Why the COVID-19 Vaccines Could Never Prevent Transmission
The history of "Herd Immunity" helps explain why our officials lied to us while marketing the vaccines.

Recently, the lies conducted to push the vaccines have been brought back to the public’s attention. This is partly because of the numerous videos now circulating that show just how many times a spokesman for them contradicted himself while making false promises about the vaccines to sell them to the American public on national television (which he later denied ever claiming) and partly because recent FOIA disclosers again proved our the officials who pushed the vaccines were not transparent with the public:
Emails obtained through a Freedom of Information Act request show that CDC Director Rochelle Walensky and former NIH Director Francis Collins were aware of, and discussed, “breakthrough cases” of COVID in January 2021 — right when the vaccines became widely available. In her email, Walensky says that “clearly,” it is an “important area of study,” links to a study raising the issue, and assures the person she is sending it to that Dr. Anthony Fauci is looped into these conversations.
However, in public, Walensky was saying something quite different. Two months after discussing this data, she said vaccinated people “don’t carry the virus” and “don’t get sick.” In a congressional hearing, after it became clear people were able to get infected with COVID even after receiving the vaccine, she defended her original statements by claiming it was true at the time she said it — namely, for the strands we were dealing with in early 2021.
To better understand the implications of the revelations, I believe it will be helpful to share what I directly observed occur around me and what each official stated at the time to the public.
When the COVID-19 vaccines came out, most of my colleagues drank the Kool-Aid and scrambled to be the first ones to make it to the mass vaccination site (healthcare workers got first access to the vaccine). My spouse and I were two of the only exceptions at our facility.
Later, when our administrator (also a physician) realized that we had not been vaccinated, a series of meetings were arranged to address our “vaccine hesitancy.” A few things stood out to me throughout this process:
•Numerous major errors were immediately apparent in Pfizer’s NEJM paper, but all of the physicians I worked with (who on a daily basis patronizingly reminded all of us of their competency for appraising the scientific literature), became fixated on Pfizer’s “95% effective claim” and were completely blind to the paper’s methodological shortcomings.
•At various times both of us were informed that it was immensely arrogant on our part to assume our colleagues had incorrectly appraised the evidence and that by having a differing assessment of the paper, we were suggesting that we knew better than all of them.
•Every single point we cited was subsequently proven to be true (hence why I preserved our correspondence).
Due to the politically charged nature of the topic, we tried to be as non-confrontational as possible and only critiqued the least controversial aspects of the vaccine (e.g., I was nearly certain there was massive fraud in the trials, there would be serious issues with vaccine efficacy and there would be significant autoimmune and cancer issues for the vaccinated). Since discussing the “controversial” areas could label us an “anti-vaxxers” and cast doubt on our ability to accurately appraise this paper, the most defensible areas we instead mentioned were as follows:
•The vaccine had not been tested for fertility effects in women of childbearing age.
•The reported benefits were minuscule, 119 had to be vaccinated to prevent a symptomatic case of COVID-19, e.g. a sore throat, 2711 had to be vaccinated to prevent a “severe” outcome (which of course was never clearly defined by Pfizer or Moderna), and 44,060 (split evenly between vaccine and placebo) person trial was too small to even determine how many needed to be vaccinated to prevent a single death from COVID-19. Considering that over half of the trial’s vaccine recipients experienced symptomatic side effects from vaccination, it was thus unclear if the risk-to-benefit ratio justified vaccination.
•This technology is experimental and the clinical trial is not scheduled to finish until 2023, so it will not be possible to fully assess the risks and benefits of the vaccine until then.
•The vaccine was not tested for its ability to prevent transmission, so we cannot know if patients will benefit from their doctor being vaccinated. Based on the design of the mRNA spike protein vaccines, it seemed reasonable to assume that they would not prevent transmission. I suspected testing was never conducted so that there would be no available evidence to disprove the inevitable claims that the vaccines did in fact prevent transmission.
All of these points were of course ridiculed and dismissed, but were sufficient for us to be left alone provided we agreed not to be vocal in our skepticism towards these vaccines (at this time Biden’s mandates had not yet been enacted). When I found particularly interesting about this process was that we were repeatedly told the fact that the vaccines prevent infection was proof that they would also reduce transmission. This statement illustrated a fundamental lack of understanding of immunology but was extremely common for me to encounter throughout the vaccine rollout.
It was also not helped by the fact the health authorities insisted the vaccine stopped transmission despite it being well-known the vaccines were not tested to evaluate transmission
Since that is a heavy accusation to level, I would like to cite a October 2020 article that was written in a premier medical journal and any policymaker should have been aware of:
Yet the current phase III trials are not actually set up to prove either (table 1). None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.
An understandable degree of outrage has emerged following a recent testimony from a Pfizer executive in front of the EU’s parliament that the vaccine’s ability to prevent transmission was never tested.
I would argue that while this outrage is understandable, the bigger issue is that this lack of testing was abundantly clear to the scientific community, and except for a few brave voices like Peter Doshi, this issue was swept under the rug.
