A Landmark Study on Vaccine Injury Once Again Proves Systemic Corruption in the COVID-19 Response

A central theme I have tried to illustrate here is how the same scams recur throughout history, which I believe is largely due to a general lack of creativity and a human tendency to default to strategies which have already proven themselves. For this reason, once you start to understand what methods are typically utilized, it becomes possible to correctly interpret events presently occurring around you.
Recently, an article was published here discussing the anatomy of corruption within the federal government. This corruption caused the federal government to promote dangerous, ineffective, and highly expensive therapeutics for COVID-19 while simultaneously prohibiting the usage of affordable, safe and effective therapies.
Two follow up articles were then as additional evidence of corruption emerged. The first detailed a recent investigation by the GAO, which what is the first official confirmation that this corruption was occurring. The second detailed a recent investigation by two independent watchdog groups that also confirmed this corruption was occurring within the NIH. That series, particularly the first part listed above, provides a valuable context for understanding this article.
The Covid Vaccine Trials
When the vaccine trials were first announced, potential participants were told that they were playing a critical role as heroes doing their part to save humanity. They were promised that the most ethical and transparent usage of their data would occur, and that if anything whatsoever went wrong every step would be taken to make things right and these heroes would be taken care of.
Having studied many previous drug trials, those of Gardasil being the best example (where many girls were injured, but the trial just covered those injuries up and did nothing to support the suffering girls), I was quite dubious any of these promises would be honored. Many who did not share my views trusted the promises they were given and willingly enrolled in the COVID-19 vaccine trials. Many of those individuals have since been red-pilled due to the horrible treatment they received after participating in these clinical trials.
While the trials were being conducted, I joined private support groups for individuals participating within the trials. There I noticed numerous participants reporting severe adverse events from the vaccination, which affirmed to me it was unlikely these vaccines would be safe.
When the landmark NEJM paper on Pfizer’s vaccine, “Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine” was published, I could not help but notice some of the severe adverse events I had read in the support groups report did not end up in the final publication, which was especially cheeky given the title of the paper. I attempted to explain this lack of data integrity to a few colleagues as justification for postponing vaccination, but they argued my observations lacked validity and insisted the peer reviewed results that refuted the occurrence of those adverse events is what should be trusted. As you might imagine, encountering this type of logic is very frustrating.
Despite this foreknowledge of the potential toxicity of the vaccinations, once the vaccinations enter the market, nothing prepared me for the tsunami of adverse events that occurred. Before long, this led me to decide that I had a duty to compile a log of those within my own circle who have been severely injured (detailed here), and before long I realized I alone knew of enough critical vaccine injuries (43 in total, most of which were fatal) to meet the threshold that typically required vaccinations to be pulled from the market.
From everything I was observing, I concluded that the following was true:
•For a yet unknown reason, the governments of the world had decided it was critical to get as many people as possible vaccinated, and anything that prevented this from happening was not to be permitted
•There were a large number of people suffering fatal or debilitating circulatory, neurological, and autoimmune conditions following vaccination at a significantly higher rate than I had observed from even the most dangerous pharmaceuticals on the market.
•Those who were injured were completely out of luck with receiving any empathy, support or treatment for their injury.
•Give or take everyone who was injured was being subjected to a massive gaslighting program every major social institution was complicit in.
Medical gaslighting is an issue that profoundly bothers me and has tortured many close friends of mine. As gaslighting has been so central to the entire pandemic response, a recently completed a five part series on medical gaslighting can be reviewed in this sub stack. If you are short on time, the first part of the series is the most important one to read. Many of these forms of gaslighting illustrated in that series were likewise reported by Brianne Dressen.
Deliberate Scientific Censorship by the NIH
Brianne Dressen was a participant in AstraZeneca’s COVID-19 vaccine trial (AstraZeneca’s vaccine is very similar to J&J’s) who previously spoke at Senator Ron Johnson’s panel on COVID-19 vaccine injuries. Maddie De Garay, also attended this forum and was a subject in Pfizer’s small study of vaccine safety for children. Maddie suffered significant neurological complications from the vaccine which were concealed by Pfizer, which led many healthcare professionals to erroneously assumed the vaccine was safe for children) Dressen, like Maddie experienced severe neurological complications after her experimental vaccination that persisted and have severely impacted her life.
