The Forgotten History of Carpal Tunnel Syndrome
Causes and treatments for repetitive wrist strain

One of the most frequent questions I receive is how I am able to produce the volume of content I write on Substack. In this article on RSI prevention and ergonomic typing for the millions of people who have to type far too much all day long, I will describe some of the methods I’ve used—many of which I fully admit I only adopted because I started developing carpal tunnel syndrome a few months after I started writing here and how a fortunate computer discovery long ago made much of what I now do possible.
Following this, I will describe my preferred approaches for addressing carpal tunnel syndrome (one of the most common causes of wrist pain and numbness in the fingers). I feel this topic is important to discuss because the commonly used approaches for mitigating carpal tunnel (e.g., regularly taking an anti-inflammatory like ibuprofen or injecting steroids into the carpal tunnel) often do not work, and frequently create a variety of complications, whereas a variety of far better options exist.
Note: I was inspired to write this article as I was finishing up the next article in the DMSO series I’ve spent the last month working on (which supporters of this newsletter can read in advance here).
How DMSO Heals Nerves and Eliminates Neuropathic Pain

Why a single agent, through its forgotten biophysical effects, can reverse an improbable range of "incurable" neurological conditions.
August Dvorak
When the earliest typewriters were made many different keyboard layouts were used (there was no existing standard), but they all suffered from a common issue; if you typed too quickly (specifically sequentially hitting keys next to each other) the typewriter would jam. To solve this issue, a keyboard was designed to prevent this from happening which made the sequential keys you would use be far away from each other. The typewriters with this layout gradually took over the marketplace, and before long, the QWERTY keyboard became the standard everyone utilized, even once the need for it had long since passed because typewriters that jammed had long ago gone extinct.
Note: the history of the QWERTY keyboard is commonly cited in economics as the classic example of path dependence where an inferior technology was locked in because the costs of switching it were too high. Nonetheless, almost no one to this day knows this happened.
August Dvorak was an educational psychologist and professor of education who served as an advisor for a master's thesis on typing errors. From it, he concluded that QWERTY’s prioritization of sequentially distant keyboard strokes to prevent typewriting jamming had the consequence of significantly impairing the ease and speed of typing. Dvorak then decided the QWERTY layout needed to be replaced, so he and his brother in law (another professor) spent years researching how to design a keyboard that would decrease typing errors, speed up typing, and lessen typist fatigue.
Eventually they developed a layout (in the 1930s) which emphasized having the most common letters on the home (middle) row, having frequently used keys be close to each other (so the fingers would not have to travel far for each keystroke) and having the fingers alternate between each keystroke (e.g., by having the vowels on one side and the most commonly used consonants on the other).
This for context is an illustration of the comparative keyboard layouts:
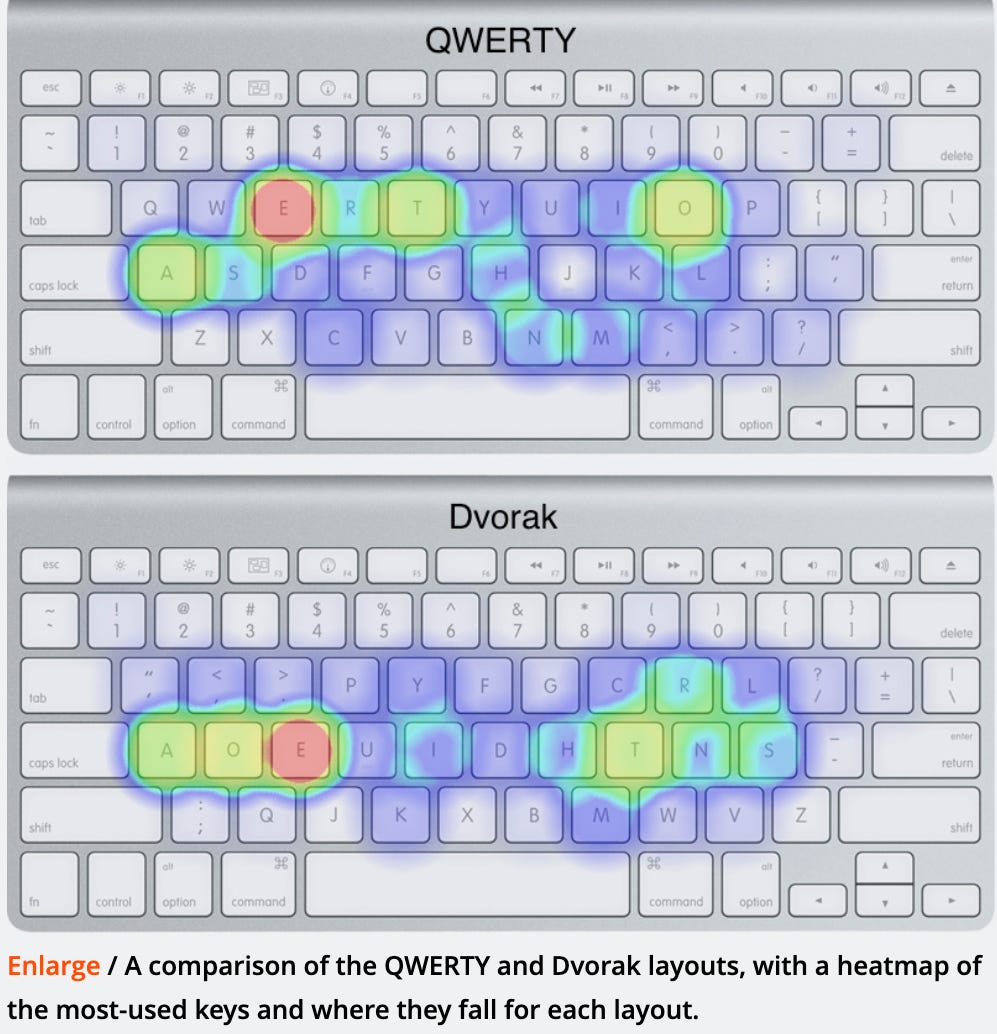