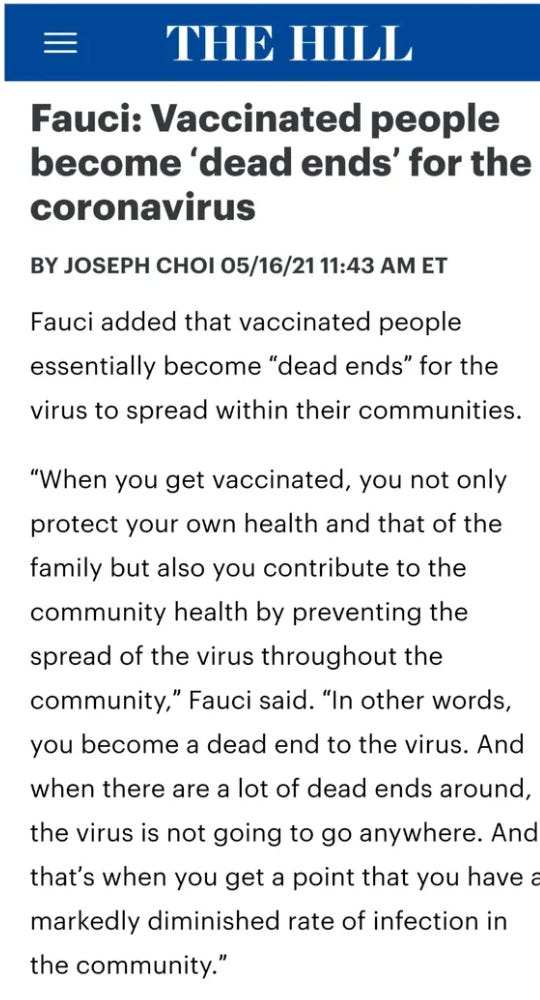
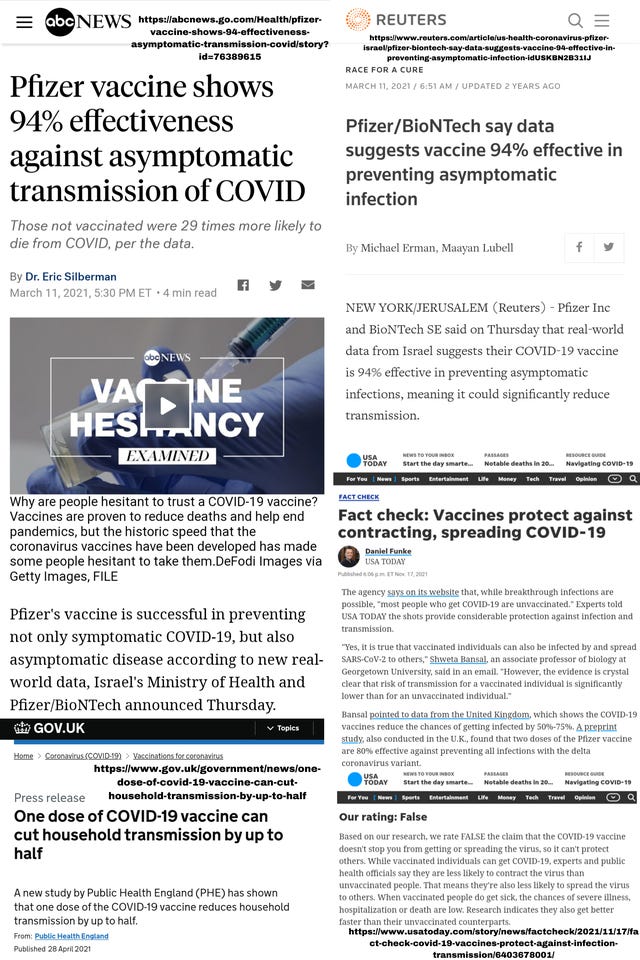
This silence from the scientific community allowed authorities around the world like Fauci (as shown above) to claim COVID-19 vaccination would prevent transmission and thus galvanize the population against anyone who was not vaccinated:

Although I believe Duran’s behavior was inappropriate, the demonization in this article really bothered me as I am well familiar with where those actions can lead to.