When Dressen’s injury occurred, AstraZeneca sure enough reneged on the promises it had made at the start of the vaccine trial. AstraZeneca dismissed her injury, gave her no way to report it, and failed to provide her any type of support for dealing with the injury. In fact, until a few weeks ago (at approximately the end of April 2022), she had had no contact with AstraZeneca as they had declined to respond to Dressen’s communications.
As he had connections to the medical and scientific field, Dressen’s husband contacted the NIH in January 2021 regarding her severe neurological injuries. On May 20th, 2022, Dressen conducted an interview detailing her process with the NIH.
I would advise watching the first part of this interview. In addition to highlighting the dishonesty of the clinical trials, it once again provides proof of the systemic corruption within Fauci’s branch of the federal government.
*If this gets pulled (which has happened with other videos linked to in these articles), I will re-upload it on another site, but for now I would like to direct traffic to the original uploader.*
Initially, the NIH took Dressen’s symptoms very seriously, asked for blood samples and requested to fly her to the NIH for an evaluation. Since the NIH was one of the only official groups evaluating these injuries, they were soon met by a deluge of other patients with the same symptoms.
Once this deluge occurred, the NIH became progressively more hesitant to study the subject, and five months later in June, Dressen was one of the only vaccine injured patients who was permitted to come to the NIH for evaluation. After her visit, she and the other participants were instructed to provide detailed logs of their symptoms to the NIH and rescheduled for a return visit in September 2021. This visit was then canceled, the NIH became much more cryptic on the subject of neurological vaccine injuries, and by the end of 2021 had gone silent to both patients and their healthcare providers.
Initially, the subjects that were evaluating by the NIH (they for instance had agreed to painful biopsies) were promised the case study they were part of would be published within a few months over the summer of 2021. The study was instead pushed back over a year for publication, and the pre-print that is now available arrived 17 months after Dressen initially contacted the NIH regarding her symptoms.
This almost certainly means that the department within the NIH, the National Institute of Neurological Disorders and Stroke (which is responsible for evaluating complex neurological injuries of public concern), was initially eager to evaluate Dressen’s case. Once it became clear that a large number of individuals were suffering the same injury as Dressen, leadership within the NIH came to the conclusion it was unacceptable to publish anything which could encourage vaccine hesitancy.
As a result, a study that would have normally been prioritized to be published as quickly as possible was instead mothballed.
You may recall that during this 17-month period, we were repeatedly told there was no evidence significant complications followed COVID-19 vaccination, and various authoritative groups such as the NIH were repeatedly cited to dispel the possibility these injuries could be occurring. Whenever evidence was nonetheless brought forward attesting to the fact, it was dismissed on the basis of it not being credible (i.e. it was not conducted by an appropriate party or it was not published in a credible scientific journal because it was unsuitable to pass review).
Throughout the pandemic, Fauci was the individual best known for doing this, as he would repeatedly state on television no evidence existed to support positions that ran contrary to his agenda, and when evidence that did emerged, he would dismiss it as un-credible. Rather than independently examine the science, pronouncements from “experts“ such as Fauci were treated as gospel by every large organization.
These pronouncements were also used by social media platforms to justify banning groups discussing vaccine injuries. For example, I participated in a group with over 100,000 people seeking support for their vaccine injuries, which was then erased by Facebook (and had it not been deleted, many useful treatment strategies likely could have been discovered by the participants, who in many cases are now completely on their own).
Because of all of this, whenever an individual attempted to share injuries they had suffered from vaccination to a medical professional, they were gaslighted by that healthcare worker who simply repeated the official messaging that there was no evidence these adverse reactions could be occurring. Likewise, when individuals bring forward concerns of side effects they have seen in their social circle from the vaccine, they are told those events were unrelated coincidences, to trust the federal government had verified there was no danger with the vaccine and that it was urgent to get vaccinated as soon as possible.
It is hence understandable why the NIH would have mothballed a study of this nature. If it were to have been published, while it would have prevented many future severe vaccine complications, it also would have heavily undermined the vaccination drive. Beyond this behavior being inexcusable, it is also a textbook example of deliberate gaslighting: the NIH ardently insisted none of this was occurring while they were simultaneously blocking an internal publication showing it was.
