Early Health Innovators and DMSO
Key lessons for the present from the history of DMSO

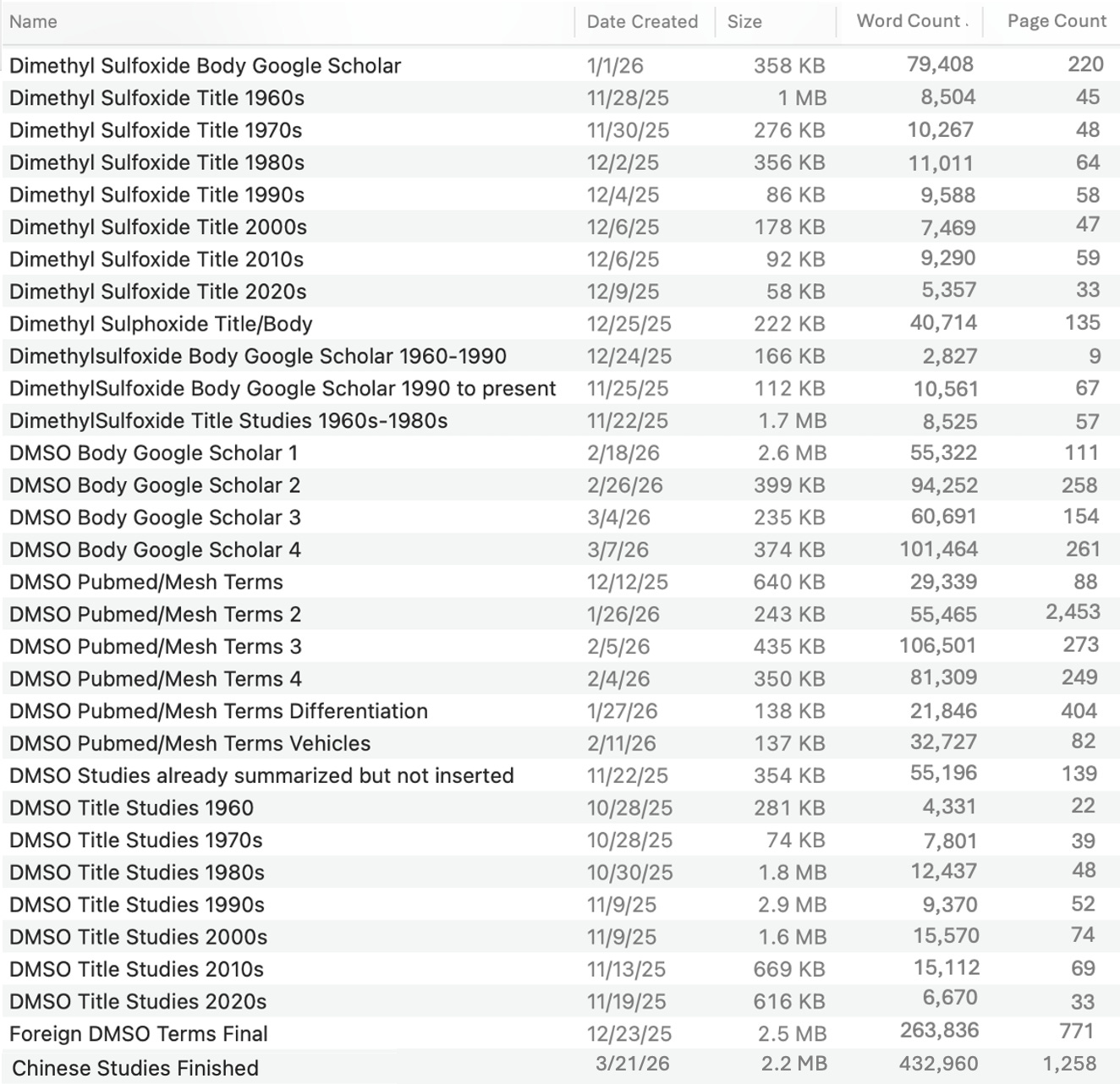
One of the things I never cease to be amazed by is how cyclical history is, and how similar many situations we find ourselves in now are to ones I’ve read about far in the past. Over the last six months, I have been attempting to compile (almost) every medically relevant paper ever written on DMSO, and in that process, skimmed through hundreds of thousands of search results (which were filtered from millions of hits) to flag each study I needed to sort and summarize, which with the help of AI, resulted in this:
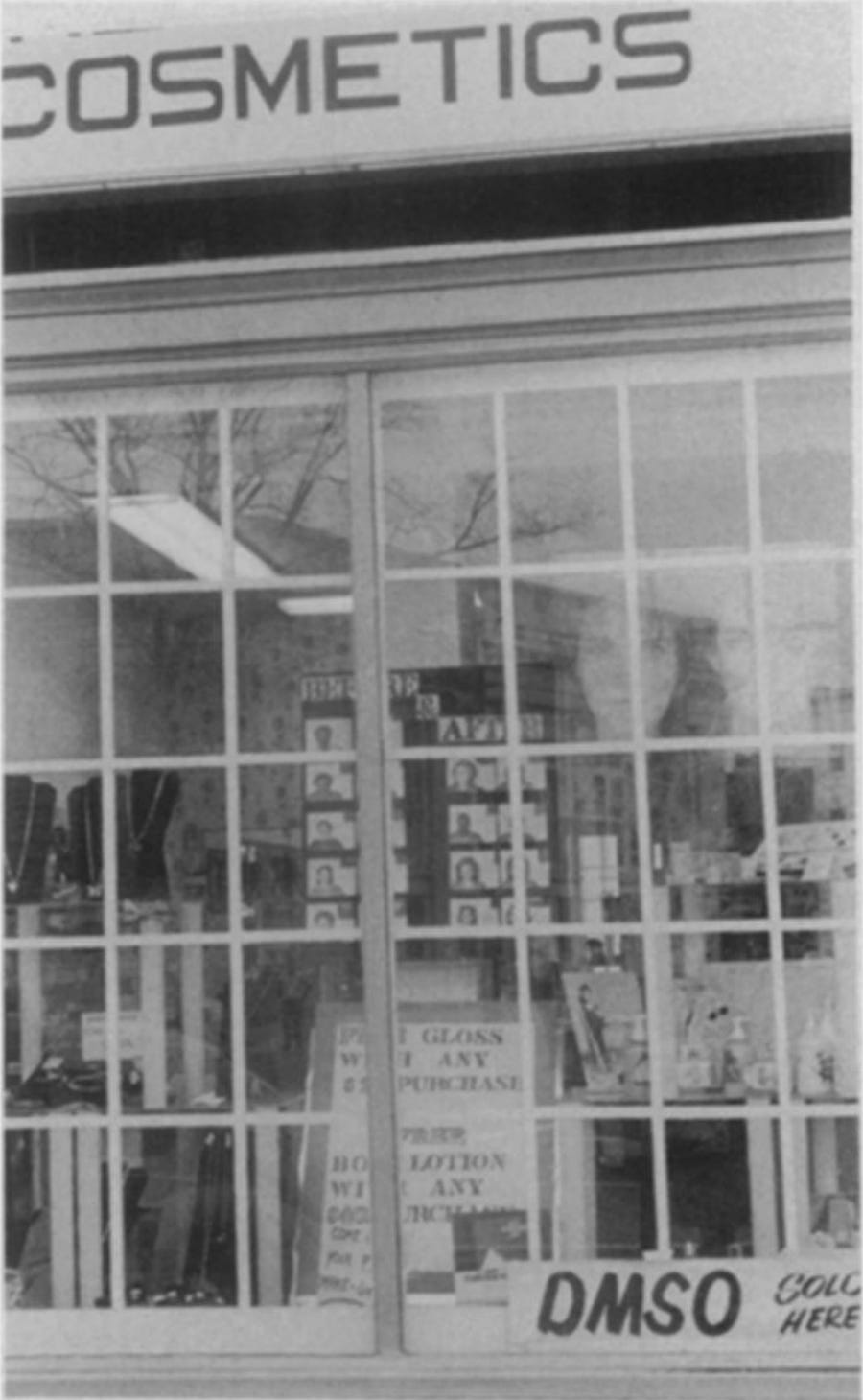
From that process, I came across many papers detailing the history of DMSO, and while many essentially retold parts of the story in Pat McGrady’s book (The Persecuted Drug: The Story of DMSO), many also contained things I never expected to come across. For example, I remember in the 1980s that gas stations would have signs saying “we sell DMSO,” but try as I might, I could never find a picture to prove this. However, during that project, I eventually found this in a 1982 article, which, while not a gas station, was pretty close:

Of these, papers on the history of DMSO, one caught my eye as it contained numerous lessons which hold just as true now as they did more than forty years ago.
