Scalability In Medicine
An exploration of the perverse economic incentives in the practice of medicine and the obstacles faced in treating COVID vaccine injuries.

I have always been fascinated by the subject of free will, and continually saddened by observing individuals choosing to relinquish the spontaneity they inherited as living conscious beings. In turn, I’ve tried to touch upon how predictable psychological patterning, external influences, and predefined thought patterns help to explain many of the abhorrent behaviors we’ve observed from the medical profession, the scientific authorities, and the general public over the last three years.
Examples include:
•Highlighting how the invisible public relations industry receives approximately 100 billion dollars each year to brainwash the public into obeying its sponsors.
•How doctors’ perceptions of reality are shaped so that they cannot perceive “inconvenient” illnesses.
•How the harsh medical training each doctor goes through leaves them with an existential need to believe their practice of medicine is safe and effective (retained emotional patterning, such as that resulting from traumatic experiences, exerts an enormous influence over most people’s lives).
•How the current academic system trains people to forfeit their critical thinking and instead follow rigidly defined cognitive algorithms, which prevents most of those it trains from arriving at inconvenient conclusions while simultaneously zealously believing in each defense they provide for the orthodoxy.
One of the fundamental obstacles to embodying free will is which beliefs one chooses to navigate reality. Each axiom (foundational assumptions about reality) you follow inevitably restricts your perceptions and actions into falling into accordance with that axiom. Conversely, if you instead discard every belief you use to navigate reality with, life becomes almost impossible to navigate through, which hence, completely invalidates the merits of any philosophy which advocates discarding those axioms in your daily life.
I presently address this dilemma by doing my best to pick accurate beliefs while simultaneously being willing to temporarily put them aside on a case-by-case basis (which is often necessary for addressing complex medical conditions) and embracing the dynamic uncertainty you are forced to enter once you let go of your anchors to reality.
Unfortunately, the human mind tends to dislike experiencing the powerlessness that comes with acknowledging uncertainty. As a result, when many encounter a situation where their axioms fail them, rather than be humbled, they will respond by aggressively attempting to force the situation to conform to their beliefs.
I recently completed a series on the relationship between the gradual decline of critical thinking within our society, and contemporary medical controversies. A central point of that series is that the education process conditions each student to become boxed into a linear mode of thinking revolving around the axioms of the orthodoxy, and the more educated one is, the more aggressively one holds onto those axioms.
Many of the frustrating behaviors we’ve observed over the last two years have resulted from this conditioning. For example, this is why educated individuals often have the most difficulty understanding arguments which challenge the narrative; they are trained to only focus on identifying ways to dismiss an argument that questions any of their axioms rather than holding the mental space for hearing a divergent perspective.
Normally when this issue is observed, the close-mindedness and stubbornness of the orthodox party are viewed as a consequence of “ego,” and their behavior attributed to either a conscious attempt by egotistical individuals to protect their pride by not admitting fault, or a fearful ego’s attempt to protect itself from the shame of being wrong. I would, however, argue that there is a much more fundamental issue at work—the human mind has a great deal of difficulty functioning without axioms (along with some type of purpose to its existence) and will fight vigorously to protect the set of beliefs it has.
Is Money The Root Of All Evil?
The origins of our faith and devotion to money have raised many questions throughout the ages. The love of money has been recognized as one of the most powerful forces for twisting human hearts towards evil (which often results in immense destruction to the people or the environment), while simultaneously, its value is often completely arbitrary—money gets printed and then assumes value because everyone holds a collective faith in it. At the same time, money is a remarkable force for both developing and organizing society, and many of the things we depend upon are only available to us because of the economic system we live within (although conversely money is the primary tool which the upper class uses to enslave the rest of the population).
When the question of money is looked at, it is often seen through a lens of greed being a deadly sin. However, I would argue that effectively accumulating money is a foundational axiom which most people use to navigate life. On one hand, this helps to explain why the motivations of others often become so much clearer once you cut through all their rhetoric and view things strictly through what they stand to profit from.
On a deeper level, the need to optimize financial acquisition helps explain many of the behaviors humans will follow, because their internal algorithm will frequently default to the choice that acquires more money. For example, both Walmart and Amazon committed to a strategy of undercutting local businesses on prices as a strategy to grow their market share. This has been devastating to local economies, and forced many in Middle America into the corporate workforce (where they are paid less and treated worse) since no other jobs remain (which further accelerated after the COVID-19 lockdowns closed small businesses but not these behemoths). Despite the fact that many are aware of this issue, they cannot stop themselves from supporting these corporations because they “need” the (slightly) lower prices being offered.