After developing the layout, a variety of studies and contests were conducted (e.g., by the US Navy) which allegedly demonstrated that the Dvorak keyboard layout was faster to learn, allowed individuals to type faster and created less repetitive strain from typing. For example, the world’s fastest typist used the Dvorak layout.
Note: To this day, I am not actually sure how much of the early research supporting adoption of the Dvorak layout actually occurred and how much of it was either fabricated or exaggerated by Dvorak proponents.
Despite many compelling reasons to have a more efficient keyboard layout, Dvorak was never adopted due to existing market pressures to stay with the standard layout everyone was already comfortable with. Eventually (at least according to the story I heard) Dvorak gave up, feeling bitter and depressed no one was interested in something he had put so much work into creating and promoting that he felt could genuinely help everyone. When I heard this, my heart went out for him, and I decided I had no excuse but to learn this layout he worked so hard to give us as I could afford to have a few weeks of impaired typing to do so.
Since that time, more advanced analytics have concluded the Dvorak is a more efficient layout to type with, but there is a bit of a debate over if that benefit is worth the hassle it takes to learn it. Since the Dvorak layout has maintained a devoted following, it has been available as an alternative language on most computer (and mobile) operating systems and numerous websites now exist to help train you in the layout. Additionally, a variety of alternative layouts like Colemak has been developed which also have a high rate of efficiency but are more similar to QWERTY and hence easier to learn (with the trade-off being the more similar to QWERTY, the less efficient they are).
Note: Dvorak layouts which change what each key on the keyboard does are built into most operating systems, so you can enable them on almost any modern computer. The best ones are the ones that switch to QWERTY when you input a command (as the commands evolved to fit the key placements on the keyboard, and, especially initially, it’s helpful to know you are hitting the right key for a command).
Once I learned the Dvorak layout, it was clear that it was much easier to type on it, and I gradually become exasperated when I had to type on QWERTY layouts as it was much slower, and importantly, much more straining. However, later in life, once medicine required me to type a lot of electronic notes (in settings where it was often quite difficult to enable Dvorak), I switched back to QWERTY and then had long periods where I would use one or the other (depending on my work situation).
At the time I started this newsletter, I had gone through a long QWERTY period and before long, began noticing, for the first time in my life, that I was developing pain with my wrists (in the carpal tunnel) so I gave myself a few tests that established it was definitely carpal tunnel syndrome. Before long, I realized I’d need to change back to Dvorak, and discovered much to my joy that external Dvorak keyboards and laptop keyboard covers in the Dvorak layout could easily be purchased online (as could stickers to place over keys). I got a cover, and since the layout was still in my distant muscle memory, I made the transition in a very short period (I believe it was a few days) and noticed a dramatic improvement in the amount of wrist strain lengthy typing sessions created.