It should also be noted that a key detail of the study (as reported by Dressen) was that the NIH used the same criteria for evaluating long-haul Covid to evaluate the vaccine injuries. This demonstrates from the get go that the NIH had an intimate knowledge of the toxicity of the spike protein and was deliberately withholding a large degree of critically important knowledge on the toxicity of the vaccines. Likewise in the paper, the NIH acknowledged that their findings suggested a progressively increasing autoimmune response to spike proteins found both within the disease and its vaccination (which I and others very much believe is true).
In the previously mentioned report produced by the GAO, the watchdog arm of the federal government, its key conclusion was that within each federal agency tied to the pandemic response “political interference in scientific decision-making occurred.” The suppression of this study is likely one such example of that political interference.
At the very start of the COVID-19 vaccine campaign, I became very concerned by how aggressively the public relations industry was pushing the vaccine (summarized here). No other PR campaign has ever been that aggressive in my lifetime.
I hypothesized that the goal would be to vaccinate the maximum number of individuals within a population, and that a variety of progressively more aggressive tactics (each of which would be enabled by an increasing number of vaccinated civilians) would be implemented as the market for each previous option became saturated. Part of the reason I suspected this would occur was because over the last decade I had watched the gradual rollout of an aggressive campaign to normalize the mandatory immunization of non-consulting adults (detailed here) and what we were now witnessing appeared to be the next logical progression in that plan.
If you think about the entire sequence of events, this makes sense, as each time the maximum uptake for one approach was reached, we then were transitioned to a more aggressive approach. I would summarize the events within the United States as follows:
•First everything possible was done to make individuals desperately want the vaccine (which required censoring every single effective therapy for treatment of the COVID-19 and destroying people’s lives by locking them down).
•Next, the vaccine was hyped up as much as possible, and initially only given to the “holy“ healthcare workers who had “earned” the right to be first in line and get their lives back, thus marketing the vaccines to the general population.
•Next mass vaccine clinics simultaneously sprung up around the country.
•Next, when the vaccination uptake at these clinics petered off, bribes such as the vaccine lotteries and gift cards were deployed throughout the country.
•Next mandates were introduced at selected areas such as the military and hospitals where their requirement could be justified.
•Next, mandates were rolled out through corporate America and our colleges.
•Next, once market saturation for the initial vaccines was reached, the boosters were introduced.
•Lastly, once that market saturation occurred, the boosters were mandated.
The below graph illustrates this progression:
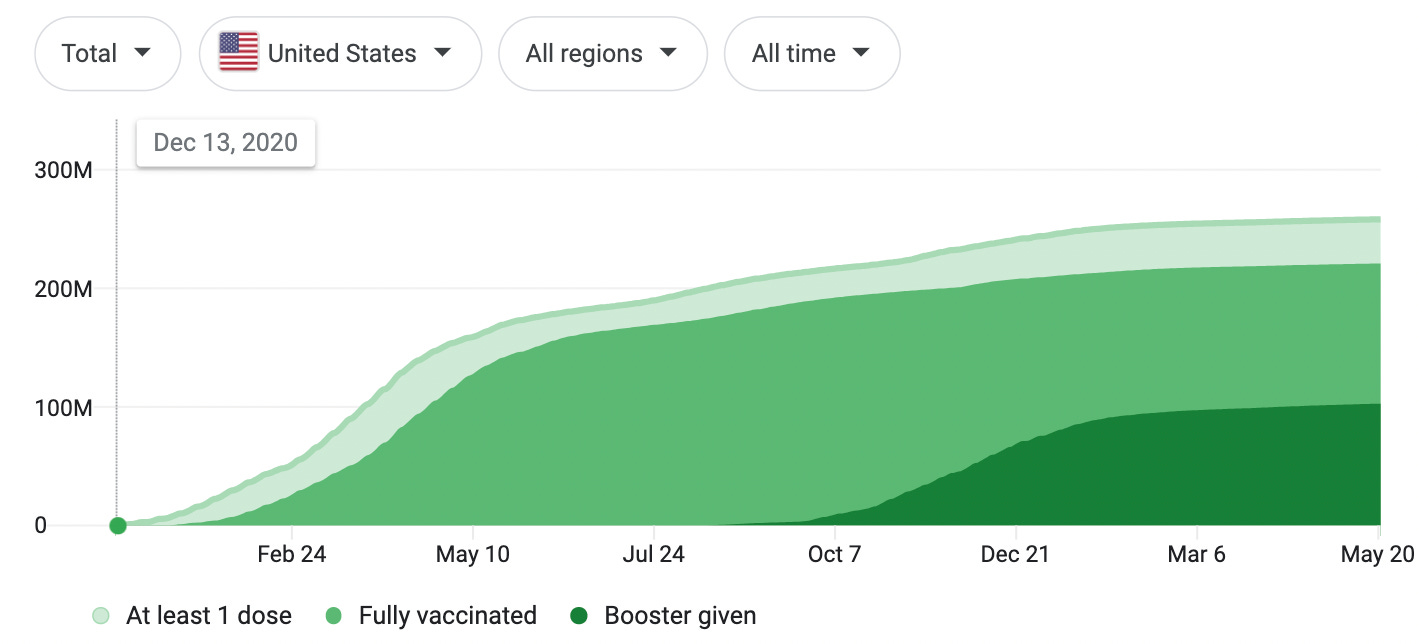