A Brief History of DMSO
DMSO is a naturally occurring substance that is found throughout nature and routinely studied in climate research as it forms a core part of the sulfur cycle many microbial organisms rely upon. Discovered in 1866 by a Russian chemist, it was mostly forgotten until the 1950s, when an emerging need for new chemical solvents prompted the paper industry to meet that demand by oxidizing the dimethyl sulfide (DMS) wood pulping produced into DMSO.
Note: the cycle between DMS, DMSO, and DMSO₂, beyond underlying many critical ecological processes, also explains why DMSO causes some users to experience an odor, and will be the focus of a future article (but in the meantime, an abridged version on how to reduce the odor some DMSO users experience can be read here).
Before long, one pulp and paper company, Crown Zellerbach, was the primary producer of DMSO, and assigned a chemist to see if there were other uses for the tree solvents they produced. Herschler accidentally discovered that DMSO could carry dyes into the skin, and also quickly realized the immense value of this with antibiotics and antifungals to treat infections normal medications could not reach. Serendipitously, Stanley Jacob, a renowned surgeon at the nearby Oregon medical school had been searching for a way to cryopreserve organs that would be transplanted, and had recently come across a revolutionary study suggesting DMSO could function as an effective cryoprotective agent.
So, when Herschler, in 1961 shared his discovery with Jacob, Jacob enthusiastically explored it, and after tasting iodine shortly after mixing topical DMSO with it, realized this drug rapidly facilitated systemic absorption, revolutionizing pharmacology. Shortly after, they discovered it rapidly treated burns, then sprains, and then a wide range of musculoskeletal issues and before long, Jacob started carrying it on him to address whatever ailment someone he ran into had (with DMSO often working). These remarkable cures inspired Jacob to invest his career, personal time (despite having a family) and savings into DMSO research, and then remarkably, once he was broke, his dean agreed to have the medical school fund his research.
Note: once DMSO began being used in a medical context, the pulp production method was abandoned as it could not produce DMSO pure enough for medical applications.
The results Jacob got attracted immense attention, and before long, numerous pharmaceutical companies had heavily invested in studying DMSO, while in parallel, the media (e.g., The New York Times) widely promoted it (e.g., a 1965 NYT editorial called it “the nearest thing to a wonder drug the nineteen-sixties have produced”) and DMSO quickly became the most demanded drug in America. Initially, the FDA was extremely open and supportive of this, but due to the public outcry over the thalidomide disaster Dr. Kelsey prevented (which caused Congress, in 1962, to grant the FDA strict regulatory powers), the FDA switched to needing “well-controlled” evidence of drug efficacy they would meticulously evaluate for a drug to be approved.
Before long, due to just how many different uses DMSO has (each of which drug companies were applying to receive approval for), this became a major issue:
' 'The FDA representatives [in 1964] seemed anxious to do everything possible to permit further testing of DMSO," Jacob told me later. "They pointed out that DMSO was a very versatile drug; and because of this they were a little apprehensive as to how many IND applications might be filed to test not only DMSO alone but DMSO in combination with various other pharmacologically active substances. "Dr. Kelsey said the number of combinations could be a hundred or more, representing a formidable challenge for a bureau that already was overburdened."
Laziness won, and the FDA began looking for reasons to stop this. Eventually in late 1965, settling on preliminary data in dogs showing high doses of DMSO could change how the eyes focused (which was never reported in the trials being conducted on 37,000 people or subsequently in humans or monkeys) and a single death (that has never occurred since and was likely due to an allergy to another drug being taken concurrently), the FDA not only banned all DMSO testing in the United States, but sent out global telegrams to each embassy encouraging other nations to do the same. Following this, the FDA, eager to assert its newfound power, then began a relentless campaign to intimidate doctors and scientists into not conducting any further DMSO research (which, I believe is a large part of why researchers now are so reluctant to ever study “unorthodox” topics).