In short, an immense amount of suffering essentially resulted from some odd historical quirks of fate that never were corrected (something that is surprisingly common).
I hence felt I needed to write this post, not only to bring attention to this, but also since the Dvorak layout played a pivotal role in making this Substack possible. Likewise it’s important to note, much of the advantage of Dvorak comes from the fact it is a mostly forgotten discovery; had Dvorak become mainstream, everyone would have been held to productivity rates it facilitated. Since it is not (and everyone instead is expected to type at the slower QWERTY rate) Dvorak offers a huge advantage to those who make use of it (although I acknowledge AI may eliminate the need for prolific typing in the not too distant future).
Note: the two times I normally use QWERTY are either when I am typing out a complex password, or when I need to write with one hand while walking and carrying a laptop (I try to make use of every available window to write). Since Dvorak is a “language” toggling between it and QWERTY is very easy in modern operating systems.
Carpal Tunnel Syndrome
Carpal tunnel syndrome is one of the more common issues patients see their doctor for that we don’t really have a good solution to (e.g., I’ve had numerous patients who had a carpal tunnel decompression surgery that ultimately didn’t help them at all).
Conventional treatments for carpal tunnel syndrome, in turn begin with nighttime wrist splinting in a neutral position to reduce nerve pressure, activity modification and ergonomic adjustments to avoid repetitive strain then progress to short-term NSAIDs for pain and inflammation, corticosteroid injections for swelling relief (both of which can create significant issues), and physical therapy, and if that doesn’t work, carpal tunnel release surgery is done (where the transverse carpal ligament is cut to open the canal).
What stands out about this progression is that each step manages symptoms or relieves pressure mechanically, yet none of them ask why the pressure built up in the canal to begin with. That question is what eventually reframed how I understood the condition.
The first thing that clued me into what was actually causing carpal tunnel was the frequency with which I would see pregnant patients who mentioned they had developed carpal tunnel during their pregnancy. One of the major changes that happens during pregnancy is that the amount of fluid retained by the body increases and there is thus a general increase in swelling throughout the body. This suggested to me that the root cause of carpal tunnel was excessive fluid within the carpal tunnel that could not drain out. As I have emphasized here, impaired fluid circulation is a key cause of many chronic conditions, and the reasons why I am such a strong advocate for approaches like restoring zeta potential or utilizing DMSO is because it frequently restores critical fluid circulation throughout the body.
