All Evidence Suggests The COVID Vaccines are Causing a Spike in Disability and a Potential Catastrophe for Our Economy

A few days ago I posted an article suggesting the mRNA vaccines were causing a spike in disability. Since that time the story has gone viral, I’ve had more time to look at the data, others have as well, and I now feel the case is very strong. Because this message is critically important, I am writing a second follow up article on the topic. In this article I will attempt to present a comprehensive analysis, and put the data into context with my experience of having worked with individuals with COVID vaccine injuries and individuals with varying degrees of disability including those seeking disability.
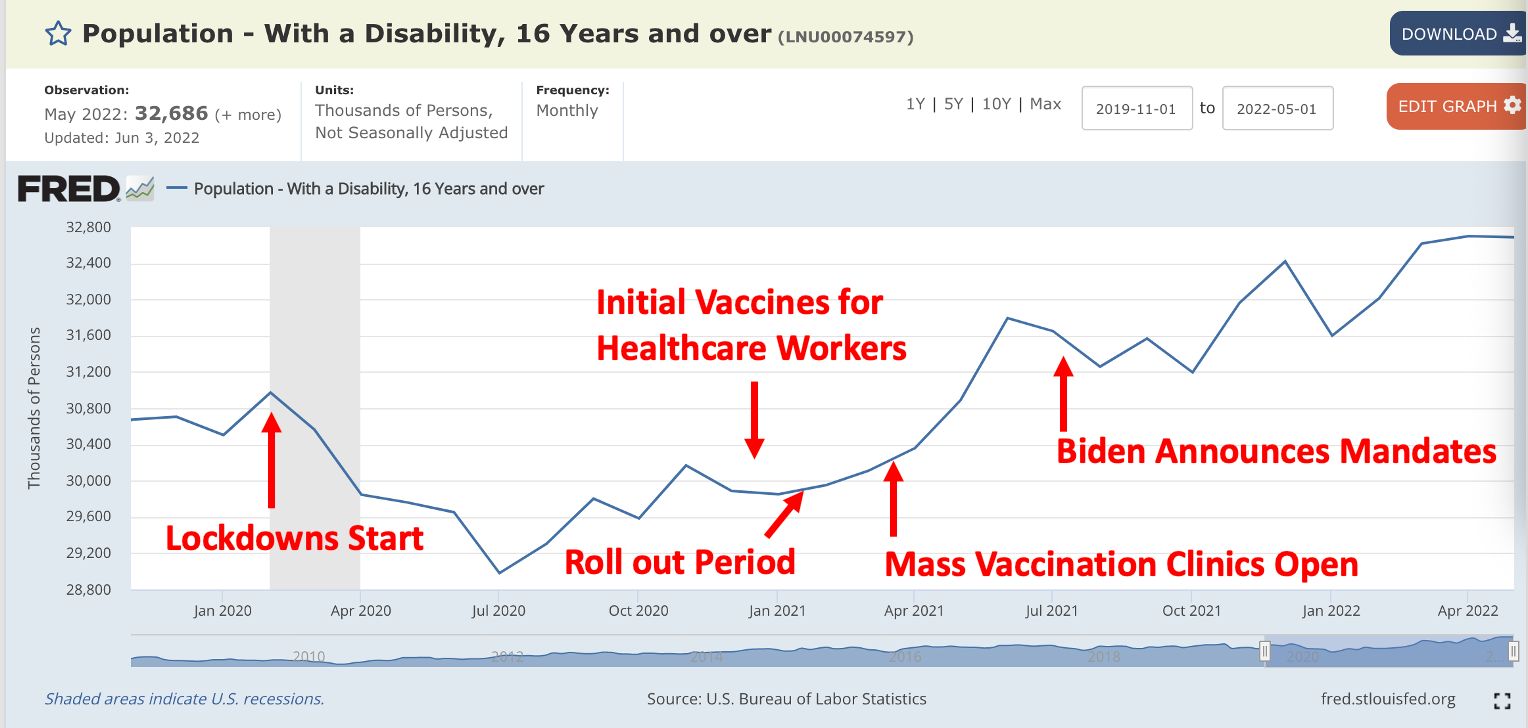
The initial discover of this dataset was Ed Dowd (the Blackrock executive who broke the story of the spike in life insurance claims following the vaccine rollout). He shared this dataset (which can be verified here):

Let’s quickly annotate that to put it into context:
Pharmaceutical injuries tend to follow a bell curve, where the more severe ones are rarer than the less severe ones. However at the same time, the most severe ones more easily catch the eye and hence tend to be disproportionately noticed. For example, in the adverse event log that I put together, I heard of many cases of deaths from the COVID vaccines that someone called me up to tell me about, whereas it was rare someone contacted me regarding a moderate injury that happened to someone they knew. Conversely many people I know personally developed moderate to severe chronic complications from the vaccine, but no one I know directly has died.