Note: the playbook the FDA used against DMSO was also used against many other remarkable (now largely forgotten) medical therapies.
Fortunately, the scientific community had not yet lost their spine, and fought back, with Jacob organizing three American symposiums (one in 1966, along with one in 1974 and in 1982—along with a 1965 one in Germany and a 1966 one in Vienna). Sadly, despite the wide range of data presented, the FDA dug in, insisting there was “no evidence” DMSO worked for anything, and eventually, in 1980, a Congressional and Senate hearing were held on the FDA’s stonewalling, where the FDA repeated a variety of excuses and made a series of promises to stop stonewalling DMSO (which not surprisingly, were never followed).
Note: the first therapeutic FDA approval for DMSO (DMSO for interstitial cystitis) happened in 1978, and I suspect was motivated by the FDA wanting to create the impression they weren’t stonewalling DMSO drug application prior to those hearings (as no subsequent approvals ever happened despite many being sent in).
To support these 1980 hearings, Mike Wallace (of 60 Minutes) aired a program immediately before the first one, which introduced the public to DMSO, and created a new wave of widespread interest in DMSO (after the FDA successfully squashed the first one in the 1960s).
Following this, DMSO experienced another surge in popularity, but gradually was forgotten except by certain segments of the alternative health community and veterinarians (who widely use it in practice). Likewise, with American research, while there was initially a huge surge of it (particularly in the 1960s) it greatly declined, and by the 1990s, therapeutic studies of DMSO in humans or animals were rarely conducted. Instead, medical research in DMSO (besides its approved use for treating interstitial cystitis) largely shifted towards it:
•Being used as a cryopreservative
•Being used as an “inert” (harmless and non-beneficial) solvent to test a wide range of potentially therapeutic substances (predominantly in cell cultures).
•Making cancer cells revert to normal cells (which is often needed for research).
•Facilitating other therapies (e.g., there are now well over a dozen FDA approved drugs which contain DMSO as an “inert vehicle”).
Fortunately, in 1971, after extensive research the Soviet Union’s Ministry of Health approved it (as Dimexide/Dimexid/Димексид), and as a result, much of the forgotten data on DMSO’s medical uses comes from the Russian and Ukrainian literature, along with a smaller amount from Chinese, South American, and German researchers (most of which I have finally been able to compile).
Note: this history is covered in much more detail here.
Early Innovators
Propaganda essentially works because most humans want to follow the crowd, but simultaneously, there is always a small portion of the population which will trust their gut and have the courage to pursue things that aren’t yet “safe” to do because neither authorities or their peers are telling them to (e.g., despite the most aggressive propaganda campaign in history, immense peer pressure and increasingly strict vaccine mandates, roughly 25% of Americans did not get the COVID vaccine).
This blog in turn is catered to the self-directed “innovators” and “early adopters” as my goal as much as possible is to provide all the essential information one would need to understand a topic and then be able to figure out how to approach it, rather than giving you a set protocol for everyone to follow and “telling you what to do.” This I believe is essential, as virtually every therapy, despite having a standard dose, typically needs to be dosed differently for different people (and I believe many medical injuries with pharmaceuticals could be avoided if lower “non-standard” doses were used for more “sensitive patients”).
However, the education system trains everyone to repeat formulas and instructions rather than creatively thinking on their own, so the standardized model persists, and the harm the excessive doses create are simply viewed as a necessary cost of doing business. This is unfortunate as while (clean) DMSO has a fairly wide therapeutic window (so, unlike many far more toxic drugs, it is very difficult to take a DMSO dose which is high enough to be dangerous), the correct DMSO dose greatly varies from person to person. As such, many commentators (beginning with Jacob) have remarked that while it is incredibly easy to determine the correct dose for a unique patient you work with, DMSO lacking a “standardized dose” has been one of the most challenging aspects of widely deploying the drug.