Note: this is not just my own clinical impression. Topical DMSO has decades of published support for tunnel neuropathies (including formal Russian clinical guidelines for carpal tunnel), and many of the reader DMSO reports I've received for wrist issues (including those following a carpal tunnel surgery) have been remarkable.
The second thing was that all the extra time I needed to write on Substack required me to use each available window I had for writing. This frequently meant that I needed to use awful ergonomics while writing, which I fully admit I actively discourage my patients from doing. Prior to this, I had experimented with a variety of typing positions and concluded the best options were either:
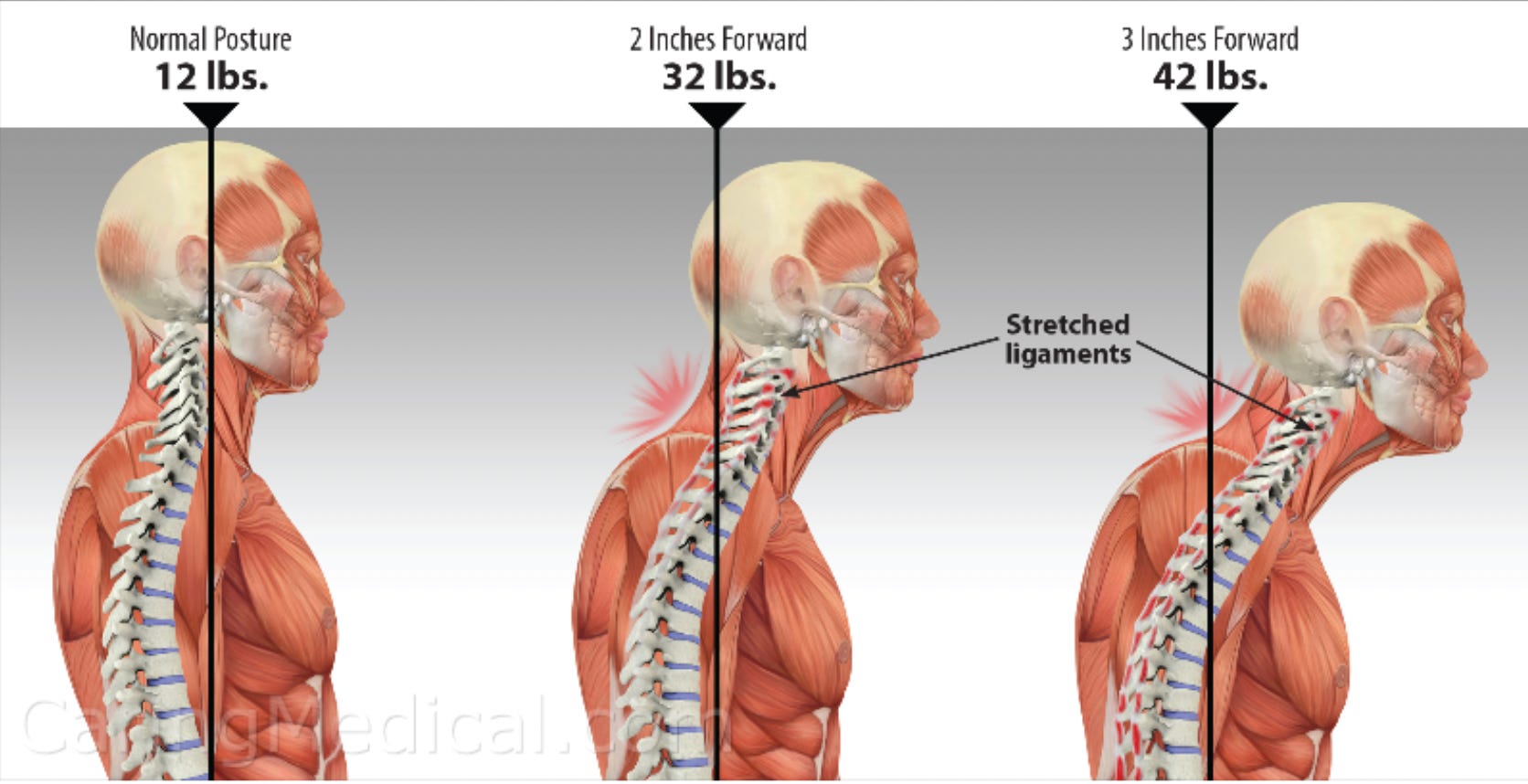
•Use some type of accessory set up which raises your monitor to the level of your head so you do not need to look down and bend your head forward (this really adds up over time).
•Using a treadmill desk (people are always selling them and used ones are fairly cheap).
Note: you need specialized treadmills designed to run at a slow speed for a prolonged period. If you repurpose an existing treadmill, you may run into issues with it.
•Use a standing desk.
•Squat (with each leg going out diagonally at approximately 45 degrees) while having a support against your back. If you find the right type of rolling office chair (e.g. one you can control the height of where the arm rests are at the correct height for your legs and the back vertically supports you), this becomes quite easy to do.
Note: Generally speaking, I think squatting is much healthier for you than sitting, and that many chronic health problems come from people sitting too much (a viewpoint that is gradually becoming more accepted by the medical profession—"sitting is the new smoking"). The setting where the ills of sitting become the most apparent occurs each time you go to the toilet (as sitting causes the puborectalis muscle to compress part of the rectum, thereby making it harder to push poop out). As a result, many find using a device like the Squatty Potty which cause them to squat when on the toilet to be very helpful for things like constipation, and there is some evidence to support this.
As I’ve gotten to know some of the other individuals who write prolifically on this platform (which requires frequently utilizing their laptop in poor ergonomic situations), I’ve discovered they also developed many of the same musculoskeletal issues I identified. For example, quite a few of them moved along this progression which causes a lot of problems as it progresses if not addressed.
There are a lot of different schools of thought on how to treat carpal tunnel syndrome, and while their proponents tend to argue their approach constitutes the correct way to treat the condition, the reality is that each is valid for some cases of carpal tunnel but not others. As a result, people often spend a lot of money seeing various people who claim they can treat the condition but then fail to do so.
