What is the Relationship Between Liquid Crystalline Water and Zeta Potential?
Untangling this mystery is key to addressing each

I believe healthy fluid circulation is one of the most neglected aspects of health and, ultimately, the cause of many of the COVID-19 and vaccine spike protein injuries we have seen. Unfortunately, since the topic is so neglected, very little knowledge exists of what creates these flows.
Although many factors influence fluid flow in the body, two bear particular importance as, in my eyes, life cannot exist without them.
The first is the zeta potential of the fluid, which defines the degree to which particles in it will repel each other rather than come together. When there is insufficient zeta potential in a fluid, that fluid will begin to clump together, and as the zeta potential in the body worsens, the flow in progressively larger vessels slows until it stops. It is difficult even to begin to describe all the different physiologic consequences of an impaired zeta potential (I tried to in this article), and in my own practice, I find poor zeta potential is one of the top three causes of health issues in the patients I see, especially in patients who are extremely ill (e.g., those who require hospitalization).
The following passage was written by Thomas Riddick, the colloidal engineer who was responsible for much of the research we still use on zeta potential:
In concert with a physician, periodic observations were made of the conjunctivas [part of the eye] of the writer's staff. They confirmed that even slight illness (such as a head cold, or “two-day virus,” or bacillary dysentery) can, in one day’s time, materially increase the degree of intravascular coagulation*. Our routine observations of the conjunctivas of persons with known cardiovascular disease (and atypical heart-beats and arrhythmia) reveal a definite and absolute correlation with their ECG’s.
That is to say, if periodic observations show a progressive lowering of intravascular coagulation (blood sludge*), then their ECG will show a corresponding decrease in the percentage of atypical (or malfunctional§) heartbeats; and vice versa. It is the writer’s experience that it is virtually impossible to find an individual with known serious cardiovascular disease who does not also have significant intravascular coagulation. As a generalization, an absence of intravascular coagulation can be found only in hemophiliacs, and persons in an excellent state of health below the age of twenty-five. But even this is not assured, because significant coagulations can sometimes be found in teen-agers.
*Blood sludging and intravascular coagulation are also referred to as "blood stasis," one of the classic diagnoses in Chinese medicine.§Riddick, with instrumentation, observed the heart would sometimes not pump blood even though a contraction occurred and termed these events "dysfunctional" heartbeats since a term did not exist in the medical literature for them.
One of the key reasons vaccines cause harm (which increases as more vaccines are given) is because all vaccines destroy the physiologic zeta potential of the body. This, in turn, explains why the most commonly observed vaccine injuries are deficits in cranial nerve function (especially those whose blood supply is limited and more vulnerable to blood clumping from a zeta potential collapse). The most susceptible cranial nerve is the one responsible for each eye being able to move to the side, and I have now lost track of how many people (including longtime friends) have developed this issue since receiving a COVID-19 vaccine (although a decent number don’t realize until you point it out).
Note: many other things can also impair zeta potential (malaria, for example, sometimes doing so to a fatal degree).
The second key factor governing flow in the body is liquid crystalline water, something observed by many throughout the centuries and scientifically quantified by Gerald Pollack. When water has a negatively charged surface and a source of ambient energy (which is typically infrared light—something all around us and also constantly produced by the body), water will transition from free H2O to a connected network of H3O2 that behaves like a semisolid and is best described as a liquid crystal.
Since hydrogen atoms need to be removed from the liquid crystalline water to make this transition occur (H3O2 is H1.5O, not H2O), they are found in a high concentration near the H3O2. Conversely, since the H3O2 has a semisolid structure, it will push everything else out and not allow anything to pass through it (leading to its boundary often being referred to as an “exclusion zone”). This includes the displaced hydrogens, which in contrast to the negatively charged H3O2 carry a positive charge.
There are a variety of significant effects of liquid crystalline water. First and foremost, it creates much of the structure and stability of the body all the way down to the insides of each cell. Secondly, it creates barriers that allow each surface within the body to slide frictionlessly against each other, protects cells from external damage, and maintains cellular integrity by preventing things from passing throughout. The lining of your blood vessels (the endothelium—which is coated with liquid crystalline water), for example, requires all of these to function, and one of the reasons the spike protein is so damaging is because of its ability to penetrate the protective layer which covers the endothelium. Lastly, it functions as an energy source that facilitates a variety of physiologic functions.
One of the most important functions of liquid crystalline water is that when it surrounds normal water as a tube, it creates spontaneous motion of that water from one end of the tube to the other. Many different organisms depend on a vast number of fluid movements inside of them. Still, in many cases, there is either no identified source for that motion, or the postulated source cannot account for all the motion observed. However, in each case where it is possible to assess the fluid vessel in question, a lining of liquid crystalline water is found surrounding it, and the vessel is structured so that the direction of flow of liquid crystalline water would be expected to create is what is observed.
For all of these reasons, I believe liquid crystalline water is a primary driver of fluid movement within the body. Conversely, I believe poor zeta potential is one of the primary obstacles to fluid movement in the body.
All of this raises three questions:
1. How do you appropriately support the formation of liquid crystalline water in the body?
2. How do you support maintaining a healthy zeta potential within the body?
3. What is the relationship between zeta potential and the formation of liquid crystalline water?
To best answer these questions, the third question must first be addressed.
Colloidal Stability and Zeta Potential
Note: much of what I am discussing on Zeta Potential in this article is a shortened version of my attempt to cover all its key details here.
When particles are placed in water, one of three things can happen:
•They don’t mix (e.g., oil floats to the top, sand sinks to the bottom).
•They dissolve (e.g., salt).
•They form a colloidal suspension (e.g., milk) where each particle is repelled from the other and evenly distribute themselves throughout the body of water they reside in.
In the case of colloidal suspensions, there are factors that cause colloids to come together (gravity separating things by weight, the inherent molecular attraction between objects [termed the van der Waals force], and electrical attractions). There are also factors that do the opposite.
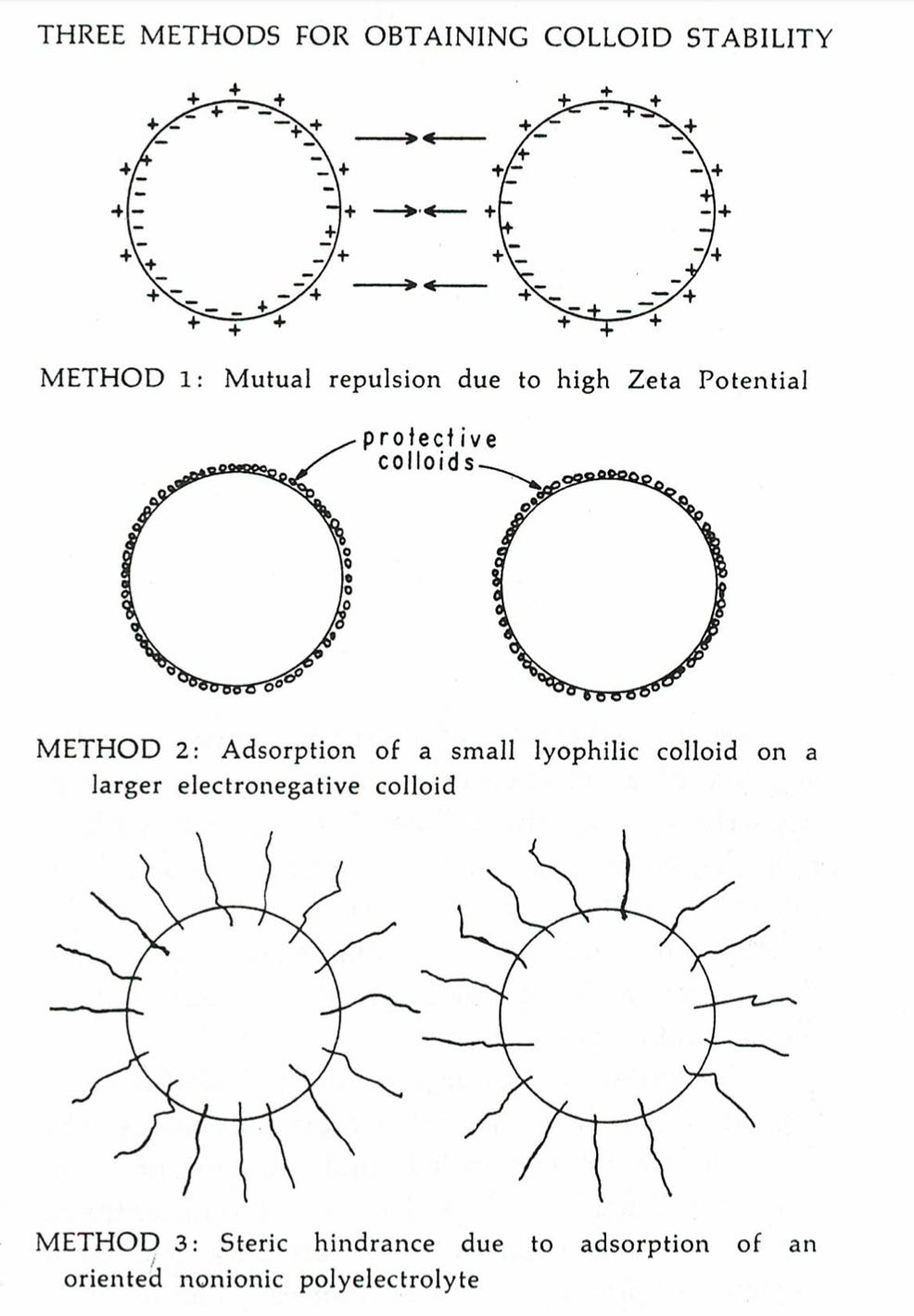
Note: steric hindrance’s effect on colloidal stability is discussed further here. Protective colloids will be discussed later in this article.