Note: this is why I have to include about 8 pages of instructions on general DMSO use at the end of each DMSO article (e.g., I did so most recently here), along with a similar amount for specific conditions being discussed within a given article. This has worked for a lot of people (particularly early innovators), but simultaneously, many have not wanted to read through the instructions and instead simply wanted a simple universal protocol (which will inevitably not work for some of those who use it). This is quite challenging to navigate, and my approach has essentially been to hope that if I can provide enough clearly laid out information, the early innovators who see it can understand how to translate that to people they meet who just want a single protocol to follow.
The phrase “early innovators” in turn came to mind due to a noteworthy 1985 article which I read during the DMSO project (“DMSO, Hobby Shops and the FDA: The Diffusion of a Health Policy Dilemma”) which discussed DMSO and the diffusion of innovations (e.g., their adoption).
Note: the dilemma being referred to was that since DMSO was legal as an industrial solvent, the FDA could not ban it, and instead could only restrict people implying it had medical uses.
History Repeats
When I created this newsletter, one of my primary goals was to get (hard to find) information out there on effective forgotten therapies that told you what you actually needed to know about them in the hope I could spread it out enough that people who were genuinely interested in the topic would eventually be able to find it. However, due to the highly unusual era we are in now, far more happened, and due to the DMSO series here going viral, I essentially created the third wave of interest in DMSO.
DMSO, Hobby Shops and the FDA: The Diffusion of a Health Policy Dilemma, in turn, caught my eye as virtually everything it described in 1985 perfectly mirrors what has happened with DMSO over the last two years. As I cannot quote the entire article here (much of which came from interviewing DMSO users who responded to a newspaper ad), I will try to highlight the most poignant parts:
We learned that DMSO is being used for an astonishing range of ailments. In order of reported frequency, these include: Osteoarthritis, rheumatoid arthritis, back injuries or pains, stiff or painful necks, knee injuries or pains, bursitis, ankle sprains, tennis elbow, hip pains, muscle spasms, burns, decubitus ulcers, psoriasis, headaches, varicose veins, scleroderma, insect stings, emphysema, cataracts, and toothaches. Actually, these are only a few of the claims being made for the curative powers of DMSO. Clearly, it is a substance that could touch many lives.
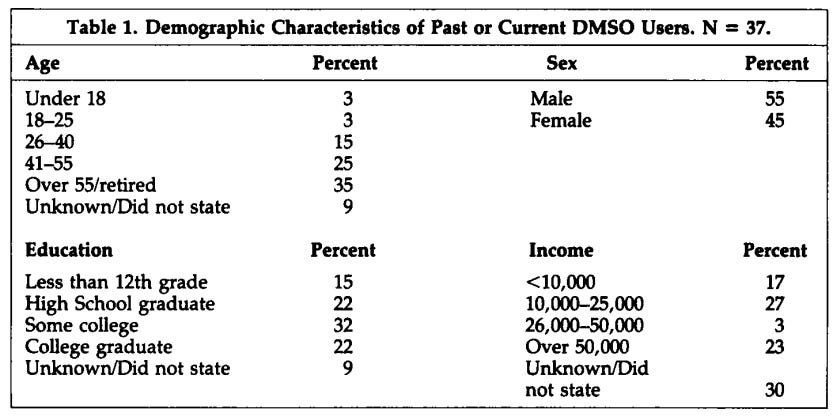
The users are as diverse as the uses (see Table 1)
Rogers and Shoemaker speak of five key innovation characteristics that may facilitate or impede adoption: relative advantage, compatibility, complexity, trialability, and observability.
They observe that there are a number of subdimensions of relative advantage including ". . . low initial cost, lower perceived risk, a decrease in discomfort . . . and the immediacy of reward." For most of the respondents, DMSO had these attributes.
Moreover, the absence of effective medical remedies for arthritis and soft tissue injuries combined with these relative advantages, make DMSO an attractive alternative. Regardless of whether a possible placebo effect was operating, most of the interviewees reported rapid decrease in pain and increased mobility with few perceived side effects and a low price.