Regardless of the approach you use however, one of the important things to recognize with the body mind and spirit is that it always has a threshold of stress it can tolerate, and then once that point is passed, strain and damage gradually accumulates in the body. Many problems in our society come from people not recognizing when they have passed that threshold and are overstraining their body (which I again must admit I’ve been guilty of while writing here).
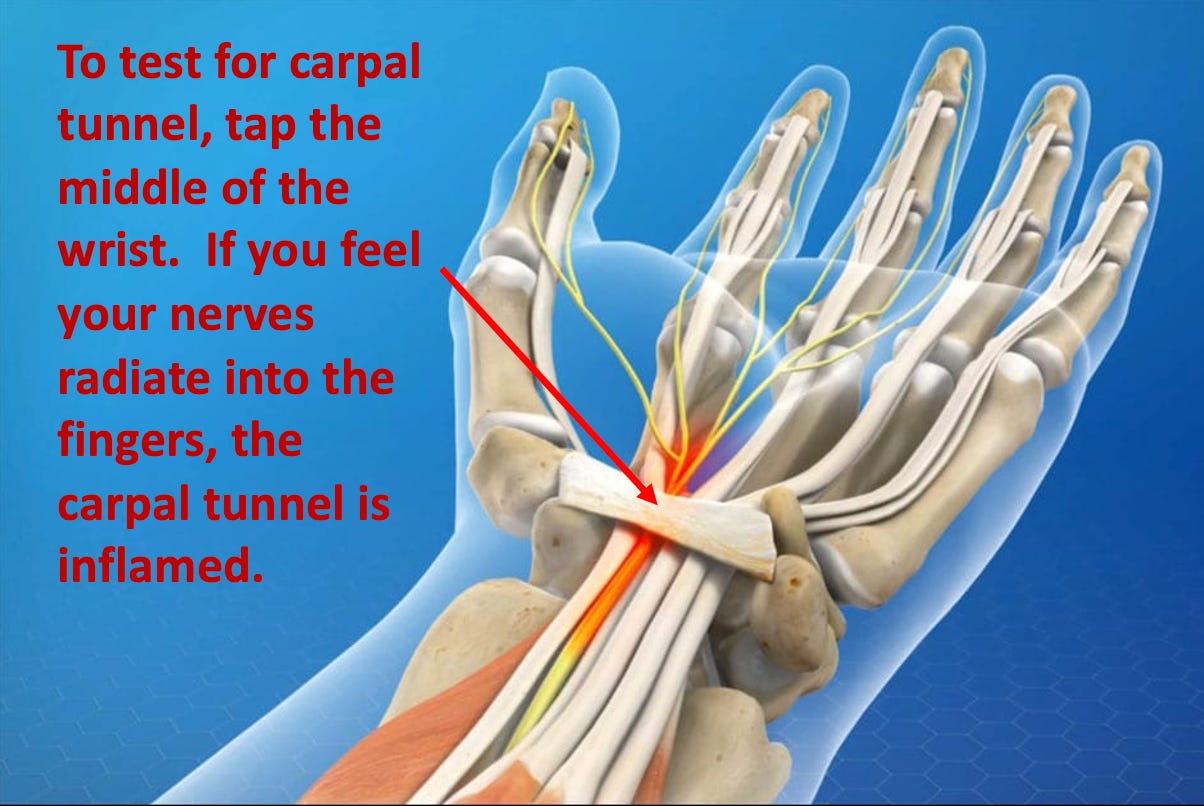
In the case of the wrists, once you start noticing they are having issues, it’s dramatically easier to fix them if you back off and give them a bit of time to recover (e.g., switching to dictation, taking a break, or doing a quick self-care approach for the carpal tunnel) rather than being forced to take a long break because they’ve gotten too sore to be able to write with. One helpful test to see how far you’ve pushed your wrists is to tap the middle of the wrist (the carpal tunnel) with a procedure known as the Tinel’s test as the nerves in it will typically go off prior to you experiencing overt pain or numbness in your fingers.
For the remainder of this article, I will discuss the approaches you can do at home that I have found to be the most helpful to address the specific consequences of poor ergonomics and poor posture that cause the body to age and no longer tolerate repetitive wrist strain that eventually leads to carpal tunnel syndrome and numbness or weakness in the hands (along with how to use DMSO for carpal tunnel—which while effective, I’ve never actually needed to do because I utilized the other approaches which addressed the root causes of carpal tunnel).