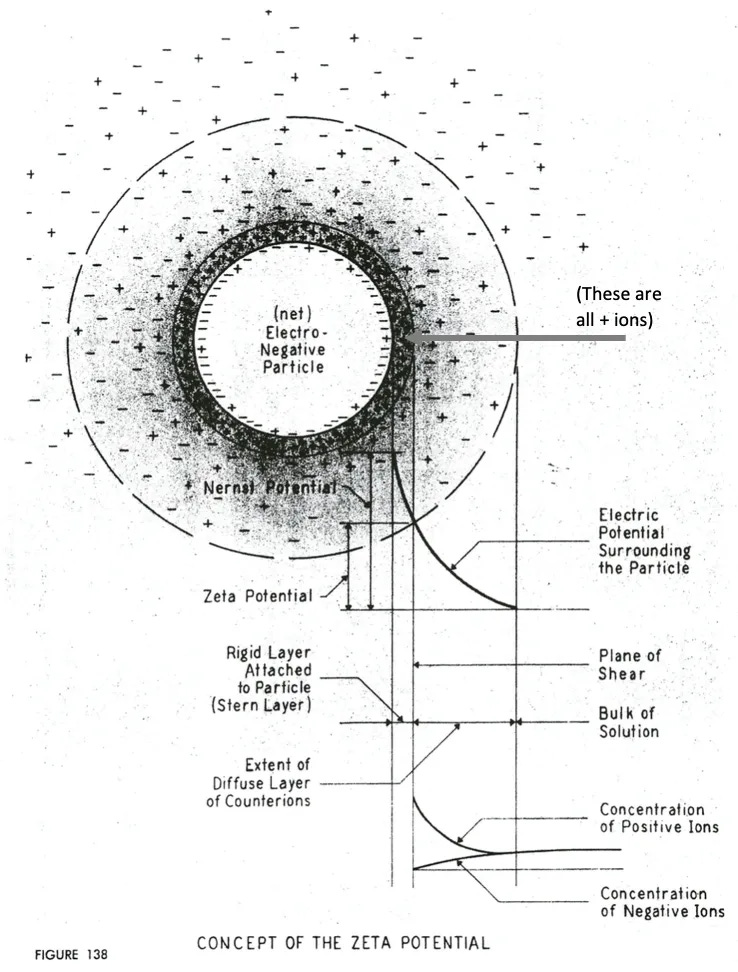
Zeta potential specifically refers to the charge difference between the water ions (that coat the charged ions) and the charge of the surrounding water.
Because electrical repulsion due to zeta potential is easier to control, it is typically (but not always) the factor focused on when trying to improve or decrease zeta potential. For example, aluminum is very effective at reducing zeta potential and is frequently used to separate organic matter from water in sewage plants or to clot wounds (additionally, its presence in vaccines likely accounts for many of their side effects). One of the key reasons I decided I needed to write on Substack was to help bring awareness to my realization that the spike protein is also a highly effective agent at destroying the body’s zeta potential and that this property explains many of the effects seen from the vaccine such as this:

Note: there are various other ways to observe decreases in zeta potential, such as using clinical signs or a specialized microscope to observe the motion of blood cells in the blood vessels (venules and arterioles) throughout someone’s eyes.
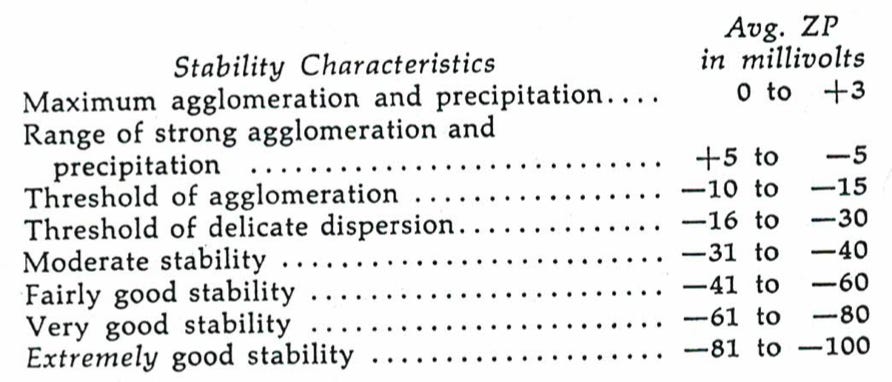
One of the most important things to understand about zeta potential is that when its repulsion is no longer sufficient to overcome the attractive forces in a colloidal system, it will clump together, initially in small clumps (termed agglomerations), and then as the zeta potential worsens, in larger clumps.
For reference, the normal zeta potential of a red blood cell is around -15.7 millivolts (although this number does vary a bit depending on the source). Additionally, as red blood cells age, they lose their negatively charged sialic acid, which in turn worsens their zeta potential.
Note: since zeta potential gets "better" as it becomes more negative, I cannot refer to that change as increasing "zeta potential" since there is ambiguity in what is being referred to (increasing typically refers to becoming more positive). For that reason, I always use words like "improve" instead. Additionally, for a positively charged colloidal system (these are much rarer), a more positive zeta potential would "improve" that system's colloidal stability.
Before we move forward, it is critical to understand that too much or too little colloidal stability in the body is not good. For example, we depend upon blood clumping together when a wound occurs to initiate the clotting process (as a leak from the blood supply decreases colloidal stability thereby crossing the critical threshold). We would likely bleed to death were that not to trigger the blood to begin clumping together due to a loss of colloidal stability (thereby allowing the full clotting process to initiate).
Conversely, if poor colloidal stability causes our blood to clump together within the circulation, many debilitating complications, including strokes of varying severity, can occur. Because of this, the blood naturally is calibrated to be just above the threshold of agglomeration and thus able to both clot when needed and become dispersed when that is not required.
Over the last 150 years, there has been a progressive decline in the health and vitality of the human species, which, as best as I can tell, began with the introduction of the smallpox vaccine. Similarly, we saw a significant decline in our health when the 1986 vaccine law removed the incentives to produce safe vaccines, and an ever-increasing number were given to our children. Likewise, an unprecedented decline in the health and wellness of the human species has been observed following the mass administration of the COVID-19 vaccines, that I fear, like those previous instances will become the new normal future physicians will be unable to recognize.
I have researched this question extensively and found various sources all corroborating this decline's presence. When I looked at the factors which appeared to be the most directly responsible, those I identified all shared the common thread of being results of living with modern technology, and many, I could make the case impaired the physiologic zeta potential of the body.
If coagulation is present in the venules and arterioles of the eye, there is every reason to believe that it exists in like degree throughout the vascular system. The writer’s [Thomas Riddick in 1968] observations with the horizontally-aimed stereoscopic microscope over a period of several years showed that significant coagulation existed in 40 to 50 percent of all persons examined. They were in a “normal” state of health—under no medical regimen—and in the 25 to 65 age bracket.
This is important because I believe that one of the fundamental issues our species now faces is that the zeta potential we evolved to maintain is no longer appropriate for the modern era. Previously, it would have created an appropriate balance between colloidal agglomeration and dispersion, but now since there are so many factors encouraging agglomeration, it is excessively tilted towards agglomeration, and for some individuals, those exposures are sufficient to cause serious illness. I suspect the variability in response is partly genetic (as there will be variation in the zeta potential each person’s physiology is innately set to). Still, since, to my knowledge, no research has ever been conducted in this area, I cannot provide evidence to support that assertion.
Additionally, much like there can be either an excessive or deficient zeta potential, you can also have excessive or inadequate liquid crystalline water. If, for example, the cells (which are predominantly liquid crystalline water) became fully liquid crystalline water, they would lose the vital channels that normal water freely flows through. I suspect, like poor zeta potential, deficient liquid crystalline water in the body is much more likely to be an issue than excessive liquid crystalline water—however, I have no way to prove this. That said, in this article, I will provide the examples I have come across where excessive liquid crystalline water does appear to be an issue.
Liquid Crystalline Water and Zeta Potential
The central question I’ve had throughout writing this series is, “what is the relationship between liquid crystalline water and zeta potential, and does improving one improve the other?” Since no one appears to have written on the subject, I am relatively sure some of what I am putting forward is incorrect, and a lot needs to be added to this.
Nonetheless, I’ve had a very strong feeling this is important to figure out, so the only thing I can do is put my best attempt forward to get the ball rolling.
Note: there are a variety of other descriptions for liquid crystalline water (e.g., it overlaps with the gel state water frequently is in throughout the body). In many cases, I will use research on those states as a substitute for liquid crystalline water and clarify when another term refers to the same concept.
Protective Colloids vs. Liquid Crystalline Agglomeration
I currently suspect that the existing zeta potential model is incorrect and that a much greater number of layers of water molecules may coat charged colloidal particles in water. Pollack, for example, has shown that particles in water can generate liquid crystalline water around themselves (which consists of hundreds of thousands of layers of water molecules), and in some cases, such as when high salt concentrations are present, a very high percentage of water present is in this form.