Fairly typical of our interviewees were statements like the following: I wasn't able to stand up and swing my left leg because of my knee pain. . . after two treatments of DMSO I could do it with no pain whatsoever. . . I cried because I could swing [my legs] almost like I was doing a can-can. I had not been able to walk up stairs for five years ... I used DMSO three times on my right hip and I now can climb stairs without any pain . . . I was severely burned when I spilled scalding coffee on my lap . . . I went to a burn center and they wanted me to stay but I did not want to because I had this trip planned to see my mother in Iowa . . . I started applying DMSO and it healed miraculously and I got to go on my trip . . .
The lack of approval by the FDA and other medical authorities may both lessen and reinforce the relative advantage of DMSO. While many interviewees are fearful of using an unapproved substance, other interviewees see the lack of approval as a confirmation that DMSO works. This paradox is explained through an interpretation which sees restraint of trade, not scientific caution, as the real explanation for the FDA failure to legitimize DMSO. If DMSO became legal, they argue, doctors and drug companies would lose a good deal of money. Therefore it must be good or "they" would let it on the market. Thus for some, the relative advantage of DMSO may even be strengthened by official non-approval.
Note: the next part of the article discusses how many being familiar with topical pain ointments, having already used DMSO in animals, or having a vet suggest it to someone for an “incurable” issue they’d seen DMSO treat in animals made it compatible (familiar) and hence likely to be adopted.
In addition to a strong relative advantage and high compatibility, DMSO compares favorably to other remedies because of its perceived low complexity, that is, ". . . the degree to which an innovation is perceived as relatively difficult to understand and use" For most people, there was no problem in learning how to use DMSO despite an almost total blackout on information, education, and instructions.
Vendors are fearful of FDA action and so are very guarded in what they say. A fairly routine story was related by one respondent: When I asked them what do I do with it they [vendor] said "I don't know," and I said just give me a little idea how to put it on and they said mix it with the paint and I said that's not what I'm going to use it for and they said "I don't want to hear any more." . . . they were kind of cold.
Note: this article also highlighted the immense confusion and variation with using DMSO (that users eventually somehow figured out) and that they experimented with topical DMSO combinations such as vitamin E oil or corticosteroids.
Although it often produced a skin burn or an unpleasant odor, these effects were welcomed by some as a positive sign. As one woman said, "If it doesn't smell or give a burn I'd throw it out because it wouldn't be the real stuff ... I know it's good, it burns ..." Users either tolerated these effects or applied creams and ointments just as they would do with other skin irritations. The distinctive odor was more often a source of amusement than worry.
Trialability means that a user can experiment with an innovation on a limited basis. DMSO was used in this way by nearly all the respondents. Those who found no relief stopped using it after about a week; one individual kept applying it for four months before the pain "suddenly" went away. It is an innovation that is eminently suited for trial on the installment plan, an important advantage for those who either are wary or without great financial resources. DMSO could be tried and discarded without much financial or any apparent physical harm
The degree to which an innovation is visible to others is labeled observability. DMSO is not highly observable in the sense that the absence of pain is not something someone else can see. However, we repeatedly found that those who used and liked DMSO did not hesitate to tell their friends, relatives, neighbors and, in some case, complete strangers. Word-of-mouth has been an important factor in making DMSO "observable" to many who otherwise would not have considered it….For this reason DMSO, despite its "illegality," has achieved a high positive observability.
It is not enough for a substance to have the requisite qualities of advantage, compatibility, reduced complexity, trialability, and observability. It must also become known. Just how did DMSO come to the attention of so many Americans? [In most cases, their initial interest was due to viewing the 60 Minutes program].
Many interested viewers naturally turned to their physicians; however, they soon learned that DMSO cannot be legally prescribed. Moreover, most physicians were either indifferent, uninformed or hostile; one respondent reported that his doctor refused to continue to treat him because he was using DMSO. Many did not even bother to tell their doctors often out of fear of just such a reaction. As one woman related: “I didn’t know who to call ... didn’t call my physician because he would climb the wall if he knew that I thought about using it ...” However there were a few physicians who were either neutral or had even tried DMSO themselves. Some respondents said their physicians were curious and asked the patients to let them know if it helped.
