, and the neurologists considered it as a likely possibility in light of the otherwise negative workup. I remember clearly this kindhearted young man telling the team he had gotten the booster because he lived with his elderly mother and wanted to protect her.
Based on this reasoning, the patient was offered and agreed to start treatment with rituximab, an immunosuppressant medication. The next day, he developed respiratory failure from flash pulmonary edema, an extremely rare side effect of the medication (only documented in a few case studies). Ultimately he required intubation, developed a wide complex tachycardia with 2 separate cardiac arrests, had VA ECMO placed (an advanced life support system that essentially functions as the body's circulatory system), and was transferred to the ICU. After almost 2 weeks, the patient's family decided to transition to comfort care measures and the patient passed away.
The other student and I who had been following this patient were greatly saddened to learn of his passing. While it was not the proximal (or confirmed) cause, he became known among some of the students and residents who had followed him as "the man who was killed by the Covid vaccine". It especially saddens me when I think back to his reasoning for getting his last booster, protecting others, when the data showing that the vaccines did not prevent infection or transmission was already available months before early 2022.