How Corruption Dictates the Practice of Medicine
Who Actually Decides What Medicines We Are Allowed To Have?

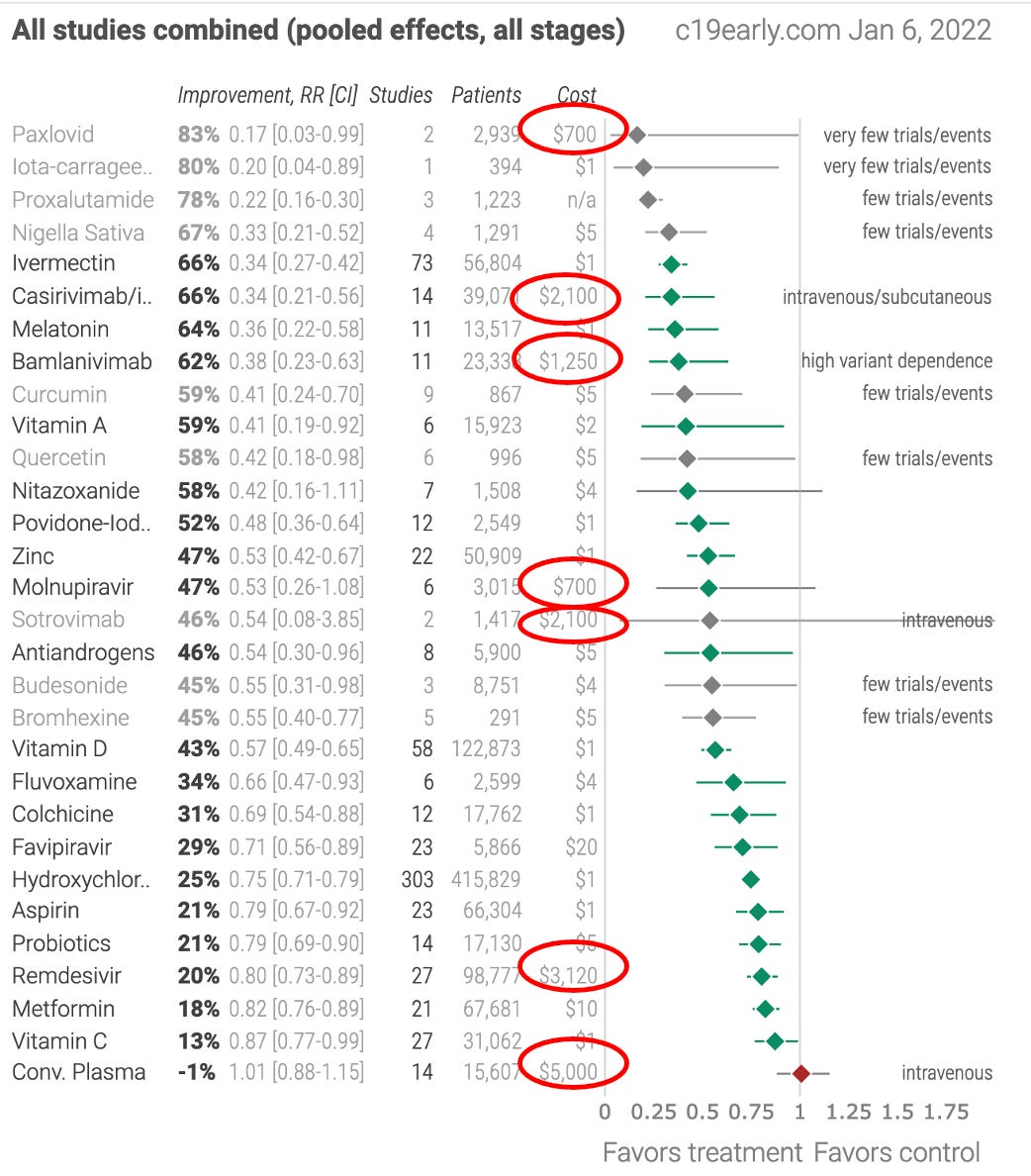
Steve Kirsch recently wrote an excellent article highlighting three “scientists” whose guideline recommendations were ultimately responsible for the deaths of nearly a million Americans. To summarize: It shows that there are dozens of treatments for COVID-19 that have numerous peer reviewed studies demonstrating their efficacy. Despite those existing therapeutics and countless petitions for their usage, the committee responsible for developing the guidelines on what is an appropriate treatment for COVID-19 has only approved remdesivir, which is a toxic drug with no therapeutic value for treating COVID-19. As a result, a dangerous drug has been mandated, while many drugs that would save lives are prohibited in most medical systems.
Evidence based medicine is commonly thought to mean “the best evidence” dictates the standard of care. In reality, it typically means financial interests dictate the standard of care and “evidence” is just used as a smokescreen to justify profiteering. This table that I initially discovered from Kirsch’s article provides clear and unambiguous proof of that contention. See if you can figure out what the circled drugs (those which received an EUA) all have in common!
Because I expected the conflicts of interests of the committee that determined the COVID-19 treatment guidelines to follow the typical pattern, I did some digging and discovered a lovely web of corruption that entangled many of its members. The purpose of this article is to explain the typical pattern and illustrate how it was followed in this case. I am doing this because I believe the first step to moving beyond that pattern is to recognize its existence. For those of you who do not need the context, please skip ahead to the COVID-19 Treatment Guidelines section.
Introduction
There are two ways you can observe most organizational systems:
•As someone trapped inside the system observing their surroundings.
•As an outside observer who sees the entire system as a whole.
Since we typically do not explore or examine systems that are outside our everyday lives, we will typically experience the first type of observation. This occurs after life circumstances force us to become stuck in a system, which happened to many of us who were swept into the maelstrom of COVID-19.
Two of my central principles for understanding the architecture of modern society have been the relentless creation of hierarchal systems and the monopolization of resources that are essential for life.
In regard to the first principle, no matter where you look, a typical pattern is always followed: a hierarchy is established, significant investment is created to establish the importance of the hierarchy, and the top of the hierarchal pyramid is bought out (often through bribes) so that a small investment at the top can be leveraged to control an entire population.
In regard to the second, those with obscene fortunes seem to always find ways to monopolize resources essential for life and transform them from something each person can independently produce to something they must continually work to obtain. For example, it is extremely common after communist revolutions that the independent farmers in the nation will either be prohibited from farming or executed, allowing agriculture to be transitioned to a state-run enterprise. Once this happens, everyone is forced to work for the state or starve, which leads them to becoming obedient subjects that can be easily exploited for their labor.
In most cases when the monopolization of a life essential resource occurs, the new approach is hailed as a technological miracle and this is used to encourage people to let go of their traditional and self-sufficient approach. The new “miraculous” approach is initially deemed “superior” but before long turns out to be worse than the now abandoned initial approach.