One of the three things that create colloidal stability is protective colloids (explained further here), which form hydrogels (clumps of liquid crystalline water) around them that coat colloidal particles and effectively create a barrier that keeps the particles separated. Since hydrogels are essentially the same as liquid crystalline water, this argues that much of the colloidal dispersion we observe is not a result of zeta potential but rather liquid crystalline water coating colloidal particles in the body and preventing them from clumping together.
Conversely, when excessive liquid crystalline water is present, the water is much thicker and viscous, something also associated with poor zeta potential. This is most likely due to the water itself being thickened, but it may also be due to it forcing colloidal particles present together (as liquid crystalline water does not permit them to be within it and thus pushes them to the regions it does not occupy).
Presently, I believe increasing liquid crystalline water most likely improves colloidal dispersion (which is why zeta potential ultimately matters). To my knowledge, the circumstances where excessive liquid crystalline water can exist and could thus do the opposite predominantly exist within cells, so an excess of liquid crystalline water should not be a common issue anywhere fluid is circulated throughout the body.
Note: within cells, the surfaces that create liquid crystalline water are very close together, leading to most of the water in cells being tightly bound together in this phase instead of free-flowing (a lot of research using a variety of approaches has confirmed this). Additionally, liquid crystalline water is often very tightly adhered to the surfaces it forms on. For example, paper (cellulose) typically contains 7–8% water; even several days in a dry oven cannot remove that water. Similarly, the liquid crystalline water found around cellular components will persist even when most of the water has been osmotically removed.
Negatively Charged Systems
One of the interesting questions about zeta potential is why in almost all colloidal systems that exist in nature, a negative charge is used to create the mutual repulsion between the particles rather than a positive charge. One potential explanation is that since biology shares a common evolutionary root, once something used a negative charge, everything else had to so it would remain compatible (this is similar to how in almost all [but not all] cases, the same reading system is used in all species to translate RNA to proteins).
This argument, however, does not address the colloidal systems found in nature that do not have an evolutionary origin but also rely upon negative charges for their colloidal dispersion. It should be mentioned that positively charged ones do exist and can also artificially be made with positive charges; they just are rarer.
Similarly, with exclusion zones, they can form on both positively or negatively charged surfaces. However, the vast majority form on negatively charged surfaces and have a negative charge, while those that form on positively charged surfaces are much smaller and much more easily dispersed.
Consider the arithmetic. Cells make up some 60% of your body’s mass, and they are negatively charged. Extracellular tissues such as collagen and elastin are next in line, and those proteins bear negative charge and adsorb negatively charged EZ [liquid crystalline water]. Only some of the smaller compartments are positively charged with protons (low pH), and they commonly expel: urine, gastrointestinal system, sweat, and expired air (containing hydrated CO2 or carbonic acid).
Note: The constant elimination of positive charges is necessary to sustain our negatively charged physiology. This may help explain the benefits of many holistic practices that augment one of these roots of elimination and why their cessation (e.g., severe constipation) can rapidly cause so many issues and rapidly improve the individual once they are addressed.
Within the body, most of the proteins and cell surfaces that contact fluid systems in the body (e.g., the blood) carry a negative charge which causes them to repel each other and, in most cases, not stick together. It is not only the repulsion of the negative charge of the proteins (and cell surfaces) that creates this effect but also the repulsion from the negative charge created by the liquid crystalline water, which forms on the negatively charged substance. Additionally, as mentioned before, I also believe the liquid crystalline water functioning as a protective colloid (as nothing can move through it) plays a critical role in these systems being able to maintain their colloidal stability.
To further quote Pollack:
Structural proteins such as actin filaments, microtubules, intermediate filaments even DNA are all negatively charged. Cross-linkers, by contrast, are positively charged. These include bridging and bundling proteins, as well as divalents. All of this seems to make sense but then again, why is it that the polarities are not reversed? Why couldn't the structural proteins be positively charged and the cross-linkers negatively charged.
Note: the primary exception I know of to this rule, as shared by Pollack, is when positively charged ions (e.g., metals) are used to “break” the liquid crystalline layer of water covering one part of the cell so a channel for things to enter and exit the cell can exist there.
Lastly, Pollack designed a simple experiment to determine if a small charge (in this case, a few volts) might generate liquid crystalline water and if this energy could be stored and harvested later (in other words functioning as a battery):
To determine what might take place during this charge transfer, we added pH-sensitive dye. Something did happen. Near the cathode, the color change indicated high pH; near the anode [the negatively charged electrode], it indicated low pH [which indicates the presence of liquid crystalline water]. The difference was easily six pH units — a proton concentration difference of a million times.
Similarly, it has been shown that Earthing (a practice that introduces the earth’s negative charge into your body and many people have benefitted from) significantly improves the zeta potential of the blood. When I first learned about Earthing, I realized most of the benefits attributed to it reflected a partial restoration of zeta potential (which has since been proven, although I believe there are more effective ways to introduce negative charges to the body). Similarly, I have found COVID-19 vaccine-injured patients frequently improve somewhat from adopting the practice of Earthing. Additionally, in the one instance where it was studied, Earthing was shown to significantly benefit patients with COVID-19.
Note: I have been unable to find any studies showing Earthing increases liquid crystalline water, but Pollack did state in an interview that this occurs.
All of these points regarding negative charges, like the previous ones, again argue there is an inseparable interrelationship between zeta potential and liquid crystalline water and that it is possible the effects of one are being mixed up with the other.
pH
At any given moment, positively (H₃O⁺) and negatively (H1O-, typically written as OH-) charged forms of water exist. If far more positively charged H₃O⁺s are present, the solution is considered acidic, while if negatively charged OH-’s predominate, the solution is considered alkaline.
The degree to which either is present determines how acidic or alkaline a solution is and is designated with pH. The balance between the two, in turn, is primarily determined by the number of positively charged hydrogen atoms (H+), present. If these are in excess, they will be more likely to combine with H2O to form H₃O⁺ rather than combining with OH- and having it become H2O.
Since the (negatively charged) liquid crystalline water kicks out H+ (a proton) during its formation, the positively charged protons remain in the vicinity of the liquid crystalline water, creating an acidic and positively charged layer immediately adjacent to the liquid crystalline water. Using the same logic that a negative current would build the exclusion zone, Pollack also predicted an alkaline environment (which has more negatively charged OH- molecules) would favor the exclusion zones formation:
That balance can shift as ambient conditions change. In acidic water conditions, the ample hydronium [H₃O⁺] ions in bulk water should continually chip away at EZ [liquid crystalline water] mass, tilting the balance towards a smaller EZ. We have confirmed this experimentally: sufficiently acidic pH does diminish EZ size. Salts erode the EZ similarly. Consider NaCl: While the Cl– component can combine with H3O+ in the bulk to yield HCl + H2O, the positive Na+ can invade the negative lattice, and go on to create NaOH by extracting a lattice OH– unit. The EZ erodes and adds a water molecule to the bulk water. Wherever the lattice is open, positive ions of any sort can enter and cause EZ erosion.
Similarly, in most cases, Riddick found that acidity worsened zeta potential while alkalinity improved it. The primary exception was at extreme pHs (1-3 and 12-14), which destroyed the zeta potential in both cases. Concurrently, he found that agents which created alkaline pHs also improved zeta potentials and that positively charged agents (which worsen zeta potential) would decrease (acidify) the pH in tandem, making the zeta potential more positive.
Riddick’s most interesting observation was that many systems with biological colloids, at around a pH of 4, would flip from a positive to a negative zeta potential. This is because many amino acids, and hence the proteins they create, switch from being positive to negatively charged around this pH. Since the body relies on a variety of proteins to function as stabilizing colloids (e.g., albumin), this means that the zeta potential of many systems will become negative between a pH of 5-10.