Algorithms of Business
In the same way that a default behavior to seek the most profitable choice helps to explain many of the individual actions we observe around us, businesses also follow a relatively predictable set of behaviors aimed at optimizing profit, which you can see in a wide range of industries.
In general, most large businesses aim for the following:
•To achieve continual growth.
•To have a product they sell with a large markup (hence allowing them to profit significantly from each sale).
•To have as wide a market as possible for their product.
•To ensure that they have market exclusivity (so they can maximize the sales within their market).
•To ensure that they have repeating sales of their product far into the future.
The pharmaceutical industry—not surprisingly—excels in these areas, which helps to explain why they have managed to sustain steady growth for decades, and why one-fifth of all money spent in the United States goes to healthcare.
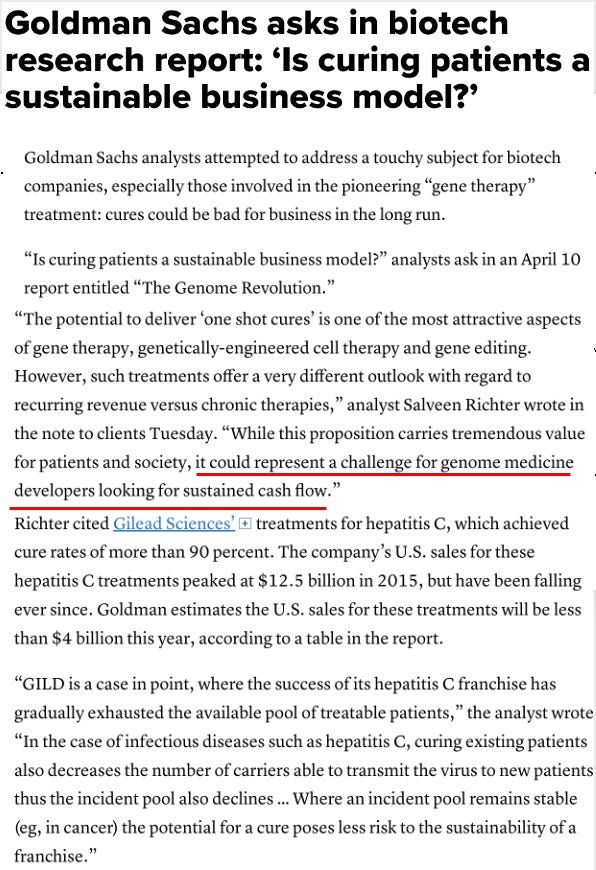
At the time this report was published, it understandably provoked significant outrage as these economic principles were not that well understood by those outside of the industry. Most pharmaceutical products do not cure illnesses, rather they perpetually shoot for a vague target (e.g., lowering cholesterol to prevent heart disease) or temporarily alleviate the symptoms of a chronic condition (e.g., reducing stomach acid production to relieve chronic heartburn).
If I had to vote for the worst offender in this regard, I would probably choose psychiatric medications. They are often prescribed for largely subjective diagnoses which far too many people can be folded into, they often don’t “help,” but due to their addictive nature (antidepressant withdrawals can be catastrophic), they often require lifelong use, and they frequently create many other life-impacting side effects such as brain damage that necessitates additional psychiatric medications (e.g., Bipolar I, which is treated with antipsychotics, is a very common side effect of antidepressants).
Vaccines and Scalability
When I was younger, I had a side gig reselling premium quality avocados (the ones you get in the store are not the best tasting, but are stocked by supermarkets because their thicker skins hide cosmetic damage). I was excited by the prospects of this endeavor, but when I shared its technicalities with a friend who worked at one of the top business programs in the country, he immediately shot my idea down because it “couldn’t scale.” He was, of course, right, but I still kept at it for a few years, because while it did not make too much money, it did give me access to those avocados.
Within business, the focus on almost any project or endeavor is “can it scale?” and the businesses that rise to the top are those best able to scale. Scalability in turn, is largely a question of meeting the criteria described in the previous section (e.g., can its market continually grow), and once you have an eye for this, you start being able to see how this algorithm always dictates a business’s behavior.
Vaccines, in turn, are an ideal product due to their scalability, and thus are a key priority of the pharmaceutical industry. Recently, the FDA provided a statement that inadvertently synopsizes much of the current situation:
Consider now how each of the following is likely to ensure the scalability of a new vaccine:
•Due to the widespread faith in the magic of vaccines, people are likely to assume that the product works and will take it even if there is no proof that it works.
•When vaccines fail, those failures are attributed to not enough people being vaccinated to achieve herd immunity (this is often a threshold that can never be reached), the immunity of a vaccine waning (and requiring a booster), or a new variant emerging which needs a new vaccine. All of these outcomes are, not surprisingly, excellent for increasing the scalability of the vaccine product.
•Due to the legal liability protections which all vaccines get (for all practical purposes you cannot get any type of financial support if you are seriously injured by a vaccine), the need to ensure safety is waived. This makes the vaccines much cheaper to develop and allows many which would normally not be profitable due to their legal hazard to remain on the market.
•A robust apparatus exists at the CDC to immediately get any vaccine with FDA approval (regardless of how questionable the approval process is) into the clinical guidelines used by physicians and health departments around the country. As you might suspect, there is a great deal of corruption in this process, and state or federal governments often subsidize it by directly purchasing large orders of each new vaccine.
•An excellent distribution system exists to get the vaccines to each possible recipient. Besides the physical delivery of vaccines to their end points, there is also the management of the potential recipients into being receptive to taking the vaccines. This includes doctors being programmed to berate their patients for not filling up with every vaccine, every health care facility offering them to their employees and patients, community vaccine clinics promoted by health authorities, and public health “activists” cooking up as many vaccine initiatives as they can (some of the more absurd incentives are listed here).
•Mandates for the population were justified under the rationalization that the alleged benefit of vaccination outweighed violating the rights of those who do not want to be vaccinated. Significant focus has been devoted to this area over the last ten years, which I suspect was a result of those in charge knowing that the potential toxicity of many of the new vaccinations would be a barrier to the scalability of these products.
•Vaccines create long-term side effects which require the consumption of other pharmaceuticals for those side effects. This is best seen with the childhood vaccines (as they commonly cause autoimmune and neurological conditions), but it has also been observed that companies such as Pfizer are investing in medications that target known side effects of the spike protein. Similarly, the large “unexplained” spike of RSV (which was predicted in the COVID mRNA vaccine trials) has prompted both Pfizer and Moderna to pursue RSV vaccines for this new “emergency.”
Although vaccines represent a nearly irresistible market, a major challenge in scaling it has always been their production time (e.g., the reason why the flu shot never matches the circulating variant is that the vaccine has to be produced well before the flu season, and it is very difficult to accurately predict which variant of influenza will be the dominant strain at the time of production).
A major reason why the mRNA technology was pursued was that the production time for each new vaccine was dramatically shortened. This made it possible both for the military to meet its need to rapidly produce vaccines for emerging bioterrorism threats and to support the pharmaceutical industry’s growth by developing vaccinations for many previously ignored diseases.
Market Protection
Capitalism, in theory, is the best economic system that has been developed, since it encourages the entire population to work, continually develop new products that are superior to previous models, and makes most goods and services be priced at a level the general populace can afford. Unfortunately, capitalism tends to fail once the players grow too large because it is often more profitable to rig the market so that an inferior and overpriced product receives a monopoly rather than to produce a superior product that succeeds on its own merits.
This also synopsizes the situation which the pharmaceutical industry frequently finds itself in; due to the massive profits which their business model creates, the industry (previously referred to as the “medical trust”) can often afford to protect the market share of an unsafe and ineffective product (e.g., the COVID vaccines). One common strategy is to buy out the media (which is why only studies that support the narrative end up being published, why only industry-friendly messages are aired on the news and why any reports of vaccine injuries that occur are censored by most social media platforms).
Another common strategy is targeting medical practitioners who threaten the scalability of a pharmaceutical product. Approaches include:
•Revoking the medical licenses of physicians who utilize an effective therapy that competes with an industry product. This revocation is done in a public fashion as a warning to other physicians, who will then be reluctant to expose themselves to the same risk. Meryl Nass’s prosecution by her medical board for treating COVID with hydroxychloroquine and ivermectin is one of the most well-known contemporary examples.
•Having law enforcement agencies raid or prosecute clinics promoting competing therapies, which like the previous example. has been an issue for decades. One of the more recent examples happened in the early days of COVID-19 when a provider of IV Vitamin C was prosecuted for providing IV Vitamin C to those with COVID-19 (although not the most effective therapy, this treatment is safe and often quite helpful for COVID-19).
•Using the academic press and media to destroy the reputation of a dissenting doctor.
Since scalability and thus, profitability, is the unifying thread behind many industry decisions, it is often quite easy to identify the real motivation behind many statements from the pharmaceutical industry. For example, consider this 2-4-21 statement by Merck (the original manufacturer of Ivermectin) that was trumpeted throughout the media:
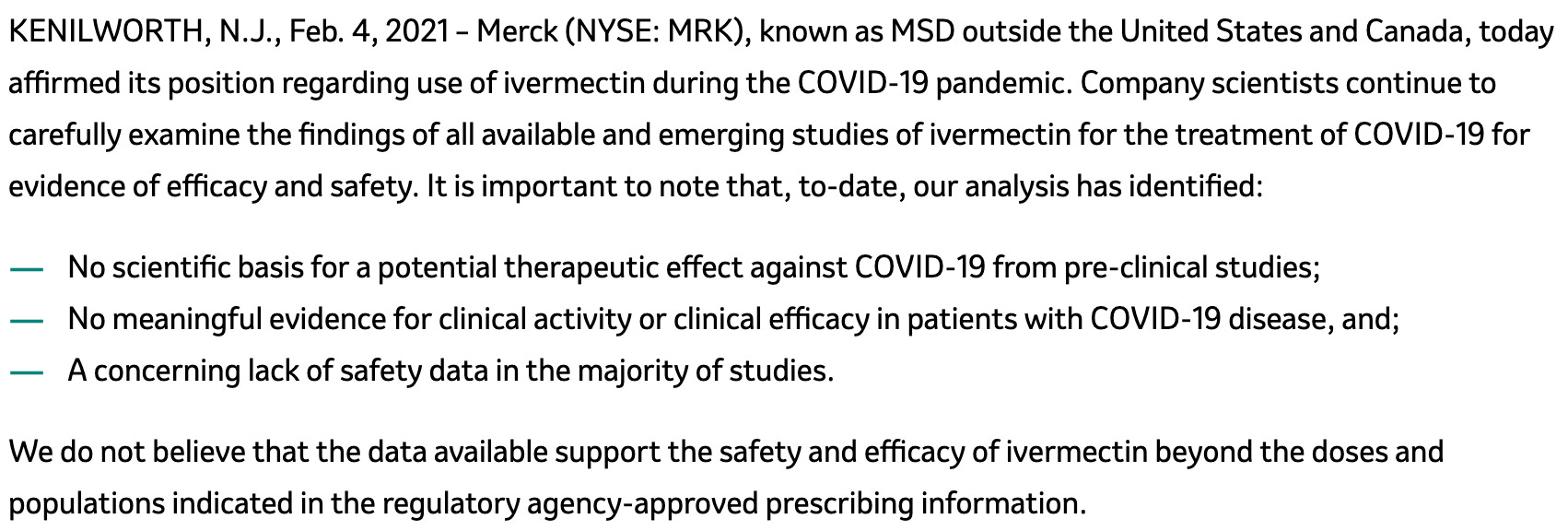
In addition to a large degree of existing evidence that ivermectin was helpful for COVID-19, this statement is particularly ironic, because Merck developed the robust safety data that was originally used to license ivermectin, and Merck has received massive fines for promoting dangerous uses of their drugs which differ from the regulatory agency approved prescribing information.
However, if you also consider that ivermectin is off-patent (and therefore cannot make money for Merck), and that Merck was heavily invested in developing a treatment for COVID-19 (with an inferior safety and efficacy profile compared to ivermectin), this behavior makes much more sense.
Another article I am drafting is about Peter Rost. Rost was a Pfizer executive and early whistleblower (Brook Jackson is a more contemporary one), who shared many extremely concerning behaviors which he observed within Pfizer’s corporate culture while fighting a protracted legal battle with them. At the time of Rost’s struggle, a debate in Congress was occurring regarding the reimportation of off-patent drugs.
The populist position was that since American drugs which were sold in other countries were much cheaper, buying them there (e.g., in Canada) and then reimporting them would make it possible for the poorer members of society to afford them (many living on fixed incomes struggle to afford their pharmaceuticals). The industry position was that the safety of reimported drugs could not be assured and thus needed to be outlawed.
Rost came to prominence by testifying at congressional hearings against the pharmaceutical industry’s arguments to prohibit reimportation. There Rost clearly made the case that the only reason reimportation is prohibited is because price gouging American consumers is necessary for the pharmaceutical industry to sustain its incredible profits. As you might expect, almost twenty years later, the FDA is still working on a way to “safely” reimport pharmaceuticals.
Scalability in Medicine
The more I look at medicine, the more I see much of it as a production line to efficiently extract billable services from each patient that is seen by a healthcare provider. For example, much of primary care is just patients being placed on lifelong prescriptions (many of which I and others believe hold a questionable benefit), or being referred out for lucrative medical services (in both cases the primary care doctor can face grave legal liability if they fail to recommend these products to their patients). Similarly, although some hospital services are necessary, many others are not and in each case, they are typically priced out at a far greater amount than their cost (this is a great investigation of the subject).
Once I started looking at medicine through the scalability lens, I realized that much of the training we received as doctors is designed to make us follow a model of medicine which relies on the distribution of medical services and products. This lies in contrast to most other medical systems which emphasize utilizing what the doctor has at hand to improve the health and well-being of each patient they see (a model that prevents parties other than the doctor from profiting off the encounter).
I believe this is partly because the previous economic systems could not support the current model (people were poor enough they would not pay the doctor unless tangible results could be provided, and in previous times a massive medical-industrial-complex did not exist which could afford to monopolize the market to assure its continued influx of revenue). I also believe this was because corrupt pressures and incentives were not placed upon doctors to prevent them from doing what they believed was in their patient’s best interest.
In a recent article, I discussed the concept of (corporate) economic feudalism, which I believe is the governance system which the oligarchs are trying to impose upon the populace. This system seeks to establish corporations as modern-day “lords,” and the working class as “serfs” (economic slaves) of those institutions. This system requires a gradual impoverishment of the population so that they are willing to settle for a grueling and degrading corporate position (e.g., millions in corporate America were forced to choose between an unjustified vaccine mandate or termination of their job and reluctantly underwent vaccination because they could not afford to lose their jobs).
The utility of this feudal model is that small economic incentives can quickly be implemented on a top-down basis, which allows the rulership to effectively control the behavior of the population. This matters because it is a much cheaper and more effective approach than would be obtained from using a standing army for enforcement (which was what monarchs and lords in the previous era needed to do).
Economic feudalism has touched many industries including medicine, and many of my colleagues have remarked that their profession has made a grave error by surrendering their power to the corporate workforce. This, in turn, has led to situations such as that experienced by Paul Marik, a world-renowned ICU doctor who was targeted by his hospital for using a protocol, that to the gratitude of his patients, effectively treated COVID-19, but made far less money than the ineffective protocol which Fauci mandated upon America. After Marik refused to switch to the desired protocol, his hospital destroyed his professional reputation and locked him out of future employment.
By using a combination of overt economic sanctions to create a climate of fear for non-compliant physicians (e.g., what Nass and Marik experienced), and softer economic incentives (doctors forfeit a lot of money which their clinics need if the doctor fails to follow policy guidelines such as vaccinating most of their younger patients), the scalability of each product in the medical industry is ensured.
In previous eras, I know of many cases where a non-compliant physician who pioneered a now-forgotten medical innovation refused to sell their therapy to the medical-industrial complex, and then were legally prosecuted (or worse). Thus far, I have not seen anyone sent to jail for challenging the medical trust during COVID-19 (although the IV Vitamin C doctor may be), which in my eyes, represents tremendous progress in this area.
At this point, I operate under the assumption that pharmaceutical companies have employees assigned to monitor the marketplace and identify competing scalable therapies that could threaten their monopoly over the treatment of a disease. This helps to explain why the same playbook is always used against any competing therapy medical doctors could easily distribute to their patients.
Simultaneously, it also helps to explain why many extremely effective modalities I’ve used throughout my life are almost entirely left alone (barring the occasional ridicule they receive from scientific orthodoxy). Although those approaches can eliminate potential customers from the marketplace, these approaches cannot scale and thus are not worth the cost it will take to prohibit them from being used in general medical practice.
I endorse certain alternative modalities (e.g., acupuncture). However, I’ve found with most of these approaches, their results are highly dependent on the practitioner’s skill level (e.g., many acupuncturists do not provide enough of a benefit for me to justify a referral, while others are miracle workers who have greatly helped my patients).
Because they tend to get the best results, many of the therapeutic modalities that I utilize are non-standardized approaches that require sensitivity, subtle observational skills, critical thinking, and creativity to employ correctly for each patient. This customized approach is very different from the training doctors receive (where they repeatedly follow standardized steps shown to them so that they can perform the same medical procedures), and thus nearly impossible to scale.
Point-Of-Care Ultrasound
Recently I read a post by Pierre Kory that illustrates many of the same issues detailed above. Within the ICU, it is often critical to identify what the key issue is in a patient as soon as possible (since delays can lead to death). Most of the diagnostic tools available in the ICU suffer from a time delay (e.g., getting an MRI done and the results sent back to you takes hours, and the same is often is true for bloodwork).
However, one exception is point-of-care ultrasound (POCUS is where a doctor quickly ultrasounds all the common areas where a severe problem can emerge from). This is because within minutes, the doctor can identify if any of the key areas are abnormal, and thus initiate a protocol that could save the patient’s life (on a side note, Kory’s experience with POCUS also allowed him to occasionally observe blood sludging within the largest veins, which he, like researchers decades ago recognized as a sign which immediately preceded death).
One interesting facet of Kory’s journey to get POCUS into the ICU was that many resisted it (e.g., radiologists or cardiologists who traditionally billed for bedside ultrasound examinations claimed that no one besides them was qualified to perform them, hospitals were reluctant to implement it since the ICU doctor would just do it rather than spending a long time writing up an extensive report about it that could be billed for).
Kory’s team was eventually able to succeed in getting ultrasounds into the ICU under the justification that by improving the safety of common hospital procedures, they reduced hospital liability (which is a huge concern for hospitals). However, despite this occurring, I have never worked at an ICU where ultrasound was utilized (excluding the occasional focal examination of an area where an issue was suspected). Instead, most ICU doctors default to ordering lots of tests in the hope that one will at least give them the information they need (fortunately some ICUs now have doctors who were motivated to adopt POCUS into their medical practical).
It would be nice if more ICU doctors were willing to make the effort it would take to train to familiarize themselves with a complex diagnostic approach (getting an accurate ultrasound evaluation in a single area is well known for being dependent on the skill of the operator, so performing a global examination and integrating it with a clinical picture is quite challenging). However, while that has not yet happened within the ICU community, medical schools are beginning to recognize the utility of ultrasound and gradually adding it to their curriculums. It is thus quite possible that some of those students will be willing to pioneer ultrasound being utilized where it is the most needed (which speaks to the broader issue of the medical profession often taking decades to adopt critical innovations).
COVID-19 Vaccine Injuries
One of my main projects over the last two years has been to figure out how to treat COVID-19 vaccine injuries. This has been helped by the years I spent studying other pharmaceutical injuries, because many of the complications observed are similar to those seen with other toxic pharmaceuticals (and thus responsive to similar approaches), but at the same time, COVID-19 vaccine injuries tend to be more difficult to treat than other pharmaceutical complications.
In that journey, I’ve done my best to correspond with those who are getting results in treating these injuries (and previous pharmaceutical complications). When I share my preferred approaches with these physicians, however, the most common critique I receive is “that’s intriguing, but it's not scalable.” Given the immense need for help, many vaccine injured patients have, that is a completely valid objection, and it has thus been a puzzle I’ve been wracking my brain over for the last two years.
From a political standpoint, there are a few major problems with treating vaccine injuries:
•Publicly stating that you are treating a COVID-19 vaccine injury requires you to acknowledge that the vaccines could cause an injury, and therefore, are not actually “safe.” In many areas, such as California, physicians I have spoken to are not willing to touch this subject because of the threat of the medical board revoking their license (which can results in them losing the ability to practice medicine entirely since medical boards tend to copy suspensions made in other states).
•Most of the approaches for treating COVID-19 vaccine injuries do not work consistently (each one works for some patients, but not for many others), and often are quite costly. This creates a situation where it is nearly impossible for the treating physician to defend against the accusation that they are exploiting vulnerable patients with fraudulent therapies.
A few options exist for addressing this problem, but none are ideal. They include:
•Having the “treating” doctor advise the patient to seek out medical services with a variety of other providers who do not administer the therapy for the purpose of “treating” a vaccine injury.
•Not advertising and only finding patients through word of mouth.
•Practicing under a medical freedom friendly jurisdiction (I am hoping a Republican state such as Florida will officially establish a policy for this in regards to the vaccine injuries at some point).
As you can see, regardless of the option chosen, all of these are significant barriers to the scalability of this approach.
The Scalability of Treating COVID-19 Vaccine Injuries
At this point, I have identified a few common subtypes of COVID-19 vaccine injuries. This is important to recognize because both the vaccine injury and its physiologic response differs from person to person, and thus, the same approach cannot be utilized for everyone. Assuming you select the therapy which is appropriate for each patient’s presentation, the options I know of for treating the COVID-19 vaccine injuries fall into a few different categories. Each of these has different challenges to scalability:
•Semi-expensive treatments that work quite well for a variety of vaccine injuries, but for all practical purposes are not available in the United States.
One of my colleagues largely suspended their clinical practice so that they could work towards making one such option available, but that is still a work in progress and it is not currently widely available.
•Treatments that work quite well but are very expensive (especially since repeated administrations are required) and I do not believe could have their production scaled up enough to meet the demand in the United States (although I may be wrong in this regard).
Another one of my colleagues switched to working part-time so they could work with a company to help make one such treatment accessible to the public.
•Treatments that work quite well, vary in their affordability, and are at high risk of being banned by the FDA. I’ve been stuck on what to do here because in the last few years I’ve seen the FDA make it impossible to acquire many of the therapies we previously utilized to help a lot of patients (thus requiring very careful rationing of the remaining stockpile).
The fear my colleagues, in turn, hold is that if we were to openly discuss these therapies in the context of their utility for COVID-19 vaccine injuries, the FDA would immediately remove them from the marketplace. Since it is unlikely a public protest could stop that from happening (e.g., consider what has happened so far with ivermectin), I’ve been asked to not publicly discuss those topics, which I believe is the correct choice, but still one I am conflicted over.
To share one recent example, the original COVID-19 monoclonal antibodies (which were one of the few approved COVID-19 therapies that worked) had their Emergency Use Authorization be withdrawn (see here and here) because the SARS-CoV-2 spike protein it targeted no longer existed since the virus has mutated. Curiously, however, this logic was not extended to the COVID-19 vaccines (almost all of which produce the original SARS-CoV-2 spike protein). Because the original monoclonal antibodies matched the vaccine spike protein, many COVID-19 vaccine-injured patients reported benefitting immensely from them. Tragically, however, once the EUA was pulled, all of it was disposed of (one colleague fortunately was able to obtain their hospital stockpile right before it was thrown away, and presently has 8 doses left).
•Expensive pharmaceuticals which can somewhat help the vaccine injured. Intravenous Immunoglobulin (IVIG) is one of the best examples—the NIH even covertly studied giving it to vaccine-injured patients, and IVIG has been previously used for certain treating HPV vaccine injuries (Merck’s HPV vaccine is also known for frequently causing severe autoimmune disorders).
While this approach can help some COVID-19 vaccine injuries, it is expensive and requires long-term administration (which makes the pharmaceutical industry support its adoption). However, due to the cost, insurance companies are understandably resistant to providing it, and I do not believe there is any way it would be possible to provide this therapy to everyone who needs it (from both a cost and a production standpoint).
•Cheap treatments that vary widely in their efficacy (e.g., B-12 occasionally helps COVID-19 vaccine injuries). I have seen people benefit from this option (and trying lots of supplements is the most common strategy I’ve seen in vaccine-injury support groups), but in most cases, it results in people taking lots of supplements but only having a small improvement from doing so.
There are a few affordable therapies that seem to consistently help (and do not create adverse reactions in the recipients), but these represent a minority of the options people are trying.
•Standardized pharmaceutical protocols that are calibrated with semi-expensive labs (making it very similar to many other functional medicine approaches).
Although this would address the scalability issue, the only approach I know of being promoted in this manner has left me with a few major concerns, and has not helped any of the desperate patients I know who have pursued it.
•Having a standardized evidence-based protocol like the Front Line Critical Care Alliance’s ever-evolving I-RECOVER post vaccine treatment protocol.
The main problem with this approach is that what patients need varies significantly (only some people are helped by the suggested first line therapies), which results in many needing to go through a large number of potential therapies (which is challenging for many) and patients needing to settle for a partial rather than full recovery. Additionally, some of the most effective treatments I know of are not discussed within the scientific literature and thus do not appear in guidelines like the FLCCC’s attempt to compile evidence-based treatments for vaccine injuries.
•Semi-expensive, widely used integrative therapies which each partially helps certain patients (e.g., hyperbaric oxygen).
The main issue with this approach is that it often exceeds a vaccine-injured patient's budget, and requires a competent integrative physician to determine which approach is correct for them. So, like many of the above approaches, it is not scalable.
•Patient-centered approaches like the ones I frequently utilize. These are sometimes what is necessary to treat COVID-19 vaccine injuries, but there are also many other vaccine-injury cases I come across that require many of the more expensive modalities outlined in this section.
Myself and colleagues are still trying to figure out if there is a practical way to sufficiently scale up the training necessary to make these approaches available to patients in need. I think it can be done, but many before us have also tried and have not been successful.
There are also a few treatments I believe have the potential to be efficacious and scalable enough to address the needs of the vaccine injured, but at this point in time they remain untested. I believe that if the COVID vaccine injured community could come together to produce something like what the Lyme community did, it could become possible to identify which method provide the best results for each type of COVID-19 vaccine injury, but I suspect it will be a while before a project like this gets off the ground (and I do not expect any conventional research to emerge in the meantime).
When reviewing this section, it is also important to remember that the pharmaceutical industry is presently investing in developing products that each treat different side effects of the COVID-19 vaccines. It is thus quite likely that they will follow the typical pattern and lobby the FDA to act against any approach for broadly treating COVID-19 vaccine injuries that thereby threaten these emerging markets. Instead, the condition will be broken into various smaller markets which each have their own expensive proprietary medication (like IVIG).
Conclusion
Not unlike how I approached the avocado business, my preferred way to practice medicine has always been to ignore the issue of scalability entirely. I spend a while with each patient and try to figure out what needs to be done to solve their case, rather than do a few standardized approaches that might help and then send them off to someone else (who probably won’t help them either) once those standardized approaches fail. Since I operate at capacity with this model and enjoy conducting it, I haven’t wanted to focus on scaling other parts of my practice (e.g., hiring employees, marketing, etc).
At the same time, a question I always ask myself is if it's ethical for me to conduct myself in this manner when I know some of what I am doing could be scaled up and reach far more people. Because of this, I always am working on projects I feel have the potential to affect a lot of people by meeting a critical need (e.g., helping vaccine-injured patients, providing key forgotten aspects of medical education, etc.). Since the support of the readers here has made it possible for me to help a relatively large number of people, this is also why I’ve rerouted so much time into this blog (406,000 words written in the last 10 months along with all the multimedia and comments I’ve put together).
So, while I detest the need for scalability which our economic system revolves around, I also recognize that it is sometimes necessary. Fundamentally, I believe my core difference of opinion is best expressed by Rudolph Steiner. Steiner stated three conditions needed to be met for the consciousness of the human species to evolve. One of these was for man to no longer work for money (I strongly agree with many of the practical and spiritual arguments supporting this position, but it is a long discussion beyond the scope of this article).
In summary, I believe that once money is transformed from a means to facilitate your life purpose to an end in itself, it becomes a corrupting force that taints your soul. Many of the extremely wealthy suffer from this problem, and they develop an insatiable greed to own everything at the expense of everyone else while simultaneously lacking much of the basic happiness we of the lower classes take for granted (I know a few people I’ve observed this in and I’ve been told the same by many others).
Finally, in the week since I posted my previous article on the German insurance data, I’ve spent a lot of time revising it and trying to vet the legitimacy of the data. At this point, I have not been able to identify any credible arguments which refute it (all but one of the rebuttals that the German authorities provided are not-valid, and the last one depends on a data source I have thus far been unable to establish the validity of). Given the importance of this data, especially for demonstrating the wide range of injuries associated with vaccination, I would strongly encourage each of you to review this article, and if you are able, to conduct your own independent review of the data (a few have been conducted since the time of publication and are included in the revised article).
" For example, both Walmart and Amazon pioneered a strategy of undercutting local businesses on prices to grow their market share. "
I know this article isn't about economics, but one thing I rarely ever see people mention is that cheap debt (printed money from the Fed) is necessary to create these corporate behemoths. It is this cheap debt that allows these mega corporations and franchised businesses to expand so rapidly and grab their market share. Without this cheap debt, it would be extremely difficult to acquire and build out the capital (buildings, truck, equipment, etc.) needed to run these businesses.
Hospitals require lots of capital (buildings, equipment, etc.). Cheap debt has allowed a small handful of corporations to take over the healthcare market. Before that, my understanding was many hospitals were run by charitable organizations, churches, etc - smaller, more private actors.
At the same time, this cheap debt makes capital equipment relatively less expensive than people. So, businesses install capital equipment at a more rapid pace than they would without the cheap debt. However, the employees cannot adjust their skills fast enough under the regime of cheap debt. So, many of them lose their jobs, even though the addition of capital equipment actually creates more, but different, jobs.
I would argue that it's not so much money, but fake money or debt that is treated as money, that causes these problems. When there is a love of money and you can simply clip coins (the ancient way - there are Bible passages on equal weights and measures about this very thing), print money (the way of most of the 20th century) or add digits in a computer (today's way), you don't need to put in any work to actually acquire more money. That naturally attracts the wrong type of people to having the most money. And, that's the problem.
Despite all the censoring, another thing to consider is the 'ignorance is bliss' mentality. If we choose not to know about or understand something, then we have no moral culpability to respond. Often, that's why it's easier for us to believe a lie than to explore an uncomfortable truth.