The Green revolution is an excellent example of this (more and more fertilizers herbicides and pesticides are needed to produce the same agricultural input). For example, Bill Gates, under the guise of “charity,” has frequently made people in Africa abandon their traditional self-sufficient forms of agriculture and switch to modern chemical-intensive industrial agriculture. Before long, this spikes their price of food and farming supplies (which must be purchased from a multinational corporation like Monsanto). As we are now hitting an unprecedented global wave of fertilizer and food inflation, it is likely that millions who were coaxed into abandoning their traditional forms of agriculture will starve to death.
I have similar reservations about our current transition to green energy technologies. I know of numerous proven effective technologies that could lessen the environmental impact of our energy consumption. However, none of the technologies currently being evaluated meet this fundamental criteria. Instead, each one further centralizes control over this life essential resource, and in the future will likely be used to significantly limit unauthorized consumption of energy or transportation once our existing fossil fuel infrastructure is displaced. For example in light of recent political developments, concerns have begun to be raised over the switches existing in electric cars that can turn them off remotely.
Medical Inflation
Those two principles (rigid hierarchal organization and monopolization of a life essential resource) also happened with the medical industry and really kicked into gear when the Rockefellers (and to some extent Carnegie) bought the AMA and invested a great deal of money into standard medicine (often called “allopathic” or “biomedical” medicine). A variety of competing schools of medicine were removed from the United States, and the practice of medicine was monopolized (those curious to learn more can find more details in this freely available classic).
This proved to be an excellent investment and the effect of this monopolization is striking:
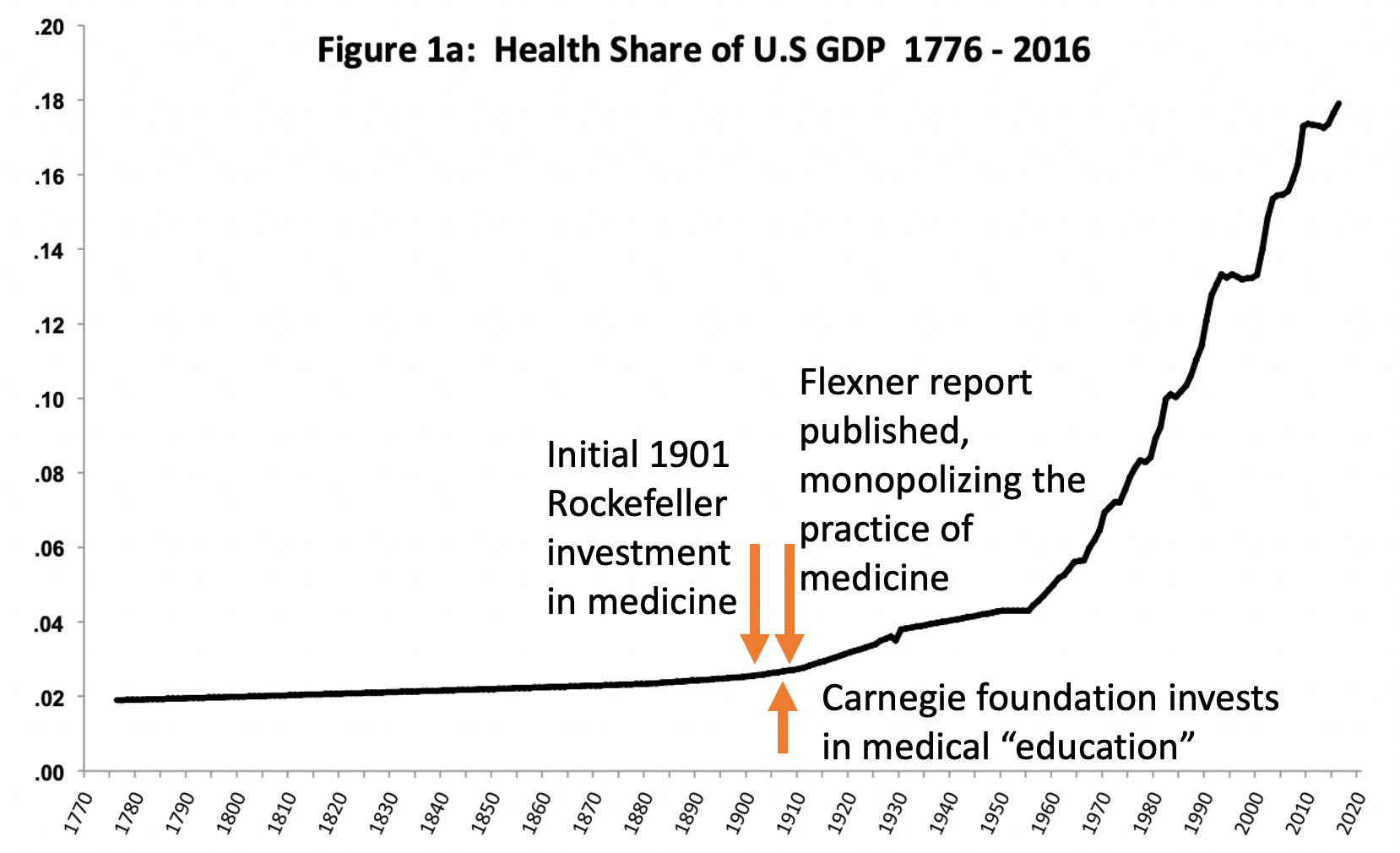
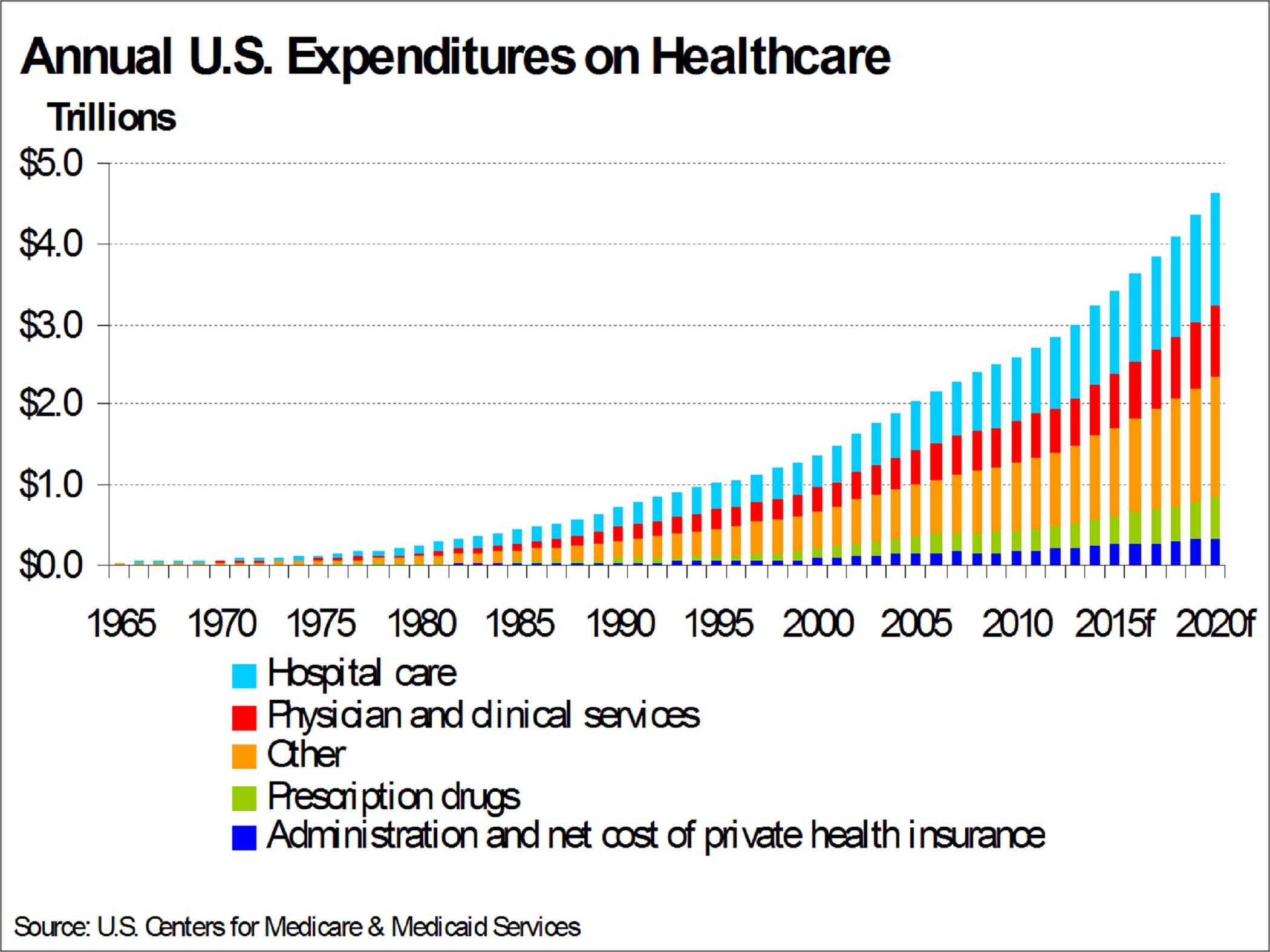
Numerous changes in society emerged to support this medical paradigm. Some of the most important were as follows:
•Society was conditioned to believe that they needed a doctor to be healthy, rather than health being viewed as something each individuals was empowered to seek for themselves. This effectively created an unlimited demand for medical services, and as the above graphs show, an ever-growing need for medical spending. Medical Nemesis by Ivan Illich was the earliest work I was able to locate detailing this change and its consequences.
•Things that genuinely improve public health (and thereby reduce medical expenses) are typically not allowed to emerge, while pointless initiatives that do not improve public health (water fluoridation or annual flu shots) are continually promoted. Likewise, basic health education is not taught to most people, and instead health behaviors developed by corporate interests constitute the majority of “health education” (industry funded nutrition textbooks for example are very common in college courses). In short, there are dozens of simple and obvious policy changes that many have independently identified which could rapidly improve public health and save a lot of money, but despite decades of campaigning to enact them, most have never been adopted.
•Hundreds (or possibly thousands) of highly effective medical treatments for common diseases have been kept off the market to preserve the market for expensive but ineffective treatments that often require lifelong purchasing. For example, prior to the legislative battle to legalize acupuncture, I remember cases where Chinese immigrants were raided at gunpoint for practicing acupuncture in their own community without a license. For those interested, I’ve spent decades tracking those “forgotten cures” down, and while I have found many that for one reason or another were oversold and didn’t really work, I also found many others that were highly effective.
•Every medical service or product is designed to encouraged the consumption of more medical services or products.
•A rigid hierarchy was created to support this monopoly.
Medical Hierarchies
The first hierarchy relates to the right to practice medicine. A large debate exists over whether or not a license should be required to practice medicine. The trade-off is that if no license is required, unqualified practitioners who might harm the public are allowed to practice, while if a license is required, the practice of medicine is monopolized (making medicine much more expensive) and medical practitioners are unable to provide life saving medicines they believe in.