Given how coordinated the entire vaccination push was, it once again makes sense that political interference could have occurred at the NIH to force honest government officials to censor any type of research that would create “vaccine hesitancy.” I suspect the reason why this study is now being permitted for publication is because it has been concluded that the total market saturation for the vaccinations has been reached, and it is time to begin gradually pivoting towards profiting off of managing the vaccine’s side effects. It should also be noted that after the federal government received a large number of similar injuries from Gardasil, Merck’s HPV vaccine, they refused to disclose them and only did so after a FOIA was filed by Judicial Watch, an independent watchdog group.
Neuropathic symptoms with SARS-CoV-2 vaccination
The pre-print of the study can be viewed here. As this is the first official publication to acknowledge neurological injury from the COVID-19 vaccinations, there is great significance to the findings within this 23 person case study. I will briefly review some of the most important points.
First, the authors repeatedly emphasized that these events were very rare, and that the study was simply composed of 23 patients who self-referred themselves to the NIH. This creates the perception (which many skeptics reading it will adopt) that there are a tiny number of patients with neurological symptoms that may just be suffering from a nocebo effect. The authors likewise emphasized the safety of the vaccine and the rare occurrence of the side effects.
This is extremely disingenuous because the paper omits mentioning (as discussed above by Dressen) that the NIH blocked almost every individual suffering a post-vaccine neurological complication from being evaluated by the NIH. Similarly, the paper insisted that these issues were almost entirely unique to women, but this in actuality was due to who the NIH admitted into the study. I mentioned this point because there is a long tradition in Western medicine of gaslighting women with serious medical illnesses under the label of them being hysterical or having some other psychiatric cause for their illness. Presently, this most commonly arises in response to the frequent menstrual complications created by these vaccinations.
Second, the paper acknowledges that the 23 subjects were suffering from clear neurological disorders and it provided evidence to prove these effects were was not psychosomatic. I cannot overstate how important this is for those currently being gaslighted by their healthcare providers.
There are a few common types of complications that arise from the COVID-19 vaccinations, and this sample consisted entirely of the classical neurological injuries (as this study was conducted by department of the NIH that is specifically charged with evaluating neurological diseases). Other important side effects are not mentioned because they were beyond the scope of this study.
The two main pathologies acknowledge within this report are small fiber neuropathy and a wide assortment of autonomic dysfunctions. When you have autonomic dysfunction, it is very common for it to trigger both palpitations and anxiety. This is relevant because I am convinced that many gaslighted individuals who have been told their symptoms are due to “anxiety“ were erroneously diagnosed due to a textbook example of autonomic dysfunction not being recognized by the doctors they saw.