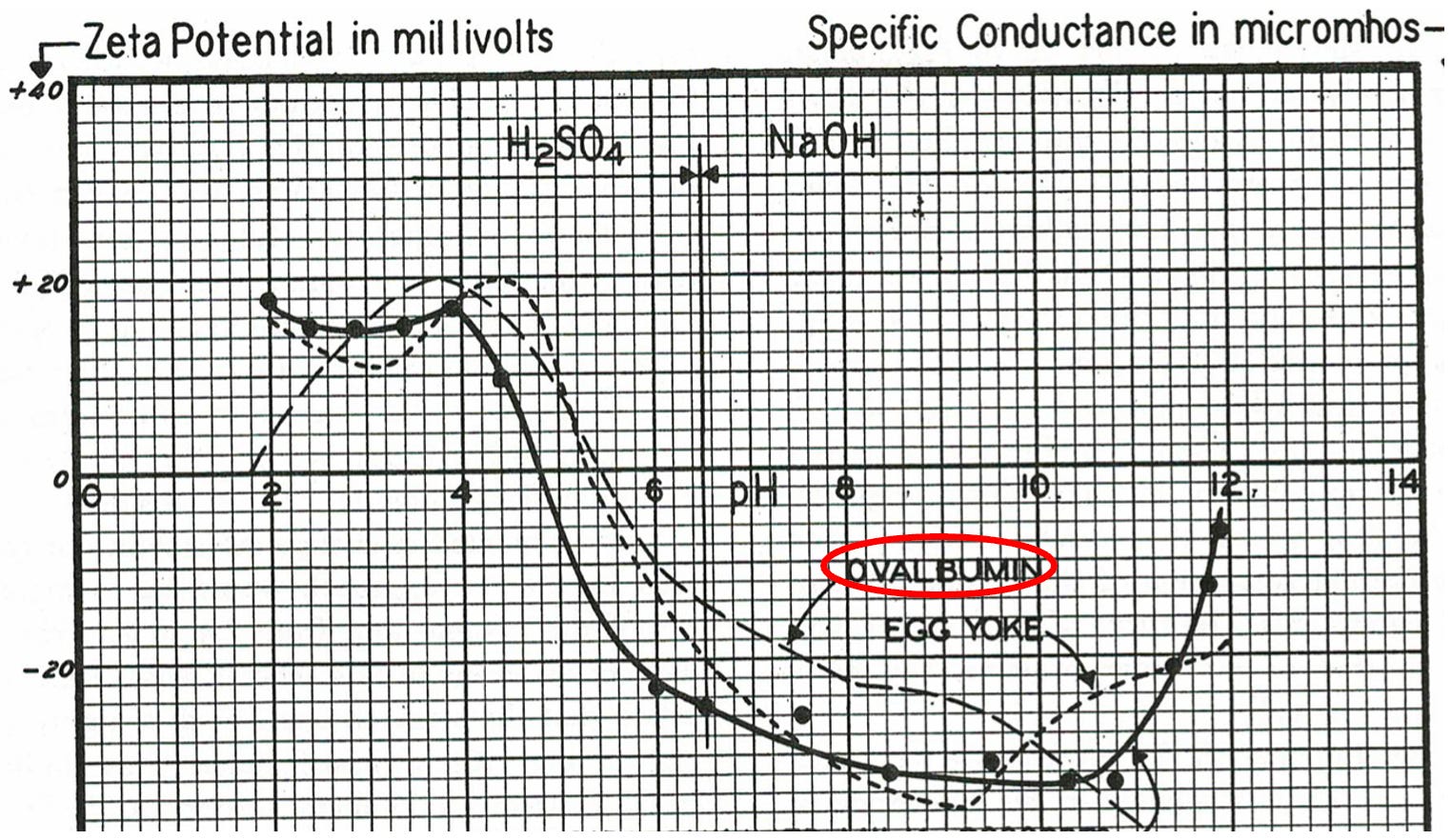
Note: 55% of egg white is ovalbumin, a protein similar to albumin. Since it was not feasible to obtain large quantities of human albumin at the time Riddick conducted his research, he frequently utilized ovalbumin.
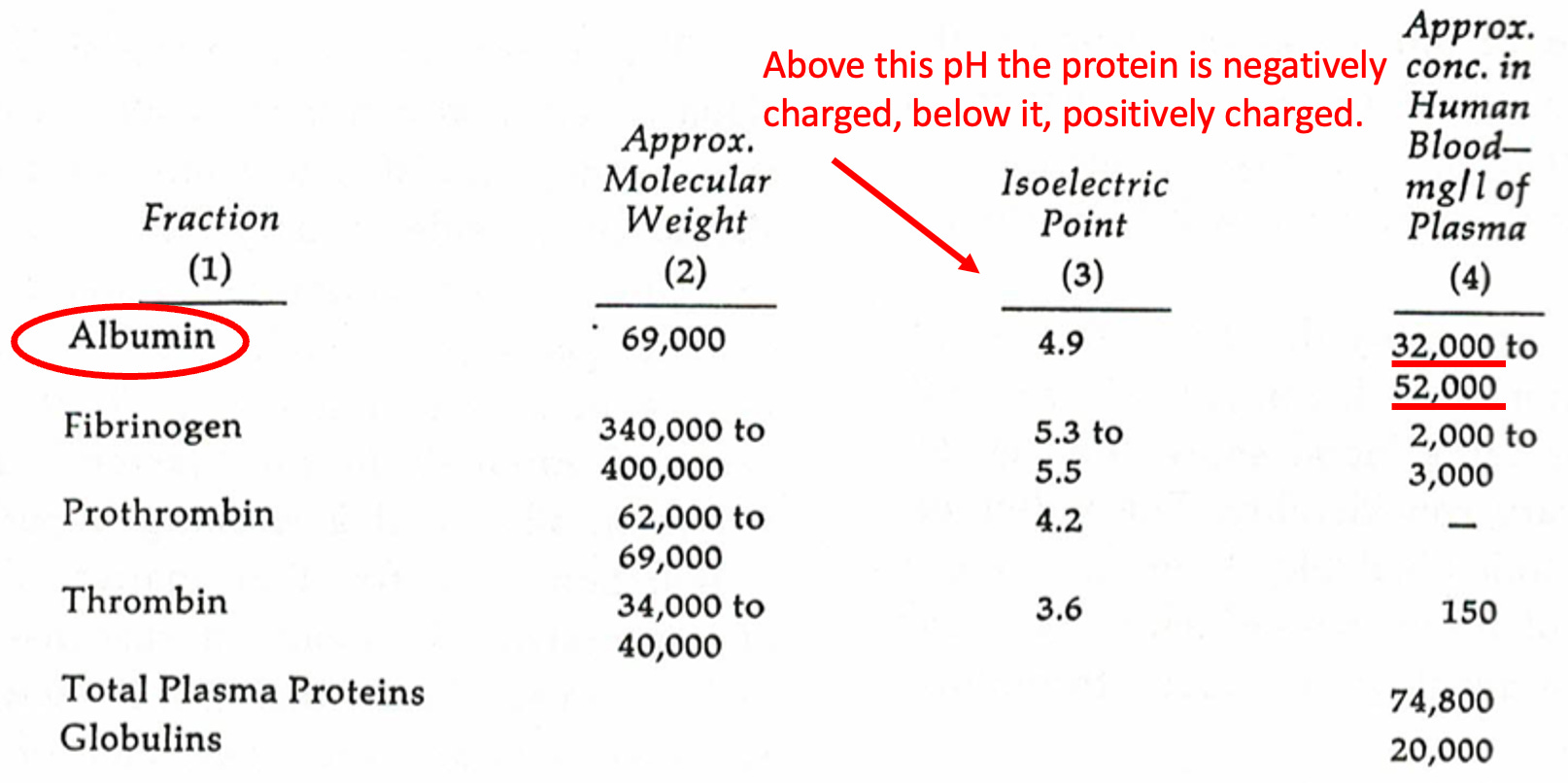
Note: This table illustrates why Riddick put so much focus on the stabilizing colloid albumin/ovalbumin (which he also showed significantly improved colloidal stability in situations that would otherwise have significantly impaired a systems zeta potential).
Temperature
Note: the physician who pioneered much of the work in zeta potential felt very strongly about not icing injuries as this would create colloidal clumping in the fluids at the site of injury, prolong the recovery, and potentially give rise to other issues. Chinese medicine has a similar perspective here (which is discussed in relation to cold creating blood stasis). The medical field always goes back and forth on if you should ice injuries—I do not personally support the practice.
Both the formation of liquid crystalline water (particularly the flow it generates) and the lack of obstruction to that flow (impaired zeta potential) are critical for a variety of physiologic circulations. Since the brain performs most of its vital lymphatic drainage during deep sleep, it may provide some valuable clues for the temperature question:
As mentioned above, the brain tissues are extremely sensitive to temperature deviations, and the physiological thermostat is able to hold the brain tempera- ture stable within about 0.1◦C. At the same time, during sleep the physiologically controlled oscillations of the brain temperature are considerably larger (from 0.3 to 3.5◦C in different animals), being the lowest in the “quiet” sleep and the highest (close to the temperature in wake state) in the “active” sleep (Cain et al., 1994; Parmeggiani, 1995; Fuller et al., 1999; Pastukhov et al., 2001). What is the reason of such high temperature alterations during sleep?
Pollack has made an excellent case that many functions in the body (e.g., muscle contractions or nerves firing) depend upon the controlled formation and disassembly of gels (which are essentially liquid crystalline water) and are a focus of the second part of this series. The transition from water being in a normal state to a gel happens very abruptly once a variable (e.g., temperature) in the system reaches a critical threshold, at which point the entire transition abruptly occurs. In all cases, a lower temperature correlates with the gel state, while a higher temperature correlates with a liquid state.
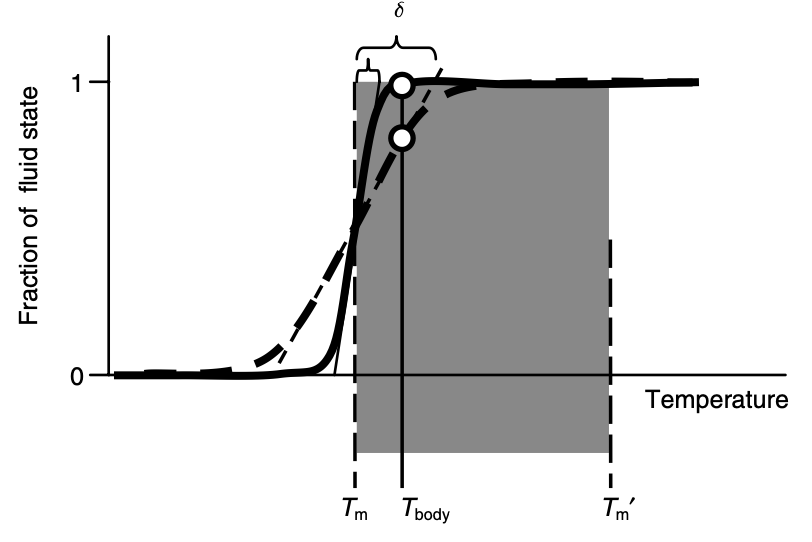
This property has led Thomas Cowan to theorize that a critical role of fevers is cause liquid crystalline water within cells to enter a liquid state and thus detoxify the body. I am unsure how this could be determined, but in an interview with Pollack, Pollack stated he thought this was the case (that fevers cause liquid crystalline water to become regular water) but added that it is difficult to model precisely what happens as temperature increases. Per my understanding, this is because infrared energy (which creates heat) creates the greatest growth of liquid crystalline water, but as liquid crystalline water becomes hotter, it becomes more unstable and likely to break apart.