The media likewise adopted their mythology of vaccines being our salvation:
Anyone who was not vaccinated was treated as a leper to be avoided

Anyone who didn’t vaccinate was viewed as Grandma’s murderer (and often barred from visiting her), while children were viewed as life-threatening risk to teachers (which was used to argue for both masking of students and distance learning, both of which were disastrous for students):

Public health officials were all too eager to take advantage of this situation and stoke hatred toward the unvaccinated:

The gullible members of society in turn were all too eager to also adopt this lie:

You’ve all had to live through this and I’m sure you have examples to share that are much more egregious than the ones I have presented here. It is thus quite understandable why so many are outraged by Pfizer’s recent admission; they have a good justification to be. For example, consider this tweet:
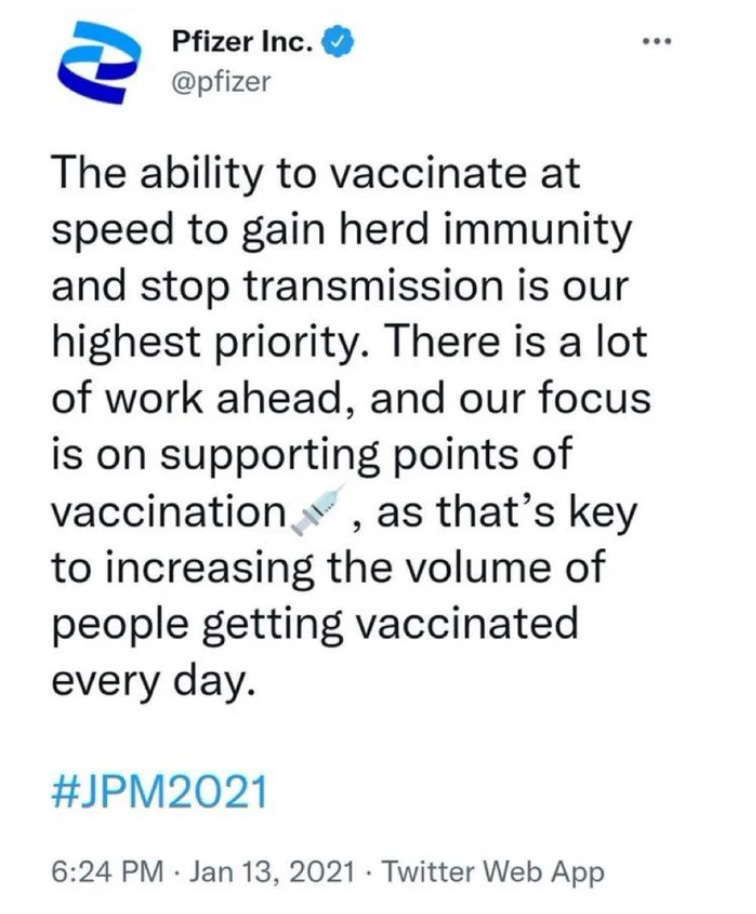
(It will be fascinating to see how this statement will eventually be justified)
However, I instead would like to propose a different way of looking at this. How do you convince the population to take a product that has clearly failed (if you are vaccinated and get ill regardless of who transmitted it to you…this means the vaccine did not work)? Furthermore, how do you convince them rather than have them acknowledge it had failed, instead get them to double down on taking more vaccines and forcing vaccination upon the unvaccinated?
In a previous article, I discussed the hierarchal structures of information control within society and argued that the same methods of propaganda are repeatedly tested out until reliable approaches are discovered. Once those methods are discovered, they are then utilized ad-nauseum.
Put differently, I was able to understand how much of the public relations (propaganda) campaign for the COVID-19 vaccines would play out because I had witnessed the exact same scams be pulled countless times in the past with other ineffective vaccinations.
Central to all these scams is the mythology of “herd immunity.”
Moving Goalposts
A common strategy in propaganda is moving goalposts, as the target ultimately being aimed for is something the public would initially never agree upon. As a result, the first thing that is pushed on the public is something that at least on the surface seems justifiable but is then gradually shifted to the originally unacceptable goal (this process is commonly analogized to the totalitarian tiptoe or slowly boiling a frog in water so it does not jump out–although the scientific accuracy of that specific claim is debated). This process is very methodical and easy to recognize once you know how to look for it.
Consider for example, as detailed previously here and here, just how quickly we have gone from each of these to the next:
•A need for Big Tech to curate information.
•Introducing the concept of “misinformation.”
•Creating the illusion of an epidemic of “misinformation.”
•Mass censorship of anything arbitrarily deemed misinformation.
•Doctors being forbidden from sharing ‘misinformation’ with their patients.
•Misinformation being declared a weapon of war by New Zealand’s prime minister at the UN.
•Governments criminalizing the dissemination of “misinformation.”
One of the most consequential examples of moving goalposts can be found in each of the recent major wars the US was involved in (Vietnam, Afghanistan, Iraq). The initial involvement was pitched as limited support (e.g. for humanitarian support), which then turned into a quagmire that only accomplished causing enormous devastation on both sides.
In each case, the American public, after years of pointless bloodshed, eventually acknowledged the wars were a mistake, and the U.S. was forced to withdraw with nothing to show for it except enriching defense contractors (a polite term for war profiteers like Biden’s Secretary of Defense). This is an important pattern to recognize because we appear to be going through the same process with Ukraine, something where our involvement with the war was initially presented as humanitarian in nature, but since that time the goal posts have been moved and moved into a much bloodier and lucrative conflict.
Note: a longer discussion on the Ukraine war and how over and over, our leaders prioritize profits rather than human beings can be found in this recent article. Additionally, Glenn Greenwald gives an excellent illustration here of how the same propaganda used to sell our previous disastrous wars is being recycled for the Ukraine war.