This category of injury also directly overlaps with the side effects typically seen from the Gardasil vaccine. This is particularly relevant, because the two main therapies the NIH used to treat these subjects were steroids and IVIg; both of which are used to treat Gardasil complications (IVIg does help). Pharmaceutical companies often sell treatments for side effects from their drugs, and the maker of the other HPV vaccine is one of the primary manufacturers of IVIg. Similarly, the FDA recently approved the first ever blood thinning agent developed for children (prior to the vaccines, it was exceedingly rare for children to develop blood clots).
From having dealt with a large number of individuals with chronic autoimmune and neurological injuries, I have found that the default approach most physicians will take is to administer corticosteroids. When the disease is infectious in nature and within the central nervous system, this can be catastrophic and I have multiple close friends with Lyme disease that was creating acute neurological symptoms who became permanently disabled immediately after a steroid administration.
More frequently though this is not the case, and the steroid briefly provides relief, but the relief disappears when the steroid wears off, tolerance to the steroid builds and increasingly more toxic doses are required (which often stop working). Beyond only partially addressing the condition, the steroids will create a wide range of exacerbations for the illness, and many other side effects (for instance a friend who like many others developed polymyalgia rheumatica after vaccination had multiple important ligaments rupture as a side effect of the steroid she was administered).
IVIg is more helpful, and while it does have side effects, as far as I know, it is less likely to create severe side complications than steroids are. However, it is prohibitively expensive (around $3500 per treatment), and there is no possible way enough of it could be produced from healthy unvaccinated donors to address the permanent need neurologically injured vaccinated individuals will have.
A related approach to IVIg, plasmapheresis also appears to be very helpful, but unfortunately it is also quite expensive and even more difficult to access than IVIg. I have also wondered if plasmapheresis may also be removing other toxic components of the vaccination the body cannot eliminate, and if a similar effect could be achieved with dialysis, but at this time I have no definitive way to evaluate either hypothesis.
I mentioned this long discussion on IVIg and corticosteroids because in the NIH paper, the authors claimed that these methods (particularly IVIG) could be used to cure the neurological vaccine injuries. When discussing the three patients who received one session of IVIG, it was stated: “In all three, symptoms improved dramatically within 2 weeks of IVIg treatment with complete resolution in one and mild residual symptoms in the other two.”
Dressen noted during her interview that these claims were dishonest as to her knowledge none of the participants in the trial had reported improvement. In Dressen’s case, taking a steroid provided a temporary relief while she was on the steroid, but when she stopped the steroid, it made things worse than they had been before. The expensive IVIg she received in turn only provides partial improvement for about two weeks and then wears off. Despite notifying the investigators of this well established declining response to IVIg, the investigators decided to evaluate the patient at two weeks, then chose to equate this brief window a symptomatic improvement to a permanent improvement from IVIg. Currently, Dressen is listed in the study as having fully recovered, but in reality she is still significantly disabled from her vaccine injury.
I am ultimately not sure what the political motivation is for acknowledging that the Covid vaccines can cause neurological injury and stating that they should be treated with IVIg (or possibly corticosteroids). Occam’s razor would suggest this is being done to sell IVIg in the future. However, like many things, that is ultimately speculation and at this point in time there is no way to know if the clinical investigators have financial conflict of interest with IVIg production (as the NIH is refusing to disclose the conflicts of interest of their scientists, which they are legally required to do by law).
Conclusion
I have been looking at a variety of treatments for COVID-19 vaccine injuries. There are a few my team has identified which seem to work very well, but we are in a situation where we have a small number of patients to test them out on (most of our patients will not vaccinate), and there is no feasible way for us to obtain more data from a larger patient pool.
Some of the results we have found how been extremely promising, but due to the small sample size we’re working with, we have been hesitant to share those results as we are not certain they will hold up in a larger sample size.
In most cases when you have a chronic autoimmune disease, the rheumatologic immune suppression approach can work, but it often only temporarily alleviates the disease, requires permanent usage of therapy, and creates significant side effects in the process. This is great for business, and in certain severe rheumatologic diseases absolutely necessary to do, however for COVID-19 vaccine injuries, it is not our preferred treatment approach. Additionally, the default approach for immunological management of vaccination injuries appears to be corticosteroid usage. Multiple rheumatologists I have spoken with (they are in a specialty that regularly requires administering a wide range of immunosuppressants) believe corticosteroids are amongst the most harmful immunosuppressants on the market, making this default treatment strategy somewhat concerning.