Note: the book that the fever concept was discussed in also highlighted that one distinguishing characteristic of cancer cells appears to be their relative lack of liquid crystalline water.
Conversely, it is also well known that water has the highest density at 3.98°C (a few degrees above freezing), likely because this temperature is also where the greatest amount of liquid crystalline water is present. Similarly, Pollack has experimentally confirmed that over temperatures ranging from 0 to 30 °C, reducing water temperature increases the size of the liquid crystalline water present.
Hofmeister Series
Any protein can exist either in its standard form (which many, myself included, view as a result of the protein being a suspended colloid) or in a denatured (abnormal) form, which often correlates to it no longer being colloidally suspended. The process of cooking egg white is an excellent example; raw egg white is transparent and has a viscous fluid quality, while cooked (denatured) egg white is white and solid. Heat is not the only thing able to denature proteins; charged ions can too.
Note: At this time, I believe the spike protein’s positive charge (along with its prion-forming domain) plays a significant role in its association with protein-misfolding diseases, such as various neurodegenerative conditions and unusual fibrous blood clots. Conversely, ATP’s negative charge stabilizes proteins (some also believe this effect comes from ATP’s adenosine). In turn, decreasing ATP levels have been found to correlate with the appearance of neurodegenerative diseases (thus leading to this being explored as a therapeutic option). Additionally, melatonin appears to be able to create a similar effect to ATP. However, given that the vaccine spike protein also contains a prion-forming domain and that mitochondrial dysfunction is also associated with declining ATP levels, other potential explanations exist too.
Researching this process 135 years ago, Franz Hofmeister produced a series of cations and anions (both are required to create a compound) he ranked by their relative ability to stabilize or denature proteins. Currently, the reason the Hofmeister series exists does not appear to be fully understood, and there are some minor variations in how sources present the series. This was one I found in a textbook:
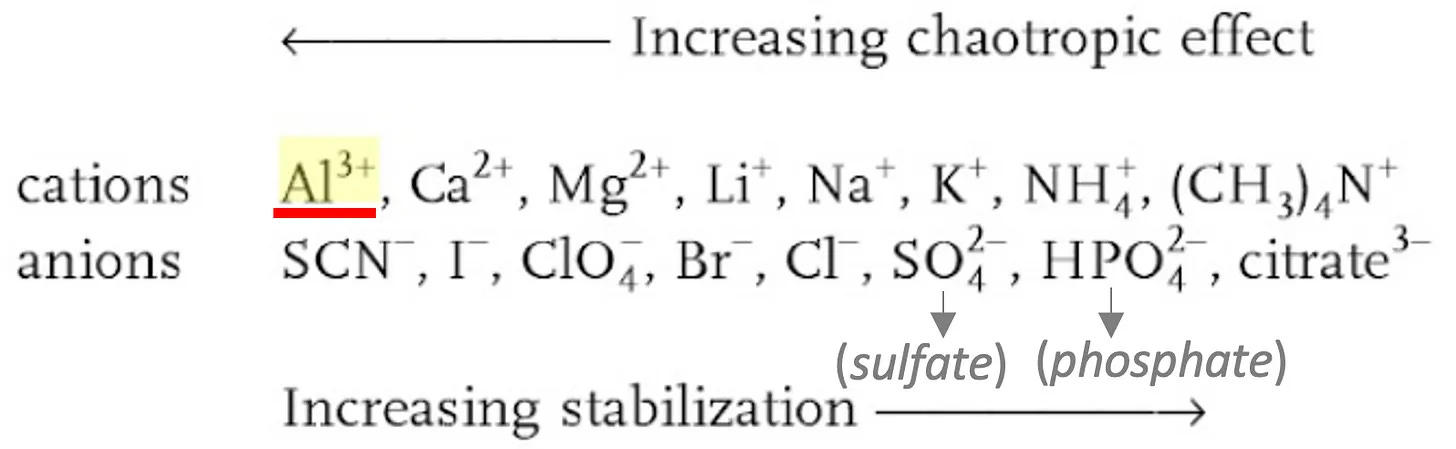
When I came across this series, it was immediately evident from looking at this list that it matched the influences of cations and anions on zeta potential:
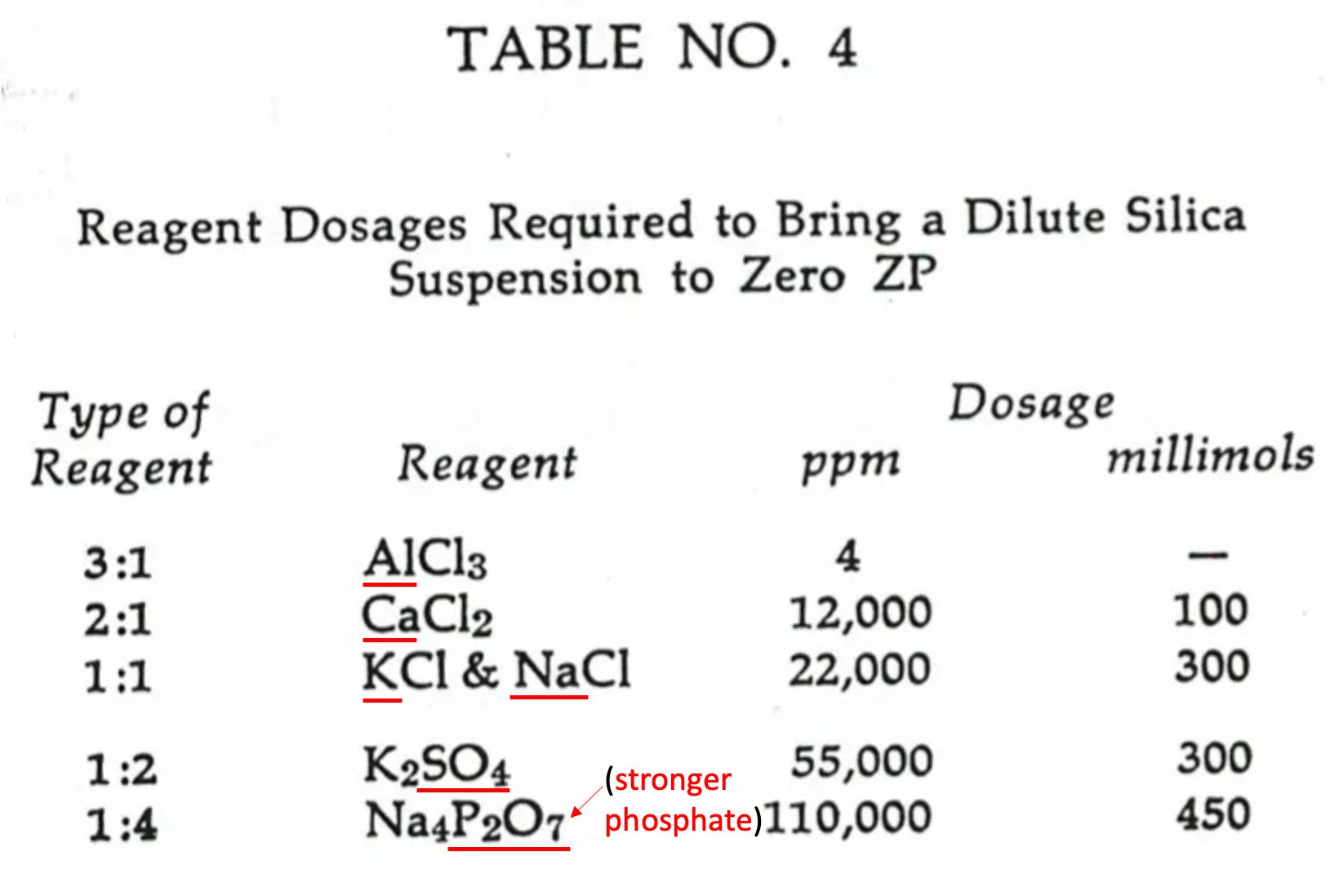
Note: negatively charged ions will switch from improving zeta potential to worsening it at high enough concentrations. Other ions matching the Hofmeister series will also be presented in the next section. One of the major issues with applying the Hofmeister series to understanding zeta potential is that the “Hofmeister effect” reverses depending on the charge of the ion (positive verses negative), so it is much more instructive to consider if the ion is on the left or the right of that series rather than if it is labeled as a kosmotrope or chaotrope.