The military-industrial complex’s propaganda has many similarities to the medical-industrial complex’s propaganda and hence is quite valuable to study when attempting to understand what happened with COVID-19. Like wars, vaccination campaigns are always initially sold on miraculous promises those with firsthand knowledge of the data and the subject know are false. Once those promises fail to materialize, the goalposts are repeatedly moved with higher and higher rates of vaccination being demanded, lower and lower bars being set for what the vaccine will accomplish, and harsher and harsher penalties being imposed upon those who refuse vaccination. Consider for example this brilliant montage of Fauci’s statements throughout the pandemic:
Note: if this video is deleted by Youtube, it can also be found here.
As many of you noticed, the COVID-19 vaccines were initially presented as being voluntary (in fact they were initially marketed under a scarcity model with each recipient being privileged to get a vaccine), it was claimed the pandemic would soon be over with the miracles of two dose mRNA vaccines, and not a peep was ever mentioned about the potential need for boosters. The goalposts were then eventually moved to mandatory vaccinations, the vaccines only reducing your chance of dying, the virus being with us for the foreseeable future, and requiring multiple boosters each year. This reversal was entirely predictable as it followed the playbook which had been already developed with previous vaccinations.

(Note: although the last point is clearly meant to be poking fun at those who worship the vaccines, some have argued it may also be applicable and I am quite curious to see how far this meme will ultimately go).
What is particularly frustrating about this vaccination campaign was that it was known from the start the vaccines would likely fail. My biggest fear, which appears to the materialized, was that the vaccines would not only be ineffective but they would prevent the population from developing herd immunity to SARS-CoV-2. In a recent article, I attempted to summarize the pieces of evidence demonstrating this was known and deliberately concealed by the healthcare authorities (I would highly recommend it to those of you who wish to know more about the content detailed within today’s article).
Some of the key points from the above article included:
•When vaccines work (many do not), they create an evolutionary pressure on the target pathogen to no longer be covered by the vaccine. This is an extremely common process that has happened with many other vaccines and is known as serotype replacement.
•Serotype replacement can often produce more pathogenic variants of a virus or bacteria.
•Given that SARS-CoV-2 mutates rapidly and is easily transmissible, it seems unlikely serotype replacement would not occur.
•SARS-CoV-2 evolving immunity to the vaccine could have potentially been avoided by designing vaccines with multiple antigens on them in regions of the virus that did not mutate rapidly. Instead, the vaccine only used a single antigen, a rapidly mutating (and cytotoxic) part of the virus, the spike protein.
•Vaccines, that do not produce sterilizing immunity produce variants and cannot prevent transmission. The spike protein vaccines were designed to reduce symptoms, not to reduce transmission.
•All of the above argues that the vaccines may have been intentionally designed to fail so that perpetual boosters could be sold to the public.
As the argument for a vaccination campaign weakens because the vaccine repeatedly fails to prevent illness while causing many concerning side effects, to sustain the vaccination campaign, mandates must gradually be enacted. Typically, to justify a mandate, it must be argued that the unvaccinated individual is not just hurting themselves but is hurting others and thereby meets the threshold for losing their personal liberties. To do so, we rely upon the construct of “herd immunity,“ which like many other things in the mythology of vaccination, is based on false premises that inevitably fail and hence require continually moving the goalposts.
Modeling
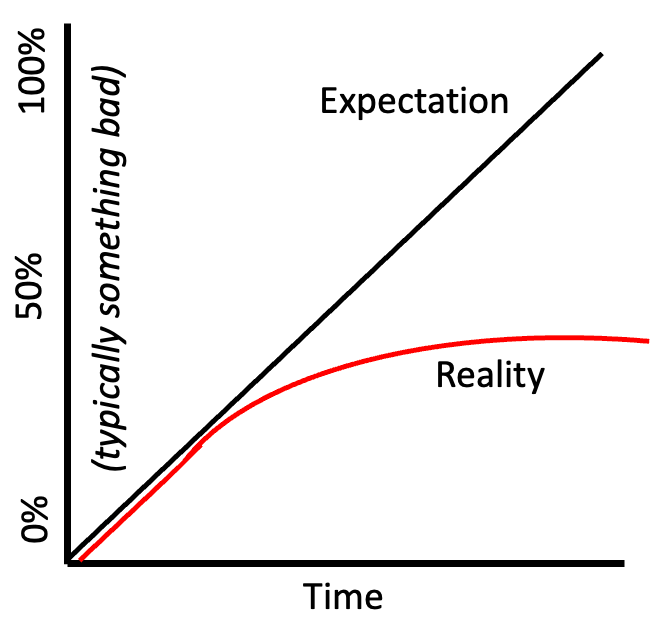
One of the foundational beliefs of our religion of science is that everything in the universe can be broken down into mathematical equations. In many cases, this is completely true. However, with more complex natural systems, especially those involving sentient organisms, those models often fail to hold up (e.g. consider this collection of climate models that were later proven to be false). Unfortunately, due to the faith we hold in the scientific” paradigm, when bad mathematical models are put forward, they are rarely if ever questioned. The below graph demonstrates what I have observed with more models or projections than I can count now:
A recent memorable example were the projected vaccination rates in the United States compared to what actually happened
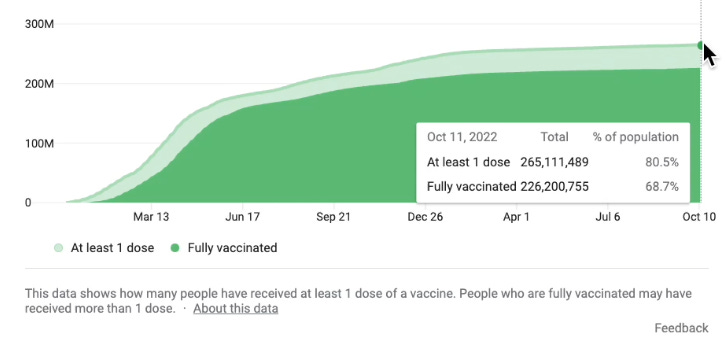
Note: presently 81.4% of the US population has received at least one dose of the COVID-19 vaccine.