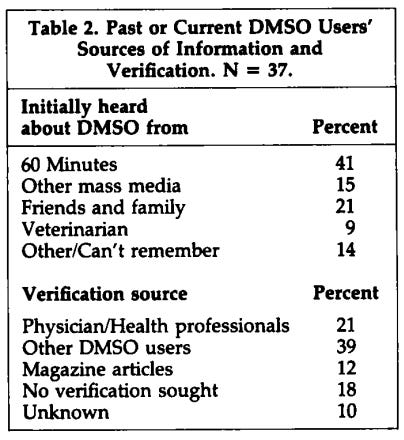
Thus, given the indifference or active opposition of most health professionals, many users started asking among their friends or relatives who had used DMSO, reading articles in papers or magazines or just using it without any verification or information. Those who felt that DMSO had helped them became in turn sources of information, and in a more than a few cases, active proselytizers. Some reported recommending it to up to a dozen people, including strangers who complained out loud in public places about aches and pains. Table 2 highlights the respondents' reports of their DMSO information and verification sources.
The article then concludes by highlighting that the FDA’s refusal to regulate DMSO in a responsible way has led to hundreds of thousands of Americans using it in an unregulated manner (the situation the FDA wanted to avoid) and criticizing programs like 60 Minutes for irresponsibly using “the enormous power electronic media now has over the health field” (whereas downplaying DMSO’s benefits would have been the “responsible choice”).
Conclusion
I have long believed one of the greatest mistakes humans have made throughout history is believing they can fully control fate and prevent the inevitable natural emergence of anything which challenges what they want. Because of this, again and again, I see the same historical dramas play out, and each time the rulership tries to suppress them from emerging, they temporarily disappear but then eventually emerge in a far more powerful manner.
For example, the smallpox vaccines were never proven to work, caused severe injury (that doctors covered up), and not only frequently failed but often caused smallpox outbreaks (detailed here). The public resisted this, and in response (to address the increasing outbreaks) harsher and harsher mandates were instilled. This lead to massive public protest against the vaccines and eventually, in 1885, an English city making vaccination optional alongside employing basic public health measures to contain smallpox. Contrary to the medical field’s apocalyptic predictions, this worked, and those public health measures were then copied, allowing smallpox (due to it not being very contagious) to be eliminated.
I mention this because I started this newsletter during the COVID-19 mandate protests (e.g., the Canadian truckers) as I realized we were re-enacting the exact same thing and people needed to know so we could break that dysfunctional cycle. Incredibly however, rather than it taking nearly a century (1976-1885) to stop the shots, it happened in two years, and public opposition now to the COVID vaccines is much greater than it ever was to the smallpox vaccine.
Similarly, due to the fanatical devotion the current rulership has to vaccines, for decades, any suggestion they cause harm is unilaterally censored, and the careers of those who speak out against them are destroyed. Nonetheless, because vaccines injuries are cumulative, as time goes on and more and more are given to us, the injuries have continued to increase, and in the last few years, reached the point it is no longer possible to cover them up.
Because of that, we have now seen rather extreme swings on this issue no one in the field previous imagined could happen (e.g., RFK becoming HHS Secretary, and the President openly speaking out about vaccines neurologically damaging children). Likewise, we are now seeing every stop be pulled out to protect vaccines (e.g., a wide coalition of Senators have been prioritizing targeting any political appointee who does not openly pledge allegiance to vaccines), and in the last week, to prevent ACIP (the committee which decides vaccine policy) from finally, after decades, allowing those injured by vaccines to publicly testify:
•Fake polls were made to convince the Trump administration the entire public loves vaccines (when in reality, most polls now show roughly half of Americans distrust vaccines) and then amplified by the mass media (e.g., The New York Times) immediately before the midterms.
•Damaging ACIP reports were “leaked” to the NYT (so a major hit piece on the upcoming meeting could be published three days before the meeting).
Note: I could not help but notice that article ridiculed the existence of COVID-19 vaccine injuries, whereas 10 months ago (due to the costly profound loss of public trust in the medical system from the COVID vaccines), the NYT published piece which “tried to have their cake and eat it” by acknowledging COVID vaccines injuries were real, but simultaneously downplayed them and said everyone was “sorry” but no one was at fault for this debacle—illustrating just how disingenuous these people are.