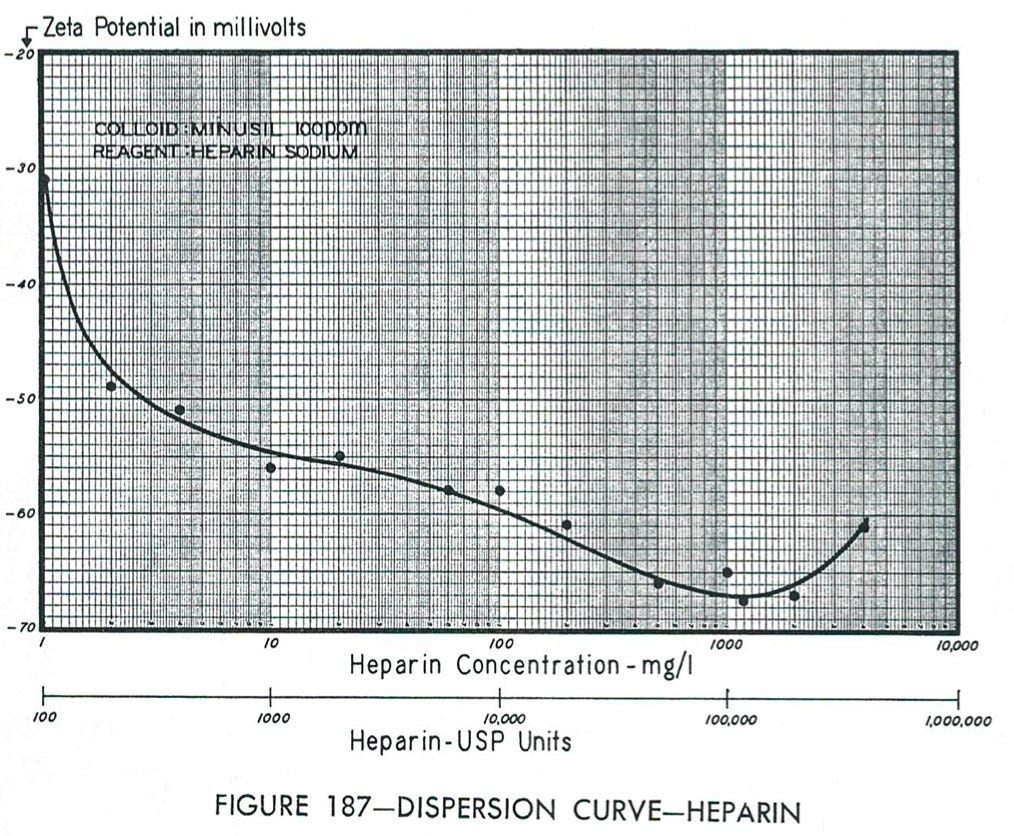
Note: Stephanie Seneff has made a strong case that the body relies upon the production of sulfates (which is frequently disrupted) to maintain zeta potential throughout the body and generate liquid crystalline water where it is needed. Heparin is a highly sulfated molecule (and has the highest negative charge density of any biological molecule) and is both one of the most frequently used anticoagulants and also a highly effective agent for improving zeta potential.
When I reviewed Pollack’s work with the transitions of gels to liquid water (which typically contain colloidal suspensions and thus leads to this also being called the gel-sol transition), I noticed another interesting correlate.
Pollack’s physiologic model (which I find incredibly compelling and well supported by the evidence he has presented) strongly emphasizes the gel-sol transition. Because certain physiologic functions, such as a muscle contraction or the propagation of a nerve impulse, require the transition to be abrupt and instantaneous, some controllable mechanism is required to move the system above or below the critical threshold that initiates the phase change.
What Pollack (and others) found was that the same ions (chaotropes) that tend to collapse zeta potential also transition a gel to a sol, while the ions (kosmotropes) that restore zeta potential also restore the gel state.
Note: Pollack has stated this occurs because the ions on the left of the Hofmeister series (the chaotropes) have the largest hydration shells (thereby making them absorb poorly). In contrast, those on the right have the smallest hydration shells (thereby making them easily absorb). The smaller ones (e.g., potassium) thus are favored for entering dense structures like liquid crystalline water and, once available, will displace the larger ions attached to proteins. While this explains many of the observations on this subject, I am unsure if this explanation adequately explains some of the observations I have made from studying this entire subject.
Since the body does not contain aluminum, calcium (Ca2+) is the positive ion it uses instead. Many bodily functions are linked to the influx of calcium ions (e.g., muscle contracting, nerve firing, or programmed cell death). Although mechanisms exist to explain why calcium ions “work” in each place their influx triggers a physiologic response, Pollack has noted that a gel-sol transition would mediate this change.
Numerous models, in turn, have been created that show that varying the environmental concentration of calcium can cause various proteins and gels to lengthen or contract in a fully reversible manner that is independent of ATP or pH and often generates a large amount of force in the areas that contract. This process also provides a mechanism to explain the motion of many microorganisms. Furthermore, in some cases, NMR spectrometry has demonstrated this.
Conversely, ATP (a molecule composed of three phosphates, which are one of the most effective agents for both stabilizing colloids and increasing zeta potential) appears to be able to directly affect cells by its presence creating liquid crystalline water (whereas in the conventional model, ATP’s function is to be broken apart for energy). In Pollack’s model, ATP’s role in muscle contractions comes from it causing the gel state (liquid crystalline) water to reform in a muscle so the muscle expands and, therefore, can contract again. This Pollack also argues is why when ATP disappears at the time of death, the muscles become locked in a tightly contracted state known as rigor mortis.
Note: As early as 1947, it was observed in blood cells that gels of hemoglobin formed “crystals” of 50% water, which appeared to be in ordered layers. Later research showed most of the water with a blood cell’s cytoplasm is not in the liquid crystalline state—except that immediately surrounding hemoglobin. For red blood cells to function, they need only to release oxygen where it is needed, which in turn requires hemoglobin’s affinity for oxygen to change depending on the current environment. ATP plays a role in this process, as it can alter hemoglobin’s affinity for oxygen. Still, since it does so without having a binding site on hemoglobin itself, Pollack argues this suggests ATP does so by directly altering the liquid crystalline water present in the red blood cell.
The Hofmeister series also appears to explain the effects of different ions on nerves. For context, this is a process Pollack and others argue is due to structural phases transitions of liquid crystalline water:
The cortical gel layer of nerve fibers has the properties of a cation- exchanger. Hence, this layer can, and actually does, undergo a reversible abrupt structural change when monovalent cations (e.g. Na+) are substituted for the di-valent counter-ions (e.g. Ca2+). This structural change brings about a sudden rise in the water content of the layer which in turn produces a large enhancement of cation mobilities accompanied by a shift of ion-selectivity in favor of hydrophilic cations. Based on these grounds, it is argued that the electrophysiological processes known as “nerve excitation and conduction” are, basically, manifestations of abrupt structural changes in the cortical gel layer. In recent studies, we have shown that several aspects of the excitation phenomena can actually be reproduced by using synthetic polyanionic hydrogels in place of living nervous tissues.
Since the following passage about nerves is a bit technical, you may want to skip it. It provides another example of how the Hofmeister series determines an anion’s ability to form liquid crystalline water:
The linkage between cytoskeletal integrity and excitability implies that action potentials could be impacted by most any agent that solubilizes gels. Consider the following. When axons are internally perfused with KCl, action potentials will wane progressively and vanish within 25-40 minutes. This decline is impacted in a telling way by ion substitutions (Tasaki et al., 1965).
If fluoride replaces chloride during the period of decline, action potential amplitude is promptly restored. Bromide substitution accelerates the decline. Examination of a large number of an ions showed that restoration efficacy followed the classical Hofmeister series (von Hippel and Wong, 1964). Thus, F > HPO > glutamate > SO4 > acetate > Cl > NO > Br >I > SCN. The anions toward the left had the highest tendency to restore action potential amplitude, and the most stabilizing. Those toward the right most strongly hastened action-potential decline and have the highest tendency to solubilize.
Note: In normal, untreated axons, when the existing cytoskeleton is further stabilized by agents such as Taxol or DMSO, excitability is also enhanced. Additionally, this Russian study found that the negative electrical potential of a gel decreased after its volume decreased after a phase transition was induced by the same ions which trigger nerve cells to fire in the body, further supporting Pollack’s proposed model.
U-Shaped Curves
One critical concept to understand regarding zeta potential is that agents that affect it follow a U-shaped curve. So initially, their addition will move the zeta potential upwards or downwards (depending on their charge), then the effect will flatline at some point, after which the effect will reverse. Because of this, it is essential not to overuse any of the agents, as if you give too much of one, it will have the opposite effect you aimed for.