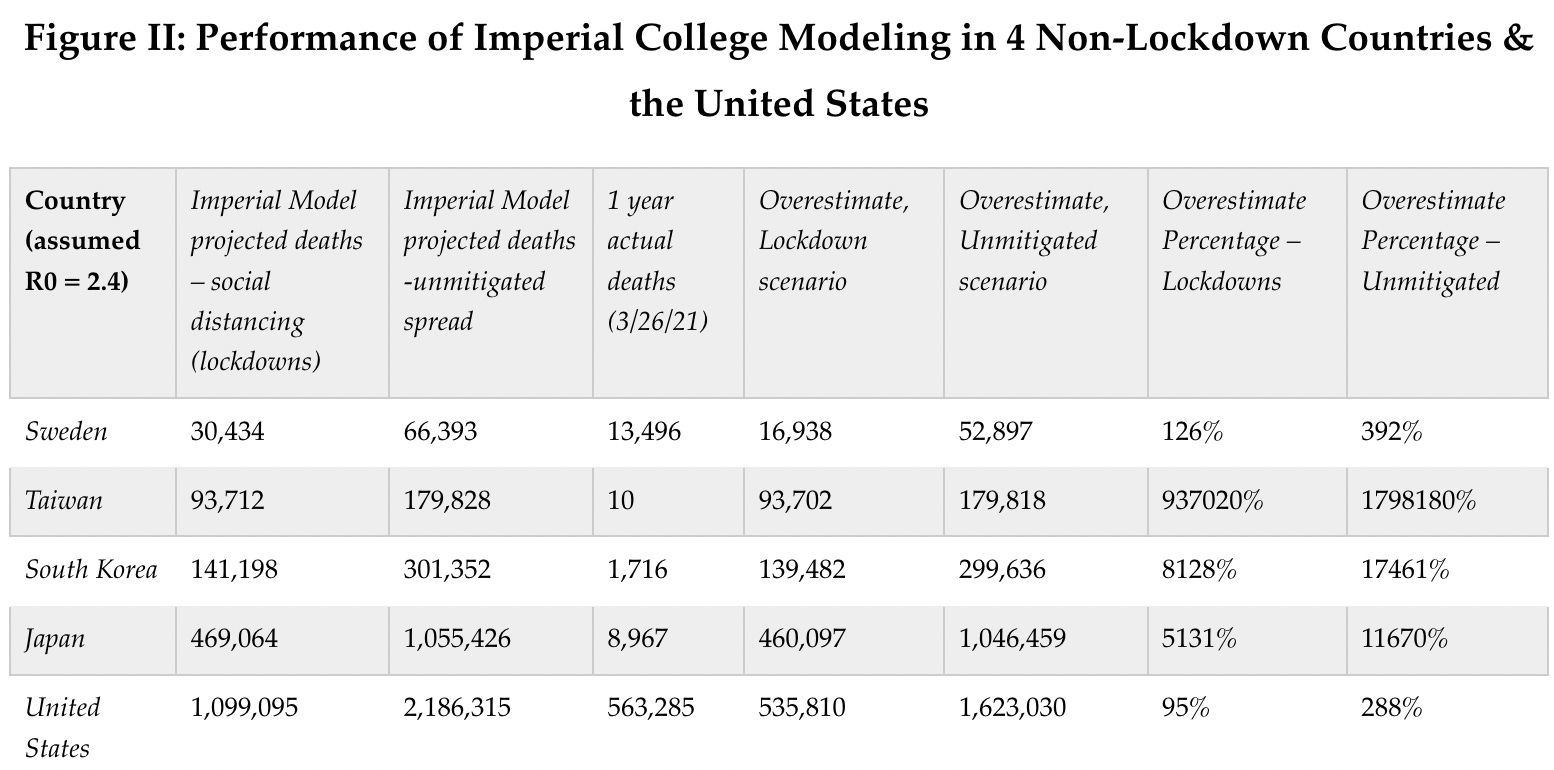
The modeling problem was most evident with the dire models that were used to justify mass lockdowns. The modelers, who had previously made wildly inaccurate models that greatly overstated the death rate from various infectious diseases, produced a model for COVID-19 that predicted a global catastrophe if strict lockdowns were not immediately implemented. When policymakers were presented with these catastrophic models, they of course felt duty-bound to impose these lockdowns and viewed their potential consequences as a necessary sacrifice.