•Two days before the meeting, a rogue judge (who has been reprimanded for previous similar rulings) arbitrarily ruled against the recent CDC vaccine schedule change and that everyone whom RFK Jr. put on ACIP was “not qualified” to be there and therefore, all their previous decisions were voided and the committee could no longer meet.
As court decisions (even ridiculous and unjustifiable ones) take a while to appeal, this coordinated attack effectively cancelled the upcoming ACIP meeting and prevented the vaccine injured from ever having a voice (along with blocking simple policies like having a way to actually track COVID vaccine injuries with a new diagnostic code and thereby make the injuries statistically exist). This was understandably devastating, as many of us (especially the ACIP members) put an immense amount of work (and often personal sacrifice) into improving the vaccine program as the system permitted it to be done, but then in the blink of an eye, a dishonest judge arbitrarily swept it all away.
However, if you consider the broader process at play, the wave against vaccines keeps building (e.g., previously it was never necessary to use tactics as extreme as this to protect the vaccine program), and now, there are even stronger feelings on this issue (as it mainstreams the vaccine issue within the Republican base because they’ve developed a strong resentment towards activist judges arbitrarily overturning conservative policies). For this reason, vaccines are likely to be an increasingly contentious issue that sooner or later, will culminate into a wave which is too large for anyone to suppress.
Furthermore, the unique characteristic of our era is that everything is greatly accelerated, particularly due to the widespread loss of trust increasingly brazen propaganda creates in the populace (e.g., what we witnessed throughout COVID-19), users searching for new media platforms and key platforms like 𝕏 (Twitter) allowing the rapid free diffusion of pertinent information.
That, I would argue, accounts for why we were able to so rapidly overturn the COVID vaccine program (despite every stop being pulled out to enact it), why the public opinion on vaccines in general has shifted so rapidly in the last few years, or on a more minor note, how a DMSO project by an essentially unknown author (which I never expected to go anywhere) instead was seen by millions of people, and, after 40 years, at last created a third wave of interest in that remarkable therapy.
Things like this are essentially what motivate me to try as hard as I do to make a positive contribution to the world we now live in, and how I am able to keep each setback in perspective (e.g., I never expected shifting the cultural perspective on vaccines to be easy, and while the setbacks are frustrating, I am mostly in awe of how much has already happened). I hope that this perspective can be helpful for you as well, and I sincerely thank each of you for giving me the chance to finally be able to positively shift some of the massive issues I’ve always wished but never imagined could be improved.
Author’s note: The most current information on using and procuring DMSO can be found here. Additionally, a key part of this project has been made possible by you submitting your treatment experiences with DMSO (now nearly 6,000) so we jab sort and present them. If you have had any therapeutic experiences with DMSO you would like to share, please consider doing so here.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.
If you have had a DMSO report you'd like to share, please do so here:
https://www.midwesterndoctor.com/p/the-remarkable-history-and-safety/comments
When they are posted in other places, despite my best efforts, they frequently get missed and don't make it up there.
Additionally, the most current information on using DMSO can be found in this article:
https://www.midwesterndoctor.com/p/dmso-heals-the-eyes-and-transforms
There are a lot of other DMSO articles in the cue, and in the next few weeks, they will finally start coming out now that all the source documents are completed (and just need to be sorted).
Thank you so much for your support and understanding.
Love your writings on this subject. Recently, I read one of your posts about DMSO and Povodine Iodine to remove warts. I used a q-tip with 99.95% DMSO, which was applied to the area on my finger. Once it was absorbed, I then used another q-tip to apply the 10% Povodine Iodine to the same area. I'm pleased to report after a few weeks the wart is now gone. I look forward to sharing my success with my GP as she recommended Compund W, which did not help at all.
On another DMSO subject, I'm now using it with Tea Tree Oil from NOW to help get rid of toe nail fungus. I am using the same process as above. Since this was done yesterday, it is too early to report results. I've had great success with only the Tea Trea Oil so I anticipate DMSO will only help eradicate it faster.
Thank you for all you do. I've been following you, Dr. Cole as well as Dr. McCullough since the COVID plandemic.