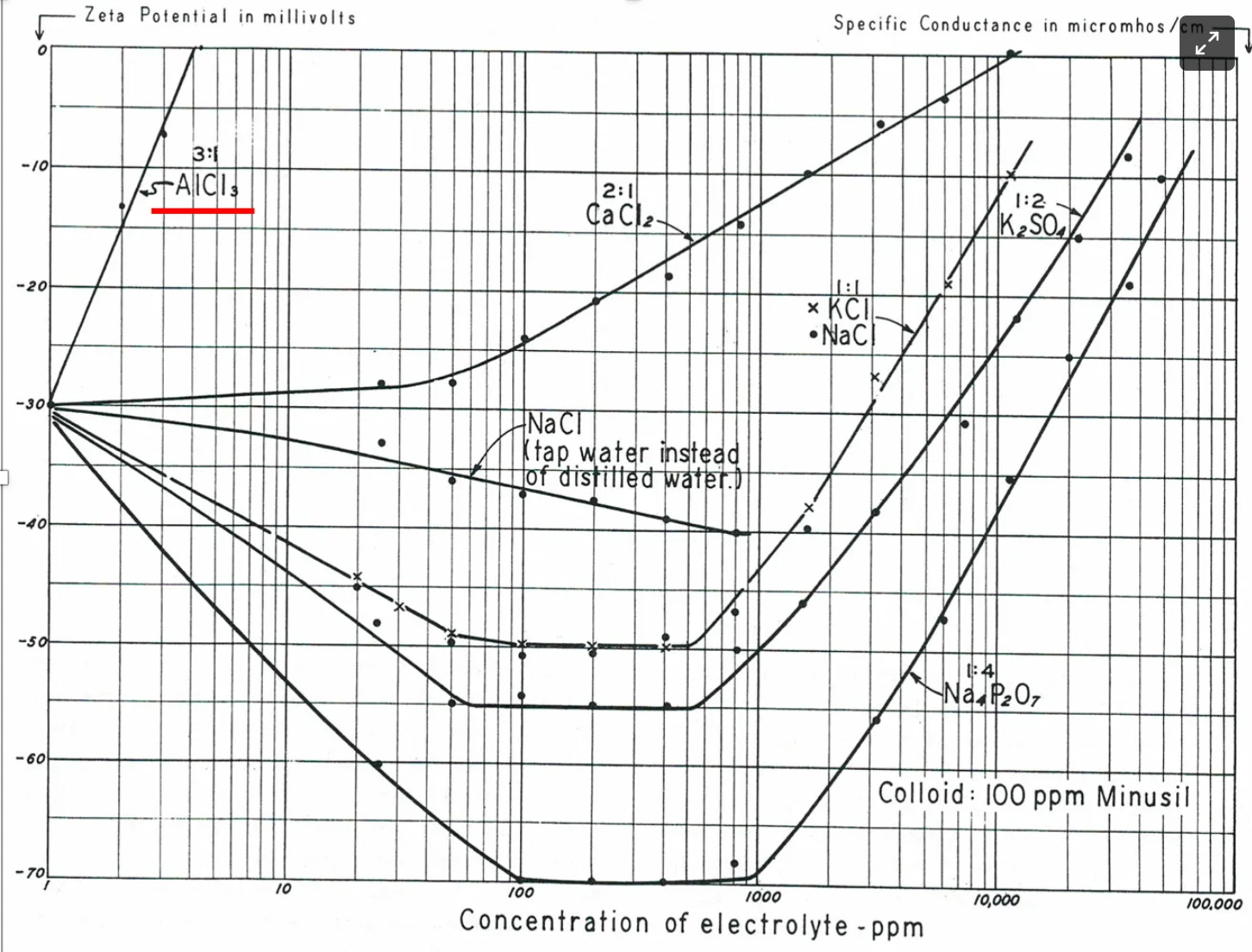
Note: this graph, when viewed in conjunction with the Hofmeister series, explains a great deal about how some of the approaches for addressing zeta potential were created. Both the cation and anion in each compound influence its effect on zeta potential, but frequently the influence of one is dramatically larger than the other.
As I looked through the existing data evaluating the effect of various things on the changes in the size of exclusion zones (which represent the amount of liquid crystalline water present), I noticed a similar U-shaped curve emerge. For example, consider the results of this study that evaluated adding ethanol (a common alcohol) to water and this study that assessed how adding ethanol changed zeta potential:
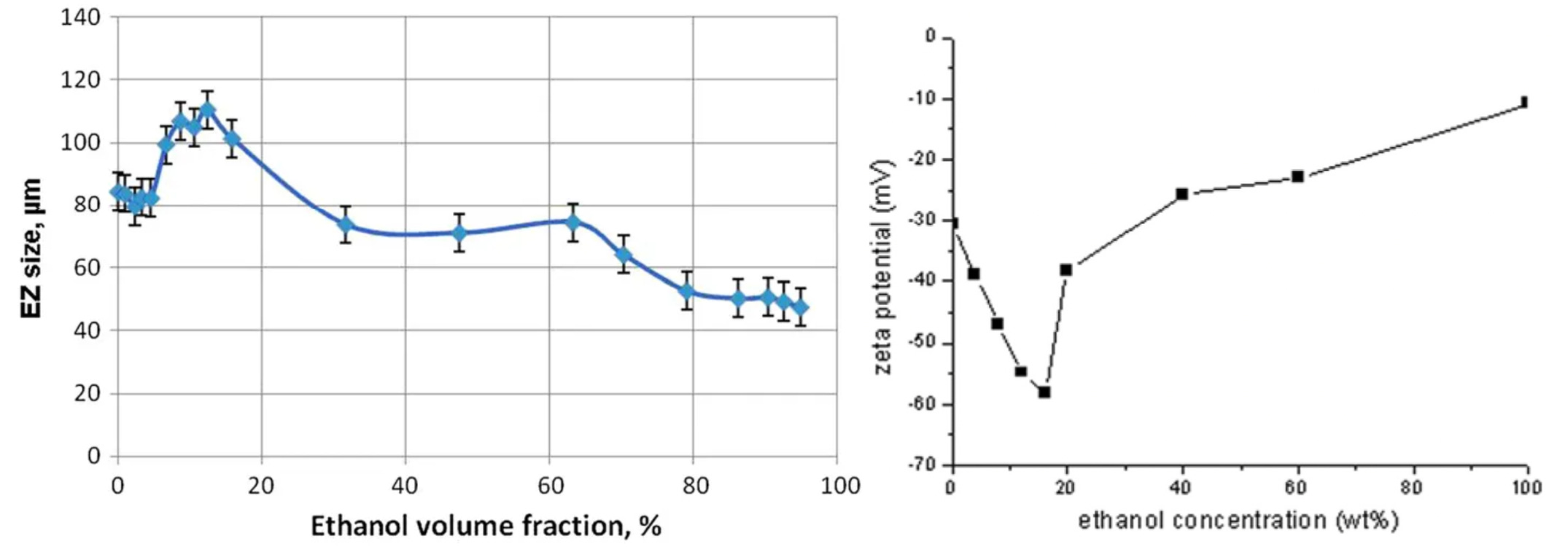
Note: exclusion zones (characteristic of liquid crystalline water) have been observed in other polar liquid such as DMSO and ethanol.
Similarly, this study attempted to evaluate if things thought to be “good for you” affected the amount of liquid crystalline water present (under the logic that the degree of liquid crystalline water formation could thus be used to assess “how good” something was for you). In each case, you will notice that the substance initially has a positive effect, but as more of it is added, the effect reverses:
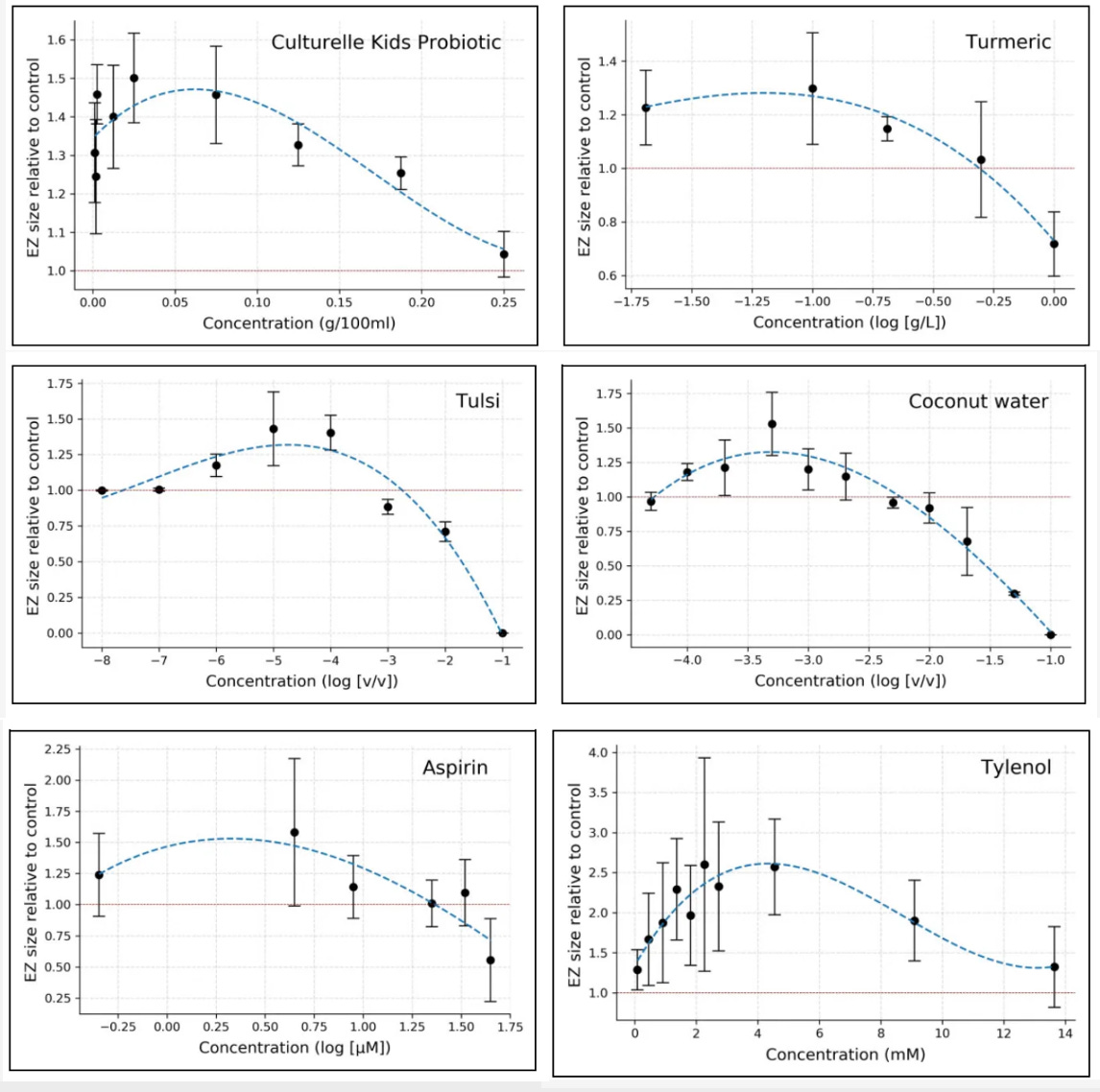
Note: Unlike the authors, I do not believe aspirin or Tylenol are “good for you.” Additionally, the case can be made that certain anticoagulants (sodium citrate, heparin, aspirin, EDTA) work by improving zeta potential. In the case of aspirin, this occurs because it acetylates a variety of molecules. Since acetyl groups carry a negative charge, each acetylation effectively imparts a negative charge to the compound, thereby improving its zeta potential.
There was one other finding in this study which I also feel I should share as it potentially contradicts some of the ideas put forward here:
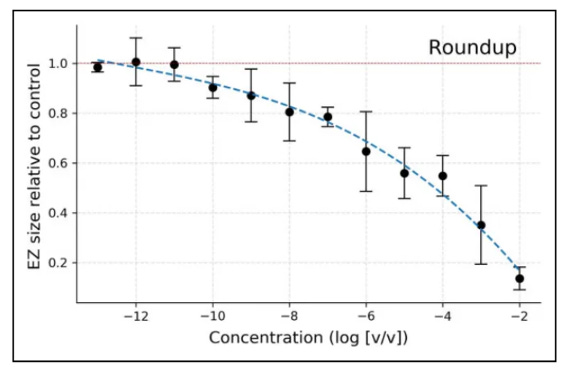
Roundup, a toxin also known as glyphosate, has a (weakly) negative charge, and due to its phosphate groups, has the characteristics of something I would expect to improve zeta potential. However, as the study shows, it neither improves the production of liquid crystalline water nor follows a U-shaped curve—although it may have done either had even smaller concentrations of it been measured.
Conclusion:
The physician whom Riddick trained, who pioneered the work on zeta potential, believed that poor zeta potential (likely due to declining renal function as the kidneys play a critical role in maintaining zeta potential) was the primary cause of aging. He was highly particular about adhering to a lifestyle that protected one’s zeta potential, and I can attest that both his patients and the doctor himself could maintain their functionality and cognitive faculties much later in life than their peer group.
Looking at the aging question, I have also felt zeta potential plays a pivotal role. This is partly because many of the diseases the elderly are vulnerable to (e.g., poor blood supply to the brain or becoming hospitalized from a respiratory infection) result from a poor zeta potential. It is also because I notice that as people’s bodies age, they tend to dehydrate, which causes much of the turgor, resiliency and flexibility we take for granted to disappear as the aging process progresses.
From researching this piece (thanks to a paper by Stephanie Seneff), I discovered that the dehydration I’ve observed has actually been proven to be a consequence of the body losing a significant portion of the liquid crystalline water within it:
This mini-review article is focused on publications devoted to the changes in water binding energy and content of bound [liquid crystalline] water in biological tissues during aging processes, when bound water lost from the hydration layer becomes free water. Bound water is released during cataractogenesis. In skin, water bound to proteins and other biomacromolecules becomes more mobile with increasing skin age. Extracellular to intracellular water ratio increases with age and was associated with muscle cell atrophy. Bound water concentration decreases with age in hydrated human bone and can be correlated with the strength and toughness of the bone. Higher fraction of free water in malignant tissues compared to normal tissues was observed. Hydration water mobility is enhanced around tau amyloid fibers. Water plays a decisive role in amyloid formation as entropic driving force. In the natural aging processes dehydration and glycation may be considered as subsequent steps.
Note: If you read part two of this series, which discusses the structural effects of liquid crystalline water, the above passage will make much more sense. Additionally, many of the themes in this passage (especially the correlation between the phase of water and the development of protein misfolding diseases like Alzhiemer’s is explained in much more detail within this paper).
One of the diseases of the modern era is "accelerated aging," which is often quantified by someone's "chronological age" (how old they are) versus their "biological age" (what age does the health of their body match). As you might expect, various causes have been proposed for why this happens (e.g., inflammation or mitochondrial dysfunction).
One of the most concerning side effects I have seen from the COVID-19 vaccines is the rapidly accelerated aging the vaccines cause (e.g., I've lost track of how many people have told me they felt like the vaccine aged them by 10+ years). While this is tragic, I believe it may also shed some clues on what causes this process (e.g., the spike protein is one of the most inflammatory things I have encountered in my medical career).
One of the most distinct characteristics of spike protein vaccine injuries is their damage to the cardiovascular system. Beyond heart issues (e.g., myocarditis), both large and small clots form (which I believe to some degree to be a consequence of poor zeta potential). Most importantly, significant damage occurs to the endothelial lining of the blood vessels, which in my opinion, is what most directly links the spike protein vaccines to accelerated aging.
The central question I sought to answer when I began this exploration is if the spike protein's disruption of zeta potential exists concurrently with the spike protein destroying liquid crystalline water in the body. I initially suspected this was the case because of how easily it (or its mRNA lipid nanoparticles) was penetrating the glycocalyx (the protective layer over the endothelium, which is largely liquid crystalline water).
Based on the other points I have discussed in this article and the high positive charge density of the spike protein, I believe this is the case and something that must be considered when evaluating the spike protein's toxicity. I also think there is a strong interrelationship between zeta potential and liquid crystalline water and that many things affect both in a similar way. However, with my current understanding of the subject, I do not believe they are similar enough to assume an agent will have the same effect for both, and in some cases significant differences will occur.
This series, starting with my initial summary of Andrew Moulden's work that explains why clinically detectable microstrokes are a common sign of vaccine injury, has been a lot of work to write (i.e., I have read well over ten books and many articles, such as all of Pollack's works). Presently, there are a few important loose ends on this topic I need to tie up (and that I sincerely wish to write about). They are as follows:
•Calcifications within the body (e.g., bone spurs or kidney stones) and how they can be directly treated by approaches that focus on restoring zeta potential and thereby disperse the calcifications.
•A summary of The Ion Effect, which is both fascinating and ultimately a consequence of zeta potential.
•A detailed review of the earlier research on blood sludging.
•A detailed review of blood stasis in Chinese medicine and its correlations to the themes throughout this series.
•A discussion of how information can be conveyed in biological systems through patterns in exclusion zone water, Luc Montagier's research into information storage within water near the end of his career, and how zeta potential collapse activates the immune system.
•Periodic discussions of conditions linked to impaired zeta potential or deficient liquid crystalline water (e.g., this is a common issue for wounds that will not heal and I now believe many skin conditions result from this occurring within the interstitium that underlies the skin).
However, since an article for each will take a long time, I deferred completing those articles so that I could complete the next and final article in this series.
At this point, I believe a key mechanism behind many different "holistic" therapies is their ability to improve the zeta potential of the body. The final article covers all the methods I know that can improve zeta potential and those which appear to increase the presence of liquid crystalline water in the body. Some of those methods and their theories are explained here, while others will be covered in the final installment. I thank you for the time you have taken to read this and help me to bring attention to this forgotten side of medicine.
How to Improve Zeta Potential and Liquid Crystalline Water Inside the Body

In this series, I have attempted to explain the vital importance of liquid crystalline water and zeta potential throughout the body—something I have greatly emphasized since I recognized their disruption appears to be a key component of spike protein vaccine injuries. One of the most common questions I, in turn, receive is, “What can be done to fix this?”
Wonderful piece...I won't claim to fully understand it, but LOVE how you're connecting all these dots. Part way through, I started thinking about grounding/Earthing, and was happy you mentioned it... When I clicked on the link to the study, I cried... My father, who passed away in June 2022, was one of the authors - Dr. Sinatra. He was so intellectually sparked by the connection between grounding and zeta potential. It was heartbreaking to lose him and I miss his intellectual curiosity and intuitive insights. I'll try to find email addresses for the other authors and send them this article.
There's only one COVID-19 and grounding study that I know of - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9381424/ - perhaps it will be of use?
I hope you keep up your amazing (and undoubtedly time-consuming) work! When I read it, my faith is strengthened that brilliant, ethical, brave and good doctors are still out there - please keep shining your light, and thanks for making my day!
Thank you for this important article. I'm gradually coming to see value in what I only recently dismissed as quackery. This morning I was alerted by Dr. Mobeen Syed (Youtube) to this paper:
https://www.nature.com/articles/s41541-023-00661-7/#Abs1
"Risk assessment of retinal vascular occlusion after COVID-19 vaccination"
which shows some alarming risks from the mRNA vaccines even years after administration.