There were however three problems:
•Lockdowns were nonsensical because at best, all they could accomplish was delaying the spread of the disease as individuals would eventually have to leave their homes.
•The modelers did not consider the social and economic consequences of their models.
•The models utilized a variety of flawed assumptions that would not have withstood any degree of independence scrutiny had they been subject to peer review. Furthermore, the chief modeler had repeatedly made extreme overestimations of the severity of previous infectious diseases, but nonetheless his models were never questioned.
To illustrate how inaccurate these models were:
Many other bad models are perpetuated indefinitely in medicine. One of my favorite “bad models” is the ASCVD calculator which was rolled out in 2013 by the American Heart Association and was eagerly adopted by my colleagues (it has a few easy to obtain numbers you can punch in to “scientifically” calculate how likely someone will be to have a heart attack or stroke in the next 10 years. Those with a score of at least 5% were “encouraged” to take a statin, while those with at least a 7.5% risk were “advised” to start a statin.
Most of my colleagues gleefully adopted this calculator (as did the medical board examinations and the guidelines each physician is expected to follow). At this point, I have lost track of how many times numbers were authoritatively pushed into the calculator in front of a patient after which the patient was gently, firmly, and then if still not agreeing to, hysterically lectured on their urgent need to start taking a statin regardless of the side effects of the drug.
I was always suspicious of this model as I knew statins provided minimal benefit in preventing these conditions (but were excellent at creating life altering side effects and enriching the statin manufacturers). It was also not hard for me to notice they tended to calculate a risk which almost always passed the statin threshold. Later, I learned of a 2016 Kaiser study had looked at the electronic health care data of 307,591 Americans and discovered that the calculator was overestimating the risk of a heart attack or stroke by between 5 to 6 times! Nonetheless, it is still being used.
As you might suspect, this exact same problem has also occurred for decades with modeling herd immunity, and like many other models, the modelers have never been required to defend their models or held to be accountable for their models’ failures.
The History of Herd Immunity
Throughout my lifetime, I have repeatedly witnessed the proposed herd immunity threshold be raised again and again, and simultaneously noticed most people don’t seem to notice this trend as they believe each projection presented to them. Fortunately, to some degree this is acknowledged by the epidemiological community (the following is a paraphrased quotation from Wikipedia with my commentary in brackets):
The term "herd immunity" was first used in 1894 by a veterinary scientist and USDA official to quantify the vitality and disease resistance of well-fed herds of pigs. In 1916, USDA veterinary scientists used the term to refer to the immunity after infection in cattle infected with brucellosis. By the end of the 1920s the concept was used extensively - particularly among British scientists - to describe the build-up of immunity in populations to diseases such as diphtheria, scarlet fever, and influenza.
Herd immunity became widely recognized in the 1930s following research on the epidemiology of measles in Baltimore after it was noticed children developing immunity to measles temporarily decreased new infections. Because methods of the time (1930s-1950s), in conjunction with natural immunity, failed to end measles outbreaks until a measles vaccine became available in the 1960s, it was concluded that herd immunity, in general, required vaccination [rather than this only applying to measels].
Following vaccination being associated with herd immunity, the term entered widespread use [presumably because of the money that could be made from it], and became dogma after being [erroneously associated] with the elimination of smallpox.
In the 1970s, the theorem used to calculate a disease's herd immunity threshold was developed
Since the adoption of mass vaccination and ring vaccination, complexities and challenges to herd immunity have arisen. Modeling of the spread of infectious disease originally made a number of assumptions, namely that entire populations are susceptible and well-mixed, which is not the case in reality, so more precise equations have been developed.
In recent decades, it has been recognized that the dominant strain of a microorganism in circulation may change due to herd immunity, either because of herd immunity acting as an evolutionary pressure or because herd immunity against one strain allowed another already-existing strain to spread. Emerging or ongoing fears and controversies about vaccination have reduced or eliminated herd immunity in certain communities, allowing preventable diseases to persist in or return to these communities [this sentence’s logic creates an unfalsifiable belief system that will always favor vaccination].
I and many others view herd immunity as a marketing gimmick used to justify higher and higher vaccination sales (e.g. the mythical 95% childhood vaccination rate California mandates across the state) because many of the premises its models rely upon are flawed (e.g. vaccine immunity lasts for a few years not a lifetime, and most of the adult population is not vaccinated). While some vaccination campaigns within limited circumstances have been shown to reduce the prevalence of a disease in a community (this will be discussed in the second part of this series), vaccination rates frequently have no correlation to the prevalence of epidemics they are supposed to prevent (e.g. in 1985, when most of the vaccines we now use were not on the market, there were not widespread outbreaks of those diseases). As this article aptly states:

In the case of COVID-19, herd immunity thresholds were initially presented as being between 60-70%, but now have risen to over 90% and it is gradually being acknowledged that achieving herd immunity is impossible.