I will now examine a few levels of this hierarchy:
•Medical boards have the power to pull the licenses (and hence careers) of any physician who does something “bad.” Unfortunately, since medical board members are directly appointed by governors, they often end up with crooked and corrupt members (one colleague who served on a midwestern medical board attested to this). Some of the reasons why medical boards exercise their authority are definitely valid, but many others are done to target physicians who step outside the line of what prevailing interests want done. This has happened for a long time. Here are a few examples:
1. After SB 276 was signed in 2019, writing vaccine exemptions was for all practical purposes outlawed in California and I heard of numerous cases where doctors wrote a single justified exemption and then had their license terminated. For this reason, doctors in California will not even write exemptions for patients who nearly died from their first COVID-19 vaccine (ie. from anaphylaxis or a heart attack).
2. The federation of state medical boards put out a statement that publicly promoting any type of COVID “misinformation" (ie. mask efficacy, early treatment options, vaccine safety concerns) could be used to take away a physician’s license.
3. Physicians have had their license suspended for using early treatment options that have FDA approval for other conditions.
The experiences of Robert Malone’s colleague Meryl J. Nass MD is a well known example of the above, but there are many others as well.
As you might imagine, it is quite easy for corporate interests to influence the composition of medical boards (as they are composed of individuals appointed by the governor). In the late 1990s the opioid manufacturers concocted the idea of having present levels of pain be the 5th vital sign and hence measured at every visit.
Since their opioids had “no addictive potential” once this epidemic of “unrecognized” pain emerged (since everyone was encouraged to say they were in pain) the manufacturers managed to lobby the medical boards into taking the position that failing to treat pain with an opioid as malpractice. Once that happened, to protect their licenses, any physicians who had hesitations providing opioids to patients started giving out opioids like candy and this created the current opioid epidemic which has been beyond devastating for many poorer regions of the USA. The problem is massive; hundreds of thousands of people have died from drug overdoses since COVID (which is a figure comparable to the death count from COVID).
•It is very difficult for physicians to work privately in independent practice (a variety of factors have been put in place to force this change over the last 10-20 years). Instead they are required to work at corporate, federal or state jobs where they are largely at the mercy of the institution they work for to follow its policies.
It is for this reason that as soon I was able to, I stopped working for an institution that controlled my practice of medicine.
During the pandemic, many physicians who had serious concerns about the existing approach towards COVID-19 attempted to do things differently, and were frequently shut down by their institution. This led to physicians being fired for not telling their patients the vaccine was “safe and effective” and others such as Paul Marik MD having to sue their hospital in order to be permitted to prescribe a treatment they felt could save the lives of their patients (where no effective treatment was currently available and the patients were frequently expected to die otherwise). Trump’s “Right to Try” law was meant to address this issue, but corporate management has largely superseded it.
•Everyone in medicine is taught to defer to the judgement of a doctor. Hence if you want to do some type of medical treatment and the doctor does not “approve” it, you can’t. In nursing textbooks, it is repeatedly hammered in to always defer to a doctor’s judgement. Nurses typically spend significantly more time with patients where they can see and in their hearts question the human cost of an enforced medical regimen. In contrast, physicians (the ones with authority over the patient), due to their time constraints, typically spend very little time with their patients and are much more detached and isolated from them. This results in bypassing the human connection that should be necessary in medical decision making being bypassed. This type of organizational structure has been used in numerous inhumane systems in the past.
Similarly, many individuals who have found their loved ones in the hospital have been told that unless the supervising doctor approves it, they cannot have any other type of therapy administered. Since many hospitals would not change their policy, numerous lawsuits have been filed to permit patients expected to die to receive ivermectin for example. To my knowledge, in each case where the lawsuit ordered ivermectin to be administered, the drug then saved the patient’s life.
To further illustrate this hierarchy, I know a few physicians with active medical licenses who were hospitalized for COVID-19. Each told me during their hospital stay their that care was continually mismanaged, they had to constantly be on the alert for a fatal medical error, and many of their reasonable requests were not approved by the doctor supervising their hospital care.
•Medical schools to a large extent select for individuals who do not challenge the system, and once in medical school, they rigidly target anyone who is not compliant and obedient to the existing hierarchy to ensure that they will not graduate.
The medical education process is extremely difficult (you have to work brutal hours which break a certain number of medical students and resident physicians each year, and suicide is quite common) and many aspects of the education could be equated to a form of hazing. These types of experiences are known to produce subservience to a system and have been utilized in many fields besides medicine throughout history.
Finally, there is a massive financial cost to become a doctor (most physicians now graduate with between $200,000 to $400,000 of debt at ~7% interest) which leaves many doctors who want to do things differently being completely unable to challenge this system.
The second hierarchy is “medical evidence.” When evidence based medicine was initially introduced, it was a very good and needed paradigm. Many horrific and harmful practices were in wide usage that evidence based medicine had relegated to the dustbins of history. However, medical evidence also follows a hierarchy which rejects foreign or competing ideas, and the upper levels of this hierarchy is bought out by pharmaceutical interests. Here are some examples:
•In order for a study to “matter,” it has to be published in a prestigious journal. The problem is that with the occasional exception of the British Medical Journal, none of the prestigious journals will ever publish studies which go against the existing narrative. “Controversial” studies that merit publication are continually rejected, while bad studies that support mainstream views are regularly published.
One of the better-known recent examples involved The Lancet publishing a study showing hydroxychloroquine was unsafe and ineffective, which was used to end trials of HCQ globally. This study used blatantly fake data and was eventually retracted after readers complained.
The Journal of the American Medical Association appears to be the most biased publication in this regard, and in most cases you can predict what an entire article will say on a topic before you even read it (ie. does the COVID vaccine have any possible harm associated with it…no). The one interesting exception I have seen to this was a recently published study debunking the use of ivermectin. Here the conclusion of the article argued against the use of ivermectin, while the actual data argued for it, raising the possibility the authors phrased the conclusion to say the opposite of their results so that JAMA would publish the study (it is very common for conclusions in journal articles to not be representative of their results).
•In order for a study to be published in most journals, it has to pass “peer review.” In most cases, peer review will hold ideas challenging the existing narrative to either a high standard or an impossible-to-meet standard. Conversely, if an idea agrees with existing narratives, it is held to a very low standard in order to be published. This is an extremely common issue and why much of the most useful research I come across is not published in peer reviewed journals.
•In order for a study to be conducted, it frequently needs approval from the FDA (or an equivalent) and in most settings needs approval from an Institutional Review Board (IRB). In general, it is very difficult to get approval from the FDA to conduct any type of study unless a lot of money is behind the endeavor (for example I was familiar with multiple teams who had safe and effective treatments for COVID with supporting data that nonetheless could not receive FDA approval to begin their human trials). Similarly, despite the fact that extremely unethical human experiments are often conducted under an IRB, IRBs typically will not approve “controversial” research, leading to it not being done.
As a result, I frequently hear of fascinating therapeutic discoveries made outside the normal research process through trial and error that greatly benefit those who receive them, but in most cases these approaches can never be published because no IRB is willing to evaluate them. An excellent 2016 article published by the Association of American Physicians and Surgeons (a group that has also continually advocated for COVID patients) summarizes how many actually useful medical discoveries are made in independent clinical practice, but the recent hierarchal shifts in medicine have made it so this process is becoming continually rarer and rarer.
The accepted practice of medicine is also a hierarchy largely dictated by “medical evidence.” The existing hierarchal structure here makes it so that contrary research that does end up being published nonetheless is prevented from challenging the status quo. I will review some key examples:
•Medical practice is largely determined by “guidelines” that each physician is expected to follow. In most cases if you follow existing guidelines (ie. don’t treat someone with COVID until they have respiratory failure, then put them on a ventilator and give them remdesivir), you get paid and cannot get in trouble. If you do not follow guidelines, it becomes possible for you to be sued for medical malpractice, health care systems will fire you, and medical boards may take your license.
To illustrate physician attachment to guidelines: Throughout the pandemic I have participated in an online forum that approximately 100,000 US healthcare workers use. As you would imagine, the general mentality there is very conventional. One of the more interesting things I noticed in the early days of the pandemic was health care providers desperately asking for and enthusiastically sharing COVID-19 treatment guidelines from various academic institutions, while at the same time aggressively shooting down independent suggestions or ideas raised by individual physicians.
Guidelines are supposed to be made by impartial committees of experts tasked with reviewing the existing evidence in order to determine the most appropriate guidelines. In reality, as pointed out in Steve Kirsch’s article, these committees are extremely biased, and selectively choose evidence supporting the prevailing narrative.
In most cases, the decision of these unelected guideline committees goes unchallenged and even though they should not be (as discussed later), they are in effect the law.
The only exception I know of occurred when the Lyme community sued the Infectious Disease Society of America (which has also published widely cited COVID treatment guidelines I and others strongly disagree with). The lawsuit challenged IDSA’s guidelines that argued against the use of antibiotics for chronic Lyme disease, which was frequently being used by insurers to deny payment for those treatments and as a basis for authorities to crack down on those treatments being administered in private practice.
•Many people can only afford medical care covered by their insurance. In most cases, insurance will only pay for treatments supported by guideline committees and forces providers to spend most of their time fulfilling requirements of the insurance companies rather than treating patients. As you would imagine, significant financial entanglements exist between hospital systems, pharmaceutical companies and insurance companies (for example they often share interlocking board members), which further incentivizes specific therapeutic approaches.
The insurance dynamic creates the unfortunate situation where many people who need help for a condition must depend on word of mouth to identify a physician outside the insurance system who they have to pay for out of pocket. Provided they find the right physician and can afford their care (each of which is often not the case), these individuals often are able to recover from their illness.
•Reciprocally, insurance companies will often pressure health care providers to perform certain services for each patient that “improve quality of care.” If you follow those suggestions (which frequently results in most of the visit being taken up to do so), you are paid more by the insurance companies. Since everyone in health care is tight on money, those incentives result in significant pressure being put on physicians from their administrators to follow those suggestions.
The problem is that many of these suggestions encourage doing things I do not believe help patients and often harm them. For example, one of the reasons doctors aggressively push vaccines to their patients is because insurance companies pay them significantly more for all visits if most of their patients (especially children) are vaccinated. Similarly, one of the reasons why hospitals have been so aggressive in forcing ventilation and remdesivir (to the point they will fight expensive lawsuits to continue doing so), is because Medicare, in accordance with the COVID treatment guidelines, pays them a lot more to manage (and then kill) their patients in this way.
•Federal, state and municipal law enforcement authorities will frequently target those who promote treatments that violate guidelines. In my own experience (and for many others), IV vitamin C has been extremely helpful in certain (but not all) COVID cases. There is also research showing a benefit in COVID from this therapy Nonetheless, the guidelines recommend against it and individuals who publicly promoted IV vitamin C (at a time when no treatment for COVID-19 was available) had their clinics raided and were criminally charged.
•The media will attack any controversial treatment by claiming there is no evidence for it, and simultaneously refuse to report any evidence that emerges in favor of it. Likewise, Big Tech aggressively censors anything that goes against the existing medical narrative. For example, early in the pandemic, a video was posted by a leading researcher who had conducted clinical trials on using IV vitamin C for COVID-19 presenting his data to the NIH. This video was removed by Youtube shortly afterwards for violating their COVID misinformation policy.
How the Hierarchy is Bought Out
As you might imagine, the hierarchy outlined before is immensely susceptible to bribery. As so much money is in health care, this is what always happens.
•When the Affordable Healthcare Act was passed in 2010, its goal was to make health care more affordable. In 2009, total USA healthcare costs were 2.6 trillion dollars. In 2020 it was 4.3 trillion dollars (compared to wages going from $40,711.61 to $55,628.60 per the SSA). As this data shows, Obamacare failed its stated objective. I believe the central problem with Obamacare was that the medical industry is the largest lobbyist in Congress. Because of this, they were able to craft Obamacare to benefit their industry and thereby remove each provision that would have achieved the stated goal of the Affordable Health Care Act, leaving us instead with a variety of highly problematic federal regulations.
•The pharmaceutical industry is the largest sponsor of the mainstream media. For this reason, they prevent stories critical of pharmaceutical products from being discussed and regularly air stories promoting pharmaceuticals. Likewise, they will relentlessly attack anything that opposes mainstream pharmaceutical positions (frequently “cancelling” it and labelling it unscientific and without evidence). During COVID-19 this trend has accelerated following the Biden administration dispensing 1 billion dollars to news outlets across the political spectrum in return for positive coverage of the vaccine. I do not know of any past precedent for this.
Many journalists have complained about their inability to criticize dangerous pharmaceutical products, and to my knowledge, Tucker Carlson is the only individual with a mainstream platform who has (occasionally) spoken out against the industry. In recent times Big Tech and Big Pharma (who during Obama’s presidency became the core sponsors of the Democrat Party) have financially merged with each other, and like the media Big Tech now has a similar commercial interest in protecting Big Pharma’s monopoly.
•Most medical journals are primarily funded by pharmaceutical companies. Because of this, there is a strong bias to publish questionable industry sponsored trials. Conversely, there is also a strong bias to not publish data supporting alternative therapies that challenge their sponsors (an early example of this this is explicitly detailed and can be found within the 2001 book Heart Frauds but I am sure many earlier ones exist). As many of you have noticed, this publication bias has gone into overdrive throughout COVID-19.
•”Large randomized double-blind studies” are typically considered to be the best form of evidence, and many individuals will reflexively dismiss a study unless it fulfills that criteria. The problem is that these types of studies are immensely expensive to conduct, and in most cases can only be done if a pharmaceutical company sponsors them.
As you might expect, numerous studies have shown that when pharmaceutical studies are compared to noncommercial studies, industry studies tend to greatly overestimate the benefits of a drug and understate its harms. This is due to them having a large number of (fraudulent) tricks to create the “scientific” outcome they want. One of the best known recent examples concerned an article in the BMJ discussing a whistleblower who provided proof widespread fraud occurred during Pfizer’s vaccine trials.
While a small benefit can be attributed to the placebo effect (hence suggesting the need for a “placebo controlled trial), in most cases, the bias that emerges from the inherent conflict of interest in a pharmaceutically sponsored trial greatly exceeds the placebo effect. This is extremely important to understand, but rarely understood.
Even in non-blinded studies where a large magnitude of benefit is found (which greatly exceeds any possible placebo effect) those results are typically ignored or dismissed in favor of corporate sponsored research. A sad reality with many scientific publications is that if you read the author conflict of interest disclosures (which intentionally omit key details) and see who sponsored the study of the study, you can typically predict most of what will be written within the publication.
•Most researchers and academic institutions are extremely short on money. Because of this, they are forced to accept pharmaceutical money for any type of research they want to do, and in most cases not ask questions that will upset their sponsors (and even when honest researchers exist, administrators directly concerned with institutional finances will keep them in line). To a lesser extent, they can also function through public grants, but as detailed in “The Real Anthony Fauci” the grant system has been compromised so only researchers who support the mainstream narratives (and have not opposed Anthony Fauci) can get grants. Many respected scientists I have learned a great deal from, believe the corruption of the grant system, which Fauci is largely responsible for, has prevented American science from developing innovative scientific discoveries that were frequently developed in the past.
•In many cases, guideline committees are composed of individuals who have a direct financial conflict of interest over the guidelines they are promoting. The Lyme disease lawsuit for instance was filed on this basis. Malcom Kendrick an English physician who has done an excellent job illustrating many of the scams conducted by the pharmaceutical industry provided one of the best examples for this concept in his book Doctoring Data.
Many physicians are of the opinion statins (which lower cholesterol) have minimal benefit in preventing heart disease and expose patients to frequent and significant adverse effects, but since statins were put on the market, guideline committees have continually lowered the acceptable blood levels of cholesterol, thereby significantly increasing the pool of people who could take statins (leading to the situation that on almost any medical board examination, the correct answer is almost always “give the patient a statin”).
Kendrick’s specific example was that on the guideline committee responsible for determining who needed to receive statins in the United States, every single person who was on the committee (except the chair who was legally barred from it) had a financial conflict of interest with statin manufacturers. As you might guess, one of the quality metrics that administrators have held meetings on and which I was forced to attend regarded not enough “eligible” patients at the clinic being prescribed statin therapy.
•One of Fauci’s major achievements was turning the NIH and NIAID into pharmaceutical production pipelines. This was largely accomplished by allowing federal officials who were involved with the discovery or development of a pharmaceutical that went to market receive royalties for the drug once it was approved that often vastly exceed their salary.
As a result, there is an inherent conflict of interest to push unsafe or ineffective pharmaceuticals through the regulatory process. This frequently happens, whereas non-commercial enterprises focused on public good can almost never receive approval for a medication. Many outside observers believed based on the existing data, remdesivir should not under any circumstances have received an FDA approval, yet it did, largely due to the FDA electing to waive all the required safeguards (such as needing to consult an outside advisory panel) put in place to prevent something like this from occurring.
One of the most interesting aspects of this scheme (detailed in the Real Anthony Fauci) was that Fauci developed a large network of principal investigators (PI’s are needed to run clinical trials) who hold significant sway in getting IRBs around the country to approve ethically questionable trials needed to get unsafe drugs to market. The Real Anthony Fauci also discusses the retaliation faced by honest regulators who raise objections to problems with those trials.
In short, pharmaceutical companies have always bribed regulators, but Fauci had the unique accomplishment of transforming this into being an integral part of the HSS where the regulators would often take it upon themselves to solicit those bribes.
•Lastly, physicians in everyday practice are remarkably susceptible to being bribed, and a cornerstone of the pharmaceutical industry is sending sales reps to convince physicians to prescribe their medications. A small number of physicians refuse to see reps under any circumstances as they feel it is immoral for their own financial self interest to influence their treatment of patients. Typically however, pharmaceutical reps are remarkably effective at accomplishing their goal of selling their chosen medication and many academic physicians who widely promote pharmaceutical products receive immense payouts for doing so.
Revisiting HIV
In my initial post on this substack, I stated I was able to predict much of what has happened with COVID three months before the pandemic started. This was because I have found whenever a formula is discovered which “works” it is typically reused over and over.
The story of HIV, for those interested was originally detailed in Peter Duesberg’s book Inventing the AIDS Virus, and then subsequently further discussed in The Real Anthony Fauci. Fauci’s conduct during this period appeared to have laid the blueprint for what was done with COVID.
At the start of the HIV, there was no cure and many members of the gay community suffered severe disease or died. As time moved forward, independent physicians working in the community discovered a variety of effective treatments for the AIDS patients, some of which were alternative therapies, but most of which utilized repurposed FDA approved drugs. Like the stories shared in those books, a few of my own friends worked in HIV hot spots during this time, and each found they were able to save the lives of their patients if they abandoned government recommendations and tried their own protocols.
Despite endless requests to study these approaches, Anthony Fauci blocked every single one from being studied or adopted into standard of care. In parallel, he pushed along research on a highly toxic drug, AZT. AZT had originally been intended to be used for chemotherapy, but was abandoned as it proved to be too toxic.
While AZT should have never been approved, Fauci was eventually able to manipulate one (terrible) study enough that alongside sufficient pressure being applied to the FDA, earn AZT an FDA approval. Once AZT entered the market, as was obvious from the existing clinical trial data, it significantly worsened the prognosis for AIDS patients, something both reported in each of those books and also reported to me by a few colleagues who observed it enter the market. Despite being responsible for killing many members of the gay community (who at the time protested against Fauci for being a mass murderer), Fauci was hailed a hero, became one of the most influential members of the US government, and made a lot of money in the process.
COVID-19 Treatment Guidelines
At the start of COVID-19, the WHO made the curious announcement that Remdesivir would be the standard of care for COVID-19, despite almost no evidence existing to support this decision. After finding out the drug was a nonspecific viral RNA polymerase inhibitor, I became worried it would likely be somewhat toxic to cells, as broad spectrum antivirals tend to overlap with chemotherapy drugs (AZT being one example).
My initial suspicion was that Remdesivir would also affect cellular RNA polymerases (the classic example you learn in medical school are poisonous wild mushrooms triggering organ failure through this mechanism). As I began hearing of reports of organ failure near the start of the pandemic from physicians in China, I prayed we would not see a repeat of AZT. Since that time, significant evidence against Remdesivir has been uncovered suggesting it should have never been brought to market and to some extent, like AZT, it appears Remdesivir has caused significant harm.
As I observed the trajectory COVID-19 was headed in, I formed the hypothesis that a new lucrative drug needed to be put onto the market which could be theoretically argued to treat COVID-19 (“remdesivir must work since it is a non-specific viral RNA polymerase inhibitor”) but in reality would not be effective and instead would worsen and prolong the pandemic. I suspected this strategy would be adopted since the profit from selling the drug could be channeled into keeping effective therapies off the market long enough for vaccines to enter the market. This sadly appears to be what exactly happened once the COVID-19 Treatment Guidelines Panel of the NIH made remdesivir the standard of care for COVID-19.
After Steve Kirsch published this (accurately titled) post:


It then occurred to me to work backwards and look up each member’s financial conflicts of interest. First I checked Open Payments (which typically indexes most physicians), and oddly could only find partial information for one of the three chairs. Payment data from 2014-2016 was available for Henry Masur, who in 2015, had received $581,445.00 in “research funding” from Gilead, the maker of Remdesivir.
I then compared this to the declared financial conflicts of interest and the NIH reported that 7 of the members reported financial conflicts of interest with Gilead. However, despite it even being easily viewed for Henry Masur on Open Payments, all three co-chairs lied and reported no financial conflicts of interest in their decisions (keep in mind that the chairs of these panels are not allowed to have financial conflicts of interest).
After a bit more digging I found this article which noted that all 3 co-chairs had undisclosed financial conflicts of interest with Gilead, as did 4 other members of the panel, along with 2 former members. The composition of the panel has changed quite a bit in the last 6 months, but at the time this article was written, the majority of the panel had financial conflicts of interest with Gilead.
According to those who were studying the conflicts of interest in the panel, once it was revealed that the majority had direct ties to Gilead other academics without connections to Gilead, additional members were added to the panel to conceal Gilead’s connection to the panel, which is in line with a common industry mantra of “the solution to pollution is dillution.”
Following my posting of this article, Meryl Nass alterted me to the fact Sharyl Atkinson (an excellent journalist and one of the first to blow the whistle on how vaccine injuries were censored in the media) also investigated the panel finding:
”We found that of 11 members reporting links to a drug company, nine of them named relationships to remdesivir’s maker Gilead. Seven more, including two of the committee’s leaders, have ties to Gilead beyond the 11 months they had to disclose. Two were on Gilead’s advisory board. Others were paid consultants or received research support and honoraria. Nobody reported ties to hydroxychloroquine which is now made by numerous generic manufacturers and is so cheap, analysts say even a spike in sales would not be a financial driver for the companies.”
As you would imagine, other pertinent conflicts of interests were also present for the co-chairs (for example Gulick had ties to J&J). The conflicts of interests within HSS to the COVID-19 vaccine manufacturers (a much longer article) dwarfs any of those linked to Gilead. For example the second official appointed by Trump to head the FDA, Commissioner Scott Gottleib is now on Pfizer’s board, while the commissioner who was in charge of the FDA for the entirety of Operation Warp Speed Stephan Hahn is now an executive for the venture capital firm that launched (and still owns) Moderna. Likewise, the rank and file had similar conflicts of interest. For example, numerous members of the FDA committee that voted on approving the Pfizer vaccine for children (which was arguably the FDA’s worst approval in all of this) had worked for Pfizer.
Thousands of reasons have now emerged for why the COVID vaccines should never have been approved for human use, and many more safety signals have accumulated since they were released that would normally result in them being immediately pulled from the market. Despite facing the largest public protest against a regulatory decision in history, the FDA has done nothing to address these concerns and instead is now moving towards approving boosters for children and a second booster for adults. This behavior is perplexing to say the least, but makes more sense when you realize the heads of the agency were directly bribed by the vaccine manufacturers.
I strongly suspect there are additional conflicts of interest with Gilead and the members of the guideline committee that have not yet been identified. Given the national importance of these conflicts of interest and my own limited time (I only performed a very superficial evaluation of their potential conflicts of interest), I would strongly encourage a fellow citizen journalist to produce a full picture of the panel’s conflicts of interest. If that is done, I will do everything I can to make sure it is promoted.
To conclude this section, what this means in plain English is that the people directly responsible for much of the COVID disaster (hopefully this article has laid out the effects of their “guidelines”) did so because they were bribed. Additionally, whoever should have flagged them for having significant financial conflicts of interests before assuming the chair position did not.
The final question then becomes how on earth did they get to that position?

It turns out at least two of them had a close relationship with Anthony Fauci who as best as I can tell arbitrarily appointed them to chair (his) panel. Henry Masur, pictured above and his appointment is discussed here.
H. Clifford Lane (the NIAID Deputy Director for Clinical Research and Special Projects), had previously been exposed in a now deleted Associated Press (AP) article. That 2005 article discussed the AP’s Freedom of Information Act request (FOIA) that revealed 51 NIH scientists were “currently involved in testing products for which they secretly receive royalties.”
Fauci and Lane had received “tens of thousands of dollars” in royalties for an experimental AIDS treatment they invented [interleukin-2] as they directed the NIH to spend millions in tax dollars to test the treatment on patients across the globe. For example, 36 million dollars of tax payer money was spent testing IL-2 at more than 200 sites in 18 countries. Once again to illustrate the relationship between chemotherapeutics and antiviral drugs, IL-2 is now primarily used in treating cancer and has a significant toxicity similar to other chemotherapies.
In 2000, prior to the 2005 AP FOIA, the Secretary of Health and Human Services had issued a federal requirement for NIH scientists to reveal their conflicts of interests to subjects they enrolled in their trials. This is fundamental to medical ethics and most potential research subjects will choose to not participate in questionable research if they know the clinical investigators have a financial conflict of interest to pursue that research.
However, the 2005 AP FOIA revealed that members of NIH had not, as required disclosed their financial conflicts of interest. In fact, according to the AP, the NIH did not even consider doing so until the FOIA was filed. While in recent times the AP has jumped on the Fauci bandwagon, in 2005 they still had integrity and were appropriately outraged at the clear ethical issues with this conduct, demanding basic reforms such as HSS whistleblower protections and justice department oversight to be put in place.
Many of the studies Fauci and his principal investigators pushed through were questionable, dangerous and likely motivated by greed. For example, in the early days of HIV, black and hispanic orphans in New York were forcefully administered highly toxic and unnecessary HIV drugs. The children suffering horrific side effects could not leave the study, even when adults involved in the study attempted to adopt them so they could be withdrawn, and over 200 children died.
Not surprisingly, none of the AP’s suggestions ever happened, but it is always helpful to look back on what had been said in the not too distant past to see how quickly things have changed. While the media has always been corrupt, it is incredible how much worse it has has become in the last twenty years.
As one of the top officials within NIAID, since 2005 H. Clifford Lane has continued to work hand in hand with Fauci. This included being an author on the African Ebola study (published in the prestigious Lancet) which showed remdesivir had the highest rate of death from any treatment they attempted, and the more recent (and questionable) NEJM study used to justify remdesivir being a treatment for COVID-19.
I was unable to find any connection between the final co-chair Roy M. Gulick and Fauci. However, as they worked in nearly identical fields (Gulick is chief of Cornell’s division of infectious disease, and frequently conducts research particularly relating to AIDS medications), it is quite likely they frequently crossed paths.
On a broader level, the entire NIH (which often functions as an extension of Fauci’s dictates) had a conflict of interest with remdesivir. While Gilead claims to have invested 1 billion dollars developing remdesivir, research from the Center for Integration of Science and Industry determined that between gathering knowledge behind remdesivir’s chemical structure and molecular target, the NIH invested as much as $6.5 billion between 2000 and 2019 developing remdesivir. Much of the research to develop remdesivir was led by Ralph Baric, Fauci’s co-conspirator who is also the individuals directly responsible for creating the virus that caused COVID-19. This was done through documented (illegal) gain of function research, and referenced when Rand Paul interrogated Fauci during a senate hearing.
Early in the pandemic, despite highly questionable evidence the HHS signed a deal to buy the entire supply of remdesivir for approximately 3200.00 per treatment course (while the Gilead’s production cost was approximately 10.00). An estimated 500,000 doses were purchased, and this resulted in well over a billion dollars going to Gilead. Typically, when the government makes an investment of this scale (both in the development and acquisition of remdesivir), it will always do everything it can to utilize the investment (this is one reason there has been such a push to “use” all the vaccines the government pre-paid for).
With all of the above information, I believe it is very likely multiple members of the guideline panel, particularly Lane, have received royalties for the sale of remdesivir. At this time there is no way for me to assess who is receiving royalties, and I am doubtful in this present era groups like the AP will again investigate if that is the case. This once again demonstrates how independent journalists, such as those enabled by substack’s model are so crucial in this current era.
Conclusion
The Real Anthony Fauci makes an excellent case Anthony Fauci was the party ultimately responsible for the remdesivir fiasco and to an eerie degree did the exact same thing he did decades before with AZT. Fauci secured funding from numerous branches of the government to study and develop remdesivir, pushed it through to a drug approval despite it being both dangerous and ineffective, and he kept competing generic drugs such as hydroxychloroquine from being permitted for patient care and disrupting his monopoly.
Given all of this, it is not surprising Fauci gave himself the authority to appoint the panel to evaluate COVID-19 therapeutics, and selected individuals with massive conflicts of interest in favor of remdesivir to chair this panel. A common PR tactic reviewed in this previous article exposing the PR industry is how corporations will sponsor third party groups that “appear” to be independent and on the public’s side to promote industry interests. For some reason people always trust these “independent” groups and it appears this is what was done by Fauci in the creation of an “impartial” committee to determine the appropriate treatment guidelines for COVID-19.
When I was young, my uncle told me that for many people, if they are given the choice between getting money (or prestige or protecting their ego) and doing the right thing, they will chose to not do the right thing. He had witnessed hundreds of pretty horrendous examples of this happening and related many of them to me.
In reviewing the saga of the COVID-19 treatment guidelines, it is very clear many of the responsible parties also chose their own self interest over doing the right thing. As a result many died, and the pandemic was extended for a period of time sufficient to put millions into poverty and erase generations of wealth (depending on the estimate that 30-40% of small businesses have closed). Beyond the absurdity of the lockdowns, a good case can be made that the decision to purchase and mandate remdesivir was the action most directly responsible for the high death rate within the United States from COVID-19.
A common complaint from many conservatives pertains to “unelected government bureaucrats taking away our freedoms.” Despite their decades in government where they have shaped the health care policy that controls our lives, no one ever elected Fauci or those three co-chairs to their position. Someone just appointed each of them to serve their own agenda.
It is important to note no law existed that gave either Fauci or his COVID-19 treatment committee the authority to mandate remdesivir. Nonetheless, it has been aggressively mandated by nearly every party that could mandate remdesivir. Simple standard legal remedies that could have prevented some of this from happening, such as provisions against clear financial conflicts of interest in the guideline committee were non-existent.
While the lawsuit against the IDSA’s lyme disease treatment guidelines was ultimately dismissed, the judge’s basis for doing so relied upon two premises. The first was his agreement with the evidence that supported IDSA’s guidelines. The second was “IDSA’s guidelines…make clear that adherence to the guidelines is voluntary, with the ultimate determination regarding their application to be made by the physician in light of each patient’s individual circumstances. “ Hence even though guidelines are treated as law, it appears that the only federal ruling assessing them clearly states they are not.
It’s a fact of life there will always be bad people in the government. Democracy and laws restricting the actions of the government historically are the best remedies we have come across. Because the NIH has been allowed to operate outside of this, bad things always happen, and the corruption within the organization has grown by leaps and bounds since Fauci transformed it into a pharmaceutical pipeline.
If there is a sincere public interest in preventing another similar to the COVID-19 treatment fiasco, I believe this is where the focus must be directed. In studying the history of American politics and political activism, I’ve found most permanent changes only result through protest movements spending years of blood sweat and tears to force the passage of laws that address the existing issue.
While there are likely better options, four laws immediately come to mind.
1. Short term limits must be in place for bureaucrats in positions of significant power (which could say be quantified by the amount of federal dollars they are responsible for). Fauci has been able to do much of his damage because he has been in his position for decades.
2. There must be a state level mechanism to prosecute the HHS officials for conflicts of interest because the federal government will not prosecute itself.
3. Although this is likely a much harder law to put into law, physicians must be given protections to practice medicine that falls outside industry sponsored treatment guidelines. Many of the people who survived COVID-19 survived because doctors at great personal risk elected to do so, and had laws protecting physicians been put in place, many more would have done so as well.
4. The appointment to any committee (especially to the chair position) must be decided through random selection from a pool of qualified applicants rather than direct appointment or “pay to play”. As this may not always be feasible, it must at least occur for committees whose decisions have carry significant financial weight (such as influencing spending that exceeds 100 million dollars).
Lastly, this committee issue is not unique to the NIH. In congress, most laws and congressional actions (ie. investigations) result from the decisions of congressional committees. Because of this, the specific committees an elected official is placed on or chairs is the primary determinant of what they actually get done during their tenure.
Congressional committee placement is just as corrupt a process as Fauci’s actions within the NIH. Periodically, senators and representatives speak out on this issue, but since both parties get so much money from the process, it is rarely discussed. Additionally, I now periodically hear discussions occurring within the ruling elite of if the committee model needs to be discarded due it being so corrupt it is now failing to solve problems delegated to committees. In the 4 minute video below, one Alabama representative gives an excellent synopsis of the situation within congress. Sharyl Atkinson has also covered this issue in much greater depth.
I sincerely appreciate each of you who takes the time to read these pieces, share their content and subscribe. I had hoped to write more but was unable to this week due to a few deadlines that recently emerged at work.
Postscript:
After writing this, I realized one point must be emphasized. Doctors (or other medical academics) cannot take pharmaceutical payments without being beholden to their sponsors. A lot of people assume you can in certain cases (ie. for research), but the reality is you can’t and that’s the primary reason why these payments are made.
Since the time I wrote this piece, two important investigations have been released.
The first one, by the GAO (summarized here) found that individuals within each federal agency tied to the COVID-19 response (CDC, NIH, FDA etc.) consistently reported that corruption had happened in their agencies and the policy decisions and recommendations did not follow scientific integrity. In addition, the GAO reported there was an institutional bias against federal employees being able to report corruption in their agencies. To my knowledge, this is the first time the federal government has admitted their own corruption with respect to COVID-19.
The second one summarized here, had a non-profit watchdog group attempt to replicate the 2005 AP investigation of royalty payments to the NIH. They found that contrary to the NIH’s promise for more transparency, the opposite had happened, and the NIH made it much harder to get any type of detail on what royalty payments they were receiving, using many of the same tactics the FDA used to block the release of the Pfizer documents.
From what the independent watchdog group was able to discern, the royalty payments and corruption has ballooned since 2005 and the key members of the NIH’s leadership now receive dozens of pharmaceutical payments. This results in a bias existing to only approve (and then mandate through corrupt guideline committees) medications which members of the NIH have a financial conflict of interest in approving. This is particularly concerning given that both remdesivir and Moderna’s COVID vaccine are owned by the NIH and despite many red flags against their use have been forced on the population.
Lastly, Dr. Malone recently wrote an excellent insider’s view of the corruption within the NIH and the society in general. For those wishing to further understand this issue and understand where all of it is going, I would highly suggest reading this piece:
Re-posted from elsewhere: The lies are so transparent at this point that if you still can’t see through them then you’re practically an NPC as far as I'm concerned. That’s not a dig at democrats at all, it’s a dig at anyone still fooled by this con this late in the game.
The FDA has been hiding massive Pfizer COVID vaccine damage & death since as early as Feb of 2021 (meanwhile the CDC chief has been lying directly into our faces by telling us the vaccines are safe and effective throughout the rest of that year):
http://tritorch.com/HiddenVaccineDamageAndDeath [image]
So of course the FDA needs another 55 years in order to release the rest of this data:
http://tritorch.com/FDAWants77Years [image]
The CEO of Pfizer and the EU Commission Chief are in love, so together they've decided that mandating blanket injections and vax passports is what's good for Europeans:
http://tritorch.com/matchMadeInHeaven [image]
The near universal global ban on Ivermectin and HCQ, the lockdowns, the six feet, the masking, the mandates, and most importantly of all _the vax passports_ were strategies all orchestrated and enforced from a place that resides above the sovereignty of nations at the very top of the global power structure.
That practically every nation on the planet all moved in lockstep to adopt these strategies simultaneously while using eerily similar language to explain the reasoning for them - and all for a cold virus with a survivability rating of 99.85% - should tell you in big G.L.A.R.I.N.G. letters that the nations themselves and the politicians that run them are merely the puppets of a higher authority. Here's one:
http://tritorch.com/KlausSchwabWEF [video 1min]
And finally, here is Maajid Nawaz detailing this globalists' con to Joe Rogan - leaving him speachless:
https://www.bitchute.com/video/8JHGfuJSXd71 [video 2min]
The only way out of this onslaught of medical tyranny is to burn the entire system down because the system is rotten to the core and is woven together by blanket webs of interlocking incestuous corruption. It cannot be untangled or fixed as each corrupted entanglement has a stranglehold on the ones surrounding it. It can only be demolished and rebuilt from scratch.
https://tritorch.com/illFaresTheLand
One way the members of the NIH COVIS guidelines committee were able to hide their financial conflicts of interest was that they were only asked to disclose conflicts occurring within the prior 11 months. When Shark Attkisson looked at their financial conflicts over the past several years she found 16 total members had financial conflicts with Gilead