For individuals with Covid vaccine injuries, the process is very difficult and the majority of therapies available will be expensive and not help them. This is similar to the situation faced by many individuals with controversial diseases that are often dismissed and gaslighted by most of the medical system.
Many of the confirmed pathology findings here are very important, and it is my hope they will open the door for providing treatment to vaccine injured patients. However, from the way the study was conducted, and its deliberate suppression throughout the vaccine roll-out, various forms of corruption have been demonstrated and others must be suspected. It is very likely there is an ulterior motive to roll the management of vaccine injuries into the traditional lucrative approach used throughout neurology and rheumatology.
I thank you for taking the time to read this and your support of this newsletter.
Great post. From a historical perspective, such incredibly reckless (at a minimum) developments do not end well and could result in mass death or disablement.
I know one young and previously vaccinated person who clearly has some immunity problem, very often seriously sick with non-covid illnesses (and covid too) , hospitailzed etc, plus long covid, that do not spread to the rest of his unvaccinated family, despite the rest of the family not being more than of average health.
How likely is it, in your opinion, that the post-vaccine problems such as immune deficiency, will actually significantly affect our demographics?
(I hope that the answer and the end result will be that these concerns will not materialize)
For your statements of fact and critical analyses of them, I thank you.
Your observations regarding obscurantism and outright deception help provide context to a societal dynamic that has puzzled me for some years. There seems to be some sort of "don't ask, don't tell" dynamic regarding vaccine injury within the social contract, or so it appears to me.
Approximately a decade ago, I noticed something I considered rather odd. Mainstream expressions of opinion about the so-called "anti-vax movement" became increasingly devoid of information, becoming little more than exersizes in sneering dismissal.
Being supportive of vaccination writ large, but agnostic in relation to any given detail, I decided to explore the claims of what I thought a rather extreme fringe "movement." I was genuinely surprised at what I found, which was a rather wide range of opinion within a broad spectrum.
Within that continuum are viewpoints ranging from parents who wonder if administering innoculations in highly concentrated clusters might be inferior to spreading them out over a longer period of time with fewer combinations, to "vaccines are all pure poison!" The public narrative made no concession to such diversity of inquiry and opinion.
In a manner you might find touchingly naive, Doctor, I thought that this imbalance could be obviated with recognition of facts and a wee bit of compassion. After all, I reasoned, those who are injured and killed by adverse reactions to vaccines have sacrificed themselves for the good of us all and deserve to have their sacrifices recognized. I had thought that we all owe a debt of gratitude to these unfortunates, small in number as they are.
When I mentioned my exploration, discovery and conclusion to others, the responses were quite interesting. Universally, recognition of the injured and dead was vehemently opposed.
Ordinary individuals considered such recognition misplaced. The most telling example of this was expressed by an old soldier who thought that recognition was a form of "false valor" because few give fully informed consent to innoculation. I thought this a sensible viewpoint, and hearing it clarified a number of things for me.
What was most telling, however, was the reaction of the erudite. I was truly stunned by it. The wall of dissembling erected by their verbose deflections was impressive and disheatening. Time after time, I was confronted with extraordinary feats of rhetorical legerdemain. It was immediately apparent that such dishonesty was manipulative in nature and relied on a smug elitism that would brook no moderation whatsoever.
You have suggested that this is a form of gaslighting, Doc, and I have to agree. I find the varying motives self-serving, in the main. in it's simplest form, it seems to be some sort of a "whistling past the graveyard." Within the more complex and persistent "arguments" lies a combination of hubris and self-aggrandizement.
I truly appreciate the perspective that you bring to this subject. It seemed to me that the sort of reactions I encountered could not have arisen spontaneously. It became clearer with the advent of horrifyingly nonsensical and seemingly counterfactual hysteria in the official response to Covid.
A series of intersecting patterns have emerged, clarified by a few brave and knowledgeable souls such as yourself. You are providing a benefit to humanity in ways that will not be fully appreciated for a very long time. When providing a dominant narrative is considered preferable to maintenance of core values such as honesty and compassion, application of a corrective becomes necessary.