One of the best examples I have seen of this can be observed by contrasting South Africa (35% vaccinated, 5% boosted) with Portugal (95% vaccinated, 70% boosted). Initially, their rates of infections and death from COVID-19 were similar, but once the vaccines were introduced, infections and deaths became much more common in Portugal, while South Africa (which has many severe health care challenges) effectively developed herd immunity to COVID-19 (other African countries that did not vaccinate have also fared well).
Negative Vaccine Efficacy
As the example above illustrates, a concerning phenomenon has been repeatedly observed: being vaccinated makes one more likely to catch COVID-19.
I have long suspected this is the case as I have observed certain vaccines appear to increase the likelihood of a severe illness and I have seen countless pieces of evidence suggesting this was the case (e.g. smallpox vaccination campaigns repeatedly resulting in larger smallpox outbreaks than those that which proceeded the campaign or those in neighboring cities that were not vaccinated). Since that time I discovered that many other studies have reached the same conclusion (e.g. through a concept known as virus interference, receiving an influenza vaccination greatly increases your risk of developing a variety of other viral respiratory infections).
In the case of COVID-19, vaccine efficacy appeared to drop from the time of vaccination until it becomes negative. This later clearly demonstrated by the Cleveland Clinic's study of 51011 people):
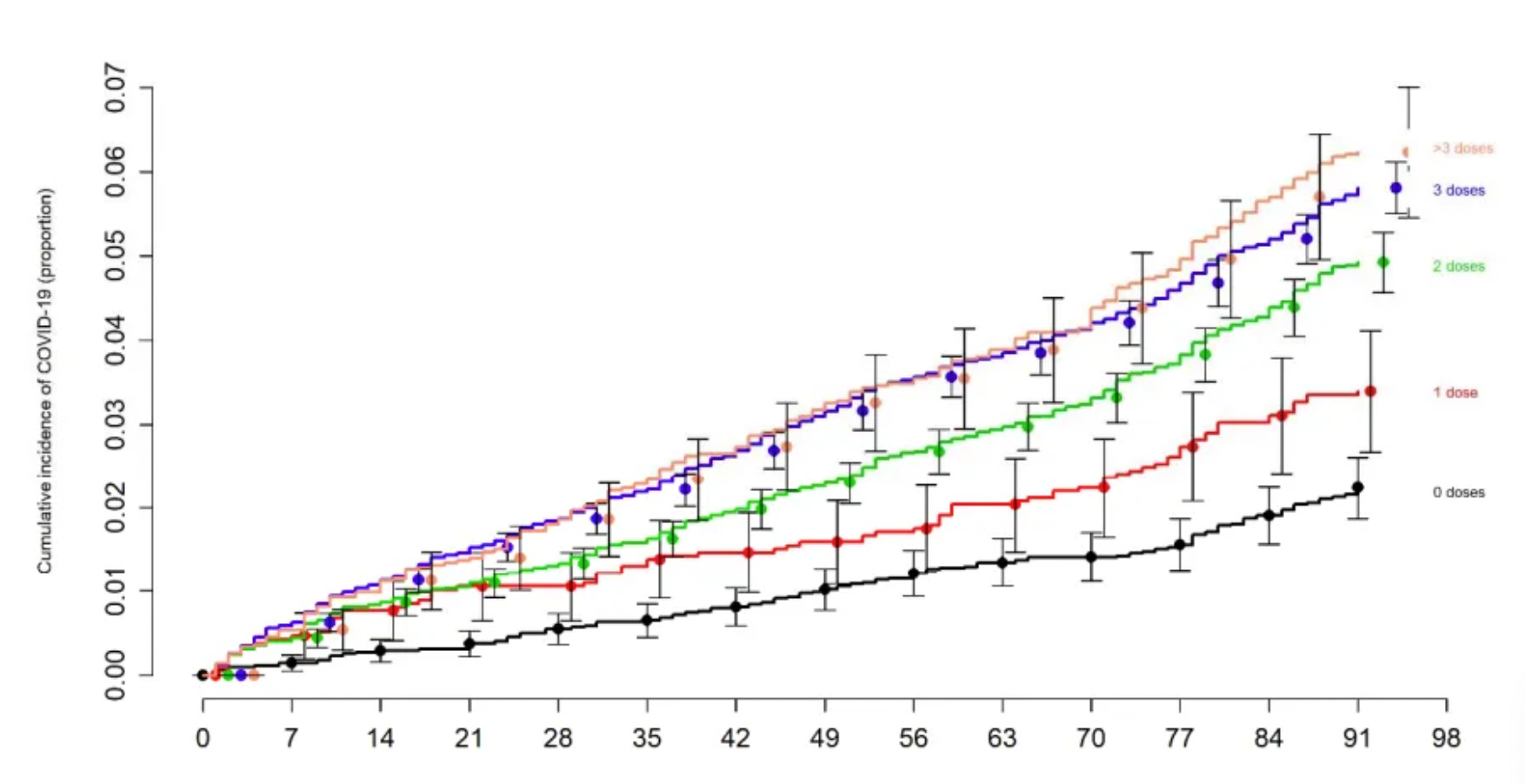
The solution to this problem has been to repeatedly deploy boosters before the vaccine efficacy can become negative. Further complicating the issue, as best as I can tell from reviewing the preliminary evidence, the rate of decline in vaccine efficacy appears to accelerate with each successive vaccination (while the rates of severe adverse reactions simultaneously increase).