One of the major problems with evaluating adverse reactions from pharmaceutical drugs is that there is a tremendous degree of latitude for the manufacturers to classify the injuries as something that is not concerning. There have been a few noteworthy cases of this during the COVID vaccine trials, such as Maddie De Garay developing a permanent neurological disability which was labeled as "Functional Abdominal Pain." Due to how small that trial was, had Maddie’s injury been classified correctly, it alone likely would have resulted in the Pfizer vaccine never been approved for children. Sadly, there is always some way you can twist and re-classify data within a trial to imply that a benefit is there regardless of whether a benefit actually exists.
For this reason, most of the best authors who understand how to critically evaluate medical literature are of the consensus that the only data point that matters is how many people died in the vaccine group versus the placebo group (termed absolute mortality), as death is the one condition that is both meaningful and not possible to re-classify something else.
Because of how dangerous the Covid vaccines are, they have created a large spike in absolute mortality. There are countless datasets that show this including Pfizer’s final publication on their own vaccine trial. Many individuals have been compiling this evidence, and as far as I know, Steve Kirsch has the most comprehensive summary.
I had initially thought that it would only be possible to prove an increase in absolute mortality through the large available data sets, as the subjectivity inherent to classifying more chronic injuries prohibits them from ever being explicitly quantified through a large dataset. Thanks to Ed’s discovery, I learned of 1998 Executive Order 13078, which required the development of questions aimed to assess disability status throughout the population that were then to be added to the Census Department’s monthly Current Population Survey.
Three data sources exist for this purpose. Most of them unfortunately are not yet current enough to provide the needed data. The one that is able to (a monthly survey of 60,000 households) has existed since 2008. The six disability related questions in the survey were a product of extensive research to determine the best way to assess disabilities with a population.
The CPS uses a set of six questions to identify persons with disabilities. A response of “yes” to any one of the questions indicates that the person in question has a disability. The disability questions appear in the CPS in the following format:
This month we want to learn about people who have physical, mental, or emotional conditions that cause serious difficulty with their daily activities. Please answer for household members who are 15 years old or over.
•Is anyone deaf or does anyone have serious difficulty hearing?
•Is anyone blind or does anyone have serious difficulty seeing even when wearing glasses?
•Because of a physical, mental, or emotional condition, does anyone have serious difficulty concentrating, remembering, or making decisions?
•Does anyone have serious difficulty walking or climbing stairs?
•Does anyone have difficulty dressing or bathing?
•Because of a physical, mental, or emotional condition, does anyone have difficulty doing errands alone such as visiting a doctor’s office or shopping?
Labor force measures from the CPS are tabulated for persons age 16 and older.
All six questions in this survey directly overlap with debilitating conditions that overlap with commonly reported effects of Covid vaccine injuries (although the vision and hearing issues are less common). I also must note that many disabling conditions caused by these vaccines are NOT covered by these survey questions, so the magnitude of harm is still being underestimated.
This survey is remarkable because it provides an objective metric to assess population level changes in chronic injuries that cannot be reclassified in order to hide their occurrence. This results of this survey are also consistent with the pattern of chronic vaccine injuries reported to VAERS.
Overall, I can only see 4 possible explanations for this data.
•The COVID vaccines are causing severe chronic injury resulting in partial disability within in the population.
•The economic downturn from the lockdowns was responsible for this data.
•The increase of long haul Covid is responsible for this data.
•Sampling errors created by the lockdowns created artifacts within this data.
From reviewing the data, I believe only the first explanation is plausible. First to make this argument, I will highlight two analyses performed yesterday.
The first by Ben makes the trend explicit:
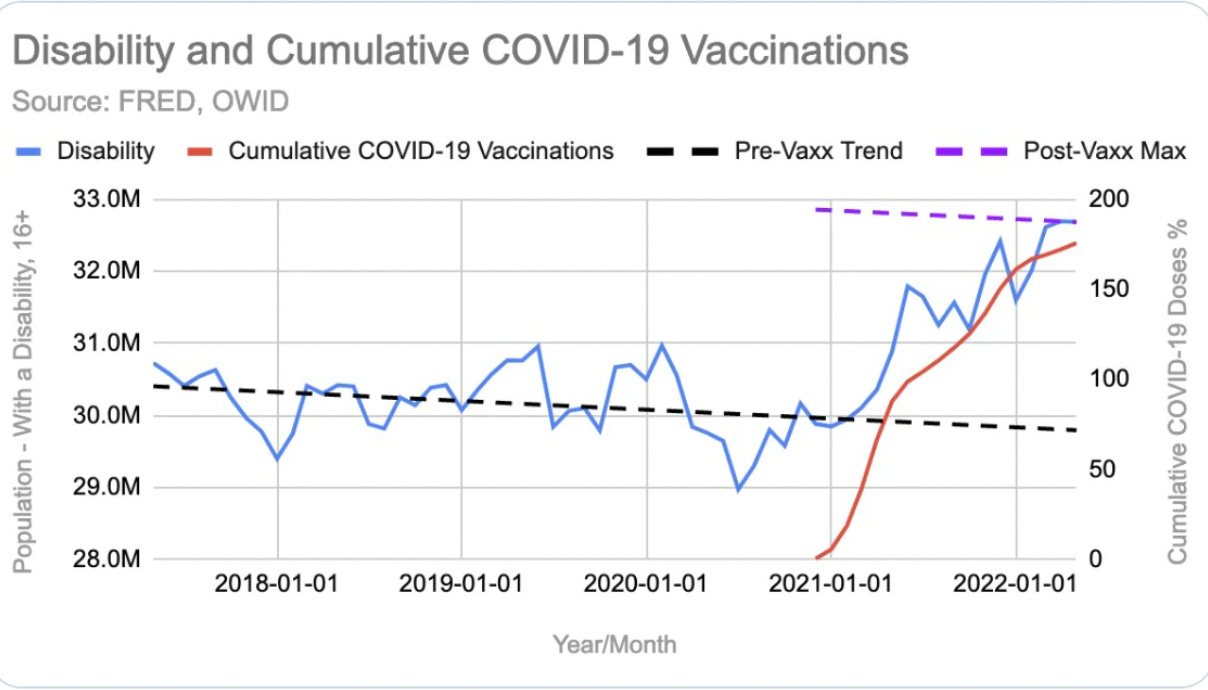
The second analysis by El Gato Malo clearly demonstrates the following:
•There is a clear correlation between the percentage of the population vaccinated and those with disability.
•There is a clear correlation between the percentage of the population boosted and those developing disability.
•This increase in disability in all cases starts between 1-2 months after the vaccines begin.
An argument commonly used to dismiss pharmaceutical injuries is that “correlation does not equal causation.” However, when the same correlation appears from multiple directions, this argument is much less sustainable.
The 1-2 month lag is particularly interesting because many of the chronic disabling symptoms from the Covid vaccination gradually worsen over time and it often takes a month for individuals to accept their condition is permanent and unlikely to resolve. Many of the people I know who became disabled from vaccination likewise took a month or so to develop the permanent disability. Additionally, since this survey is done once a month, there will often be delay of a few weeks from when someone develops a chronic injury to when they are being surveyed.
In the previous article, I attempted to compare the rates of disability increases observed to those amongst my peers. Using a 200 person sample I estimated there was between a 1-2% rate of developing chronic disability that would likely qualify for disability payments after vaccination, and 3-4% for permanent disability that would not qualify for disability payments. This matched the absolute increase in disability found by this survey (the 10% increase seen in the first graph is a relative increase in disability amongst those with disability, but since most of the US population does not have disability, the absolute increase also falls into the 1-2% range). While my sample is a smaller anecdote, this is once again internally consistent with the vaccination causality.
The one unanswered question I had from these additional analyses of the datasets was the extent of the J&J vaccine's contribution to this trend. One of the people within my own peer group who became permanently disabled had it occur from the J&J vaccine (so for me this was a large signal) but given the much smaller uptake of the J&J vaccine, my best guess is that the available datasets will make it impossible to assess the contribution of J&J to this issue.
A more precise breakdown of the data from CPS can be found here.
Note: As corruption of other large databases tracking vaccine injuries has occurred, it is very likely that future data will show a decrease in disability claims and it is likely these datasets may later be changed. I have archived everything there and advise you to do the same.
A few important results emerge from the CPS datasets which provide evidence against the alternative explanations for this trend:
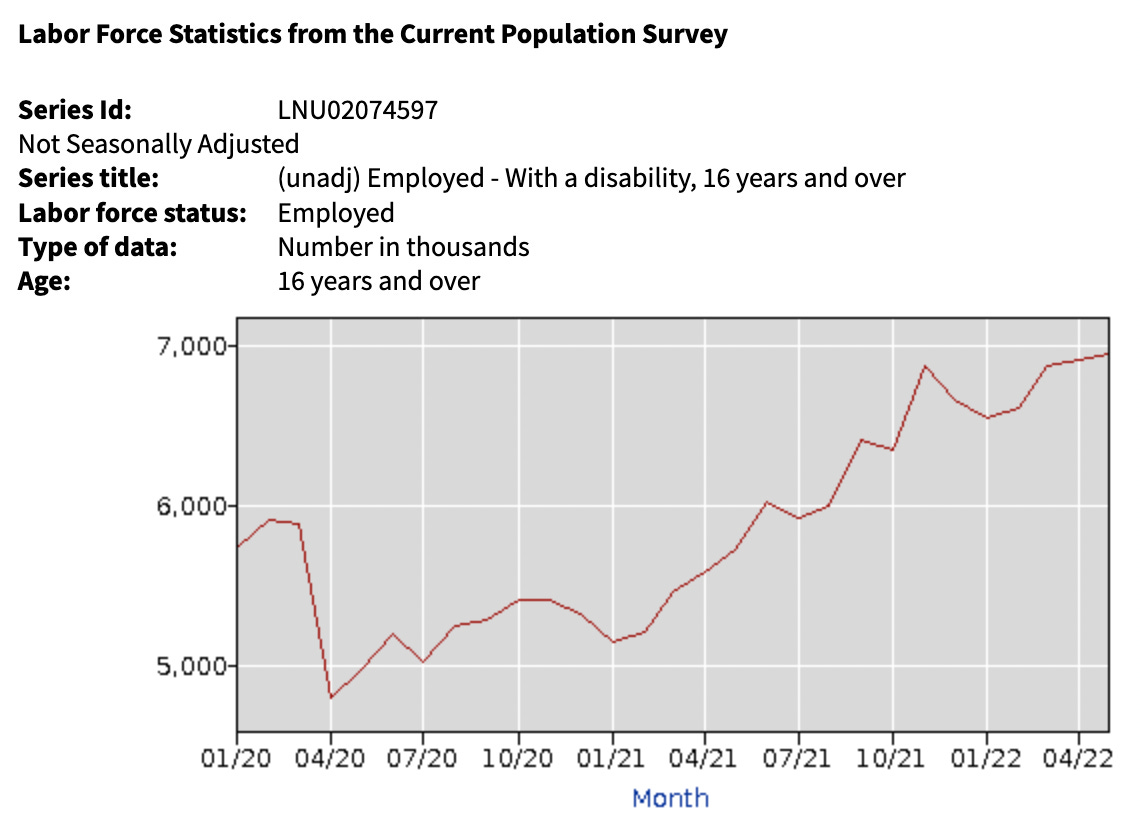
The above dataset shows that the lockdowns resulted in employed individuals with disability temporarily decreasing (most likely because they became unemployed due to the lockdowns), and then increasing by 18% (5,888,000 to 6,961,000) following initiation of vaccination campaigns. As vaccines are more likely to partially than fully disable recipients and members of the labor force were the most likely to be required to vaccinate, it makes sense that the largest increase in disability would be seen in this subset of the data-pool.
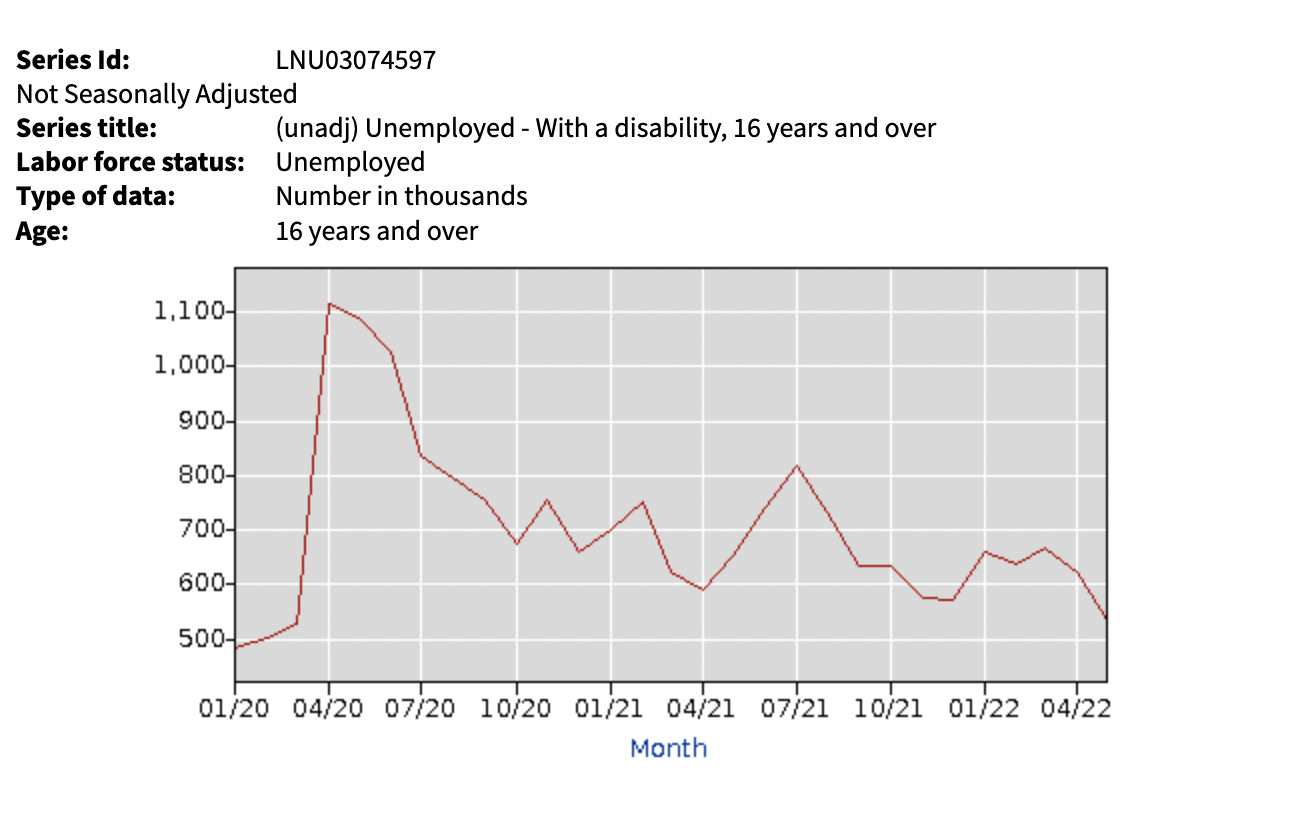
“Unemployed” is defined as not having a job but seeking work. A reciprocal relationship is seen between this and the previous dataset (keep in mind this represents approximately 10% as many people as the above one). An initial spike was seen in those unemployed with disability (since those who were employed and had disability lost their jobs due to the lockdowns), who then left this dataset once employment opportunities arose. Removing those who temporarily lost work, there was an increase from baseline in the number of unemployed individuals with disability, but it is much harder to discern the effect here. This is likely partly due to the fact unemployed individuals were not subjected to vaccination mandates.
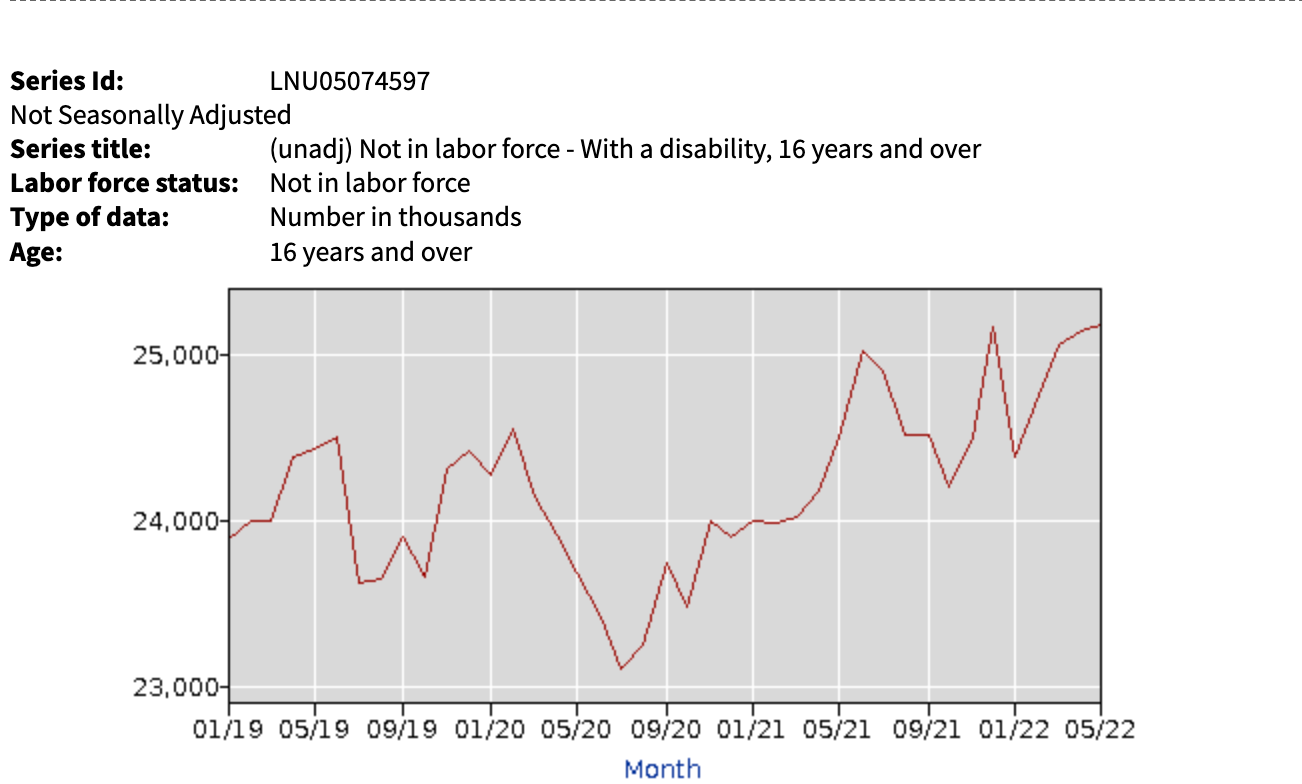
For those neither employed nor seeking work (classified as not in the labor force) and with disability, a clear trend appears. There was a brief drop in their numbers during the lockdowns (my best guess is that they either passed away during this period as this population is more susceptible to illness and stress, or started looking for work because they realized the lockdown no longer made it viable for them to remain unemployed). These changes leveled out, and factoring in seasonal variations of those “not in the labor force,” returned to baseline. Once the vaccination started, there was a 4.9% increase in the numbers of individuals not in the labor force (24005 to 25189) with disability.
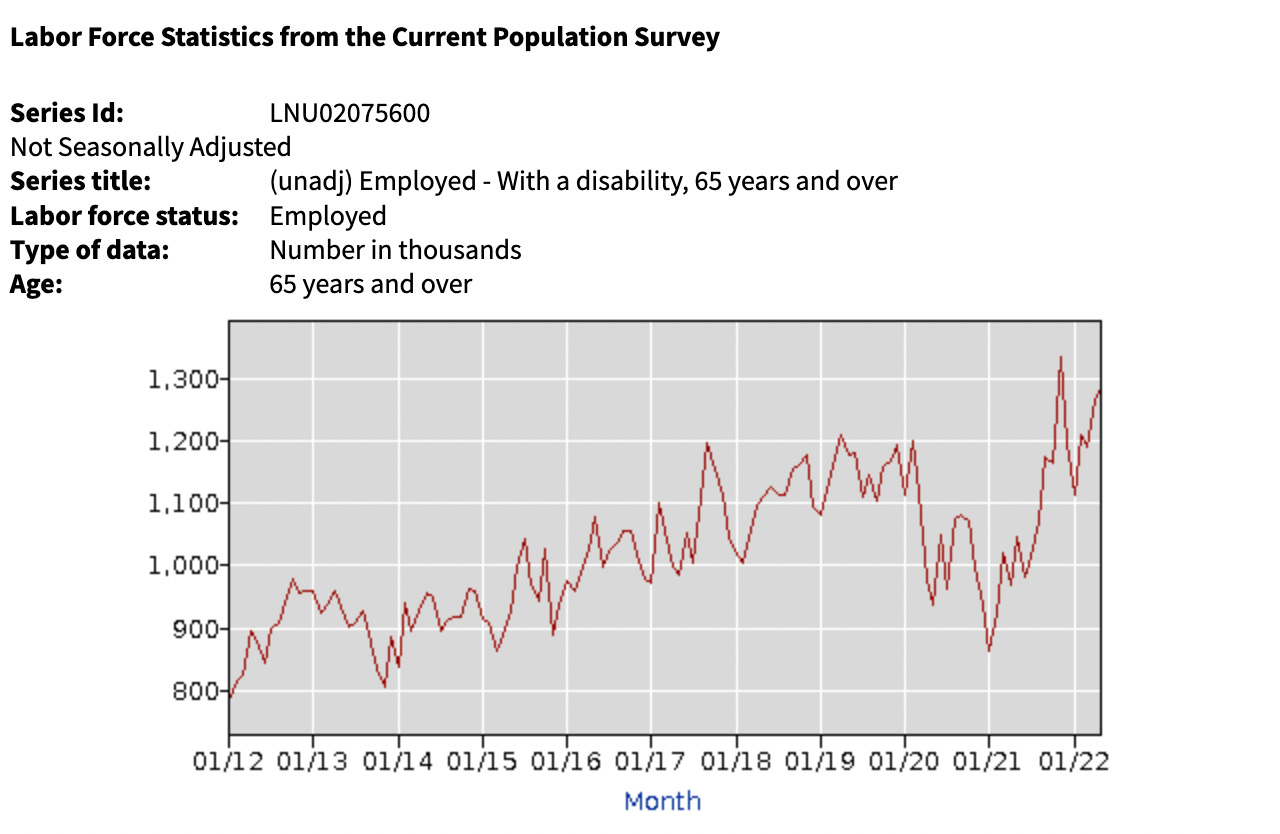
If we look at individuals over 65 who were employed, we see that there was an overall 15.5% increase (1,113,000 to 1,285,000) in disability. Additionally, this graph shows the sharpest trend in increases following the initial vaccine roll out, which makes sense since the elderly got the vaccines first and had a high vaccine uptake. In the space of 10 months we saw a 54.4% increase (865,000 to 1,336,000) in the rate of disability.
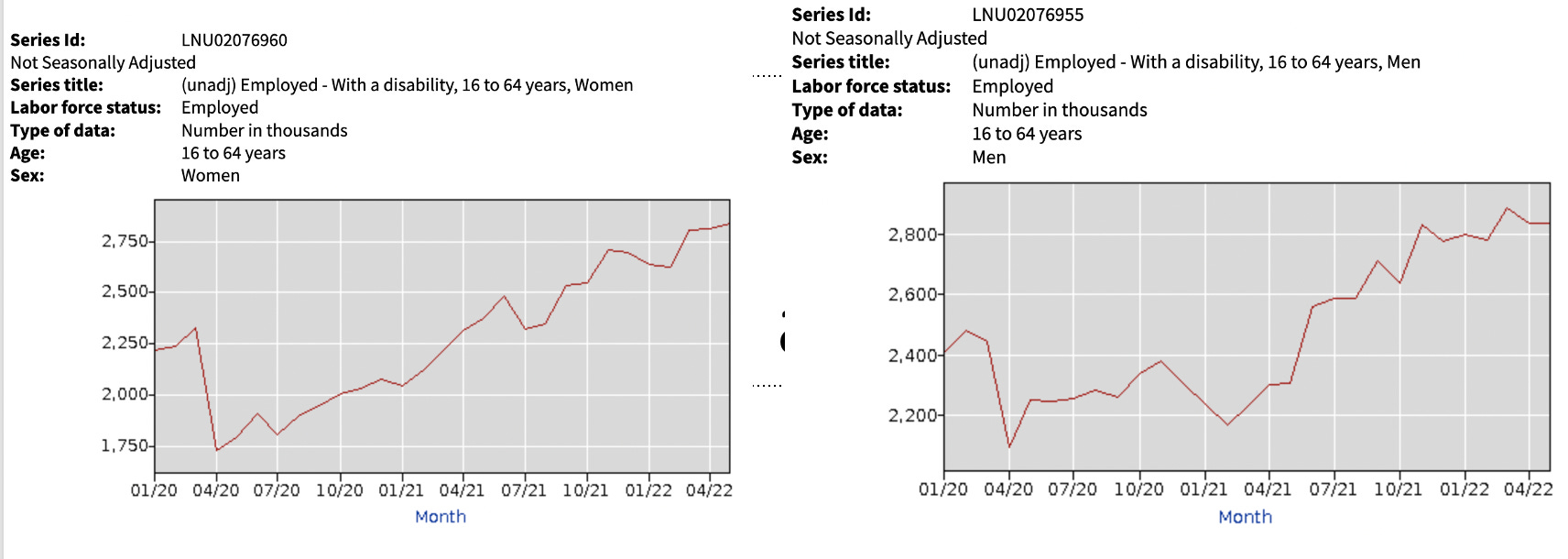
When we compare women to men, we see that women were faster to regain employment after the lockdowns (my best guess is they had a slightly easier transition to remote work). Once the vaccines entered the market, from Feb 2021 to now, there was a 34.1% (2,119,000 to 2,842,000) increase in disability amongst employed women and a 27.1% (2,236,000 to 2,842,000) increase from baseline of employed women with disability. For men, there was a 30.8% increase (2,166,000 to 2,834,000) after initiation of the vaccination campaign and a 14.1% increase from baseline (2,483,000 to 2,834,000).
For comparison, let’s compare the above trends in employment to the changes in employment status for non-disabled individuals.
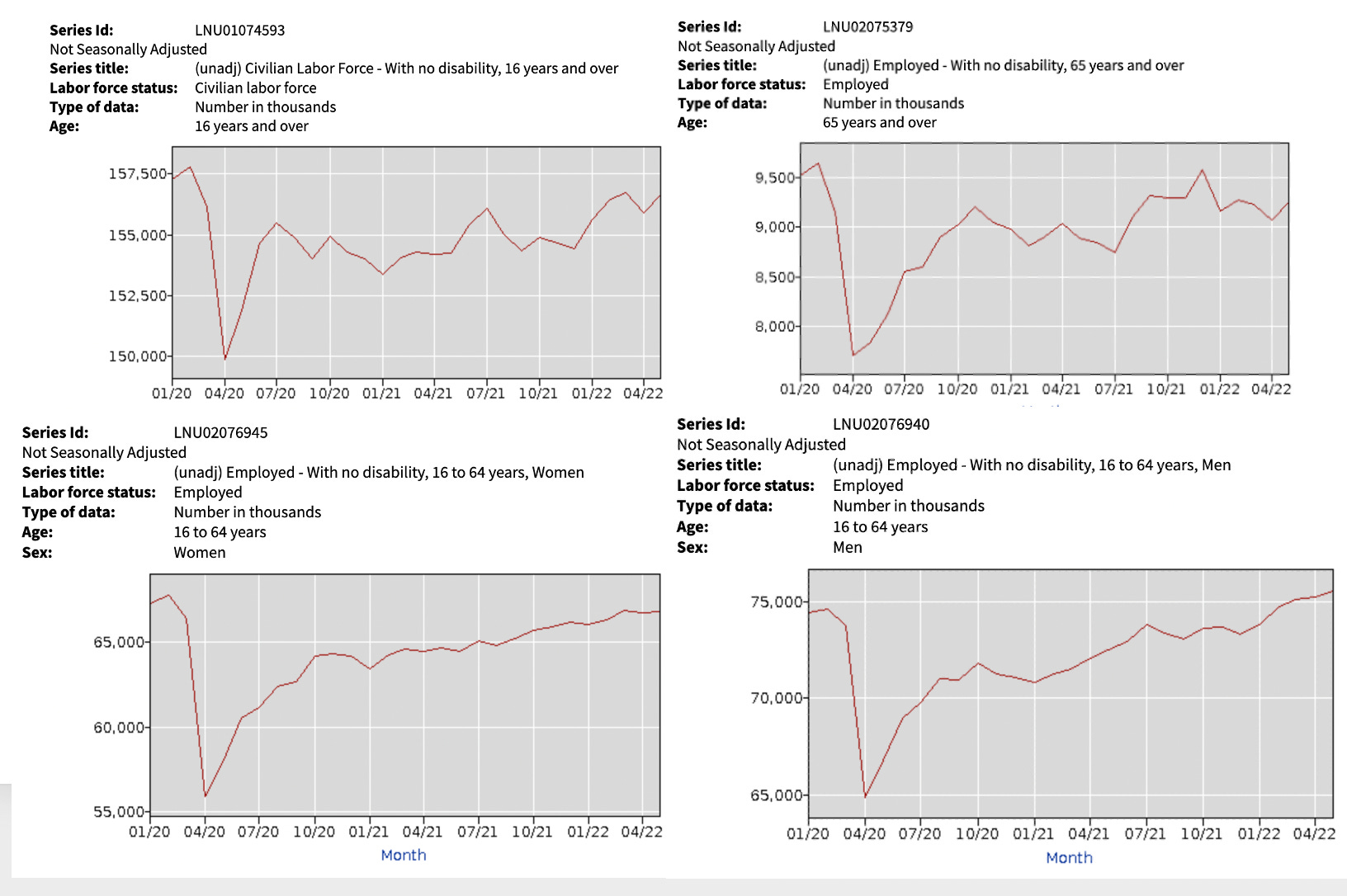
From this, we can see that while there was a reduction in employment due to the lockdowns, the overall rates of employment have remained relatively unchanged (except for a small decrease in those aged 65 and older). Additionally, the implementation of the vaccine campaign (except for men) did not affect employment rates. This means that it is highly unlikely a confounding variable from changes in employment opportunities from the lockdowns could account for the marked increase in disability seen immediately following the mass vaccination campaigns. That means the only remaining alternative explanation is a rise in disability being due to a rise in long haul Covid.
Long Haul Covid
One of the most common counter arguments I have seen to this point is that the actual cause of this increase in disability is long haul covid. While many people will try to argue it, this cannot be argued because the increase in disability was not present for the initial year of the pandemic when long haul covid was already occurring.
Let’s briefly look at the history of this disorder (per wikipedia). Pay attention to the areas in bold.
Long COVID is a patient-created term which was reportedly first used in May 2020 as a hashtag on Twitter by Elisa Perego, an archaeologist at University College London….Long COVID has no single, strict definition…It can be difficult to determine whether an individual's set of ongoing symptoms represents a normal, prolonged convalescence, or extended 'long COVID'.
In February 2021, the U.S. National Institutes of Health (NIH) director Francis Collins indicated long COVID symptoms for individuals who "don't recover fully over a period of a few weeks" be collectively referred to as "Post-Acute Sequelae of SARS-CoV-2 Infection" (PASC). The NIH listed long COVID symptoms of fatigue, shortness of breath, brain fog, sleep disorders, intermittent fevers, gastrointestinal symptoms, anxiety, and depression. Symptoms can persist for months and can range from mild to incapacitating, with new symptoms arising well after the time of infection.
The World Health Organization (WHO) established a clinical case definition in October 2021, published in the journal The Lancet Infectious Diseases: “post-COVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset, with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. Common symptoms include, but are not limited to, fatigue, shortness of breath, and cognitive dysfunction, and generally have an impact on everyday functioning. Symptoms might be new onset following initial recovery from an acute COVID-19 episode or persist from the initial illness.”
If you remember not too far back, one of the primary reasons that was cited for why you had to get vaccinated was how terrible long haul Covid could be and that the vaccines would either prevent or treat this condition (which ultimately proved false). To this point, I still distinctly remember many physician colleagues of child bearing age cite the terror of this disorder as the reason for why they had to ignore my advice and get vaccinated.
If you observe the timeline of this disease, you can see that it was officially recognized by the NIH immediately following the vaccine roll out, and formalized by the WHO once chronic injuries from vaccination began to mount. At this point in time, it appears that a large number of vaccine injuries are being erroneously classified as “long haul COVID.” A key point in this definition is that it applies to illnesses where “no other cause can be identified” (remember, vaccines can never cause harm) and for cases where the illness spontaneously emerged months after the illness occurred, which often coincides with the time of vaccination.
It is extremely common in the unfalsifiable belief structure of Western Medicine to classify an injury from a medication as actually being due to a deficiency of that medication. One of the best (and sadly very common) examples discussed within this article is that the psychiatric disorders