A phrase I have commonly heard mentioned is that the definition of fanaticism is one realizing they are going in the wrong direction, and then instead of slowing down or turning around, they double their speed (another description for this phenomenon is choosing to double-down rather than admit that one is wrong). Our society seems to reward this behavior, so it persists (the previously mentioned wars for example provide numerous tragic examples).
I can thus understand why vaccine advocates are choosing to promote more and more boosters rather than acknowledging that vaccination may not be the solution to COVID-19. I view this as a product of public health training conditioning each student to believe the solution to every problem in the world is more vaccinations, which results, quite literally with many of them being kept up at night in turmoil over the minute percentage of the population who refuse to vaccinate and prevent all of our problems from going away.
Nonetheless, it still surprises me that they don't seem to get that there is no possible way a vaccine with negative vaccine efficacy could ever create herd immunity. Like many other things in life, that is the power of ideology.
Conclusion:
In most cases, I vehemently disagree with the fact-checkers. Curiously, today I found myself in agreement with Politifact on this issue.
To quote their rationale:
But the notion that Pfizer "admitted" it didn’t test its vaccine for its ability to stop transmission is incorrect.
Andrew Widger, a spokesperson for Pfizer, said in a statement that details of its phase 3 clinical trial have been online since 2020, and that the trial was never intended to study transmission.
This line of reasoning however does put Politifact in a bit of a bind and I am quite interested to see how this Ministry of Truth addresses that problem:
(Note: The Ministry of Truth is in reference to the main character of 1984’s job being to continually edit old news stories so that the ruling party was never wrong regardless of their past errors, a trait Peter Hotez has recently brought widespread public attention to).
The most unfortunate part of all of this is that the failure of vaccines to prevent disease transmission (or to create asymptomatic carriers) has been observed with many other vaccinations and there are numerous studies showing where this happens and more importantly how it happens.
In the second half of this series, I discuss these studies as they provided many valuable lessons in immunology that should have been considered prior to choosing to adopt a spike protein synthesizing vaccine that was only designed to reduce symptoms of COVID-19. Although technical, I believe these studies are critical to share because they highlight the profound lack of knowledge within the medical field towards the science of vaccination.
When the "vaccine" was mandated at my hospital, the requirement spiel sent by email stated a few things:
-The vaccine prevents asymptomatic transmission, thereby protecting unvaccinated patients/visitors and those not yet eligible for the vaccine (young children) or those with compromised immune systems.
-It's nearly 100% effective against severe disease, hospitalization and death. It offers protection against circulating viral variants.
-Safe and effective for pregnant women.
-There are only rare adverse effects including anaphylaxis and one in 7 million thrombocytopenic syndrome.
-It prevents development of chronic covid-19 symptoms (long covid).
I knew this was a crock of shit at the time as I already knew multiple people who still got sick who got the jabs, plus one coworker with arrhythmias, one with a swollen lymph node the size of a golfball, and one who developed severe POTS and was unable to return to work. There was also a study out of Wisconsin right before the mandate occurred that was showing "breakthrough" cases and high viral loads in the vaccinated. It really was surreal watching the rest of the world pretend as if these injections made you bulletproof for the next 2 years, going so far as to segregate society and ban people from public places. I'd like to do away with this phony belief that injecting chemicals into your arm makes you resistant to disease.
Seeing all these "experts" commenting, all the new article headlines, etc.. reminds me of how bad it was. It was/is infuriating. I lost friends b/c I wouldn't vaccinate. I called colleagues who I had taken TWO graduate immunology courses with, asking WHY should I vaccinate for something for which I had a high antibody titer (paid for myself) ....crickets....just do it....its a good idea.... yeah right! Tell that to the many, many people I know with fast moving cancers, autoimmune disorders....oh yeah - and the ones that died from heart attacks (all under 50)
I was forced to take a humiliating spit test every week for a YEAR b/c I refused to submit. In front of a "monitor", like a common criminal.....or I would be put on leave without pay - NOT BE ABLE TO FEED MY CHILDREN. And I know many, many people treated worse. Disgusting!
I don't say this lightly - these people are all evil. They are the Germans, walking around aimlessly, circa 1949ish, living with the shame and knowledge of what they allowed to happen to their country....pretending and wishing they could hide and go back to "normal".
I have never trusted gov't, but now I rank the medical community right there with them. Stay away from doctors and hospitals as much as you can. They ( with a few exceptions) have all violated their oath. We don't even live in the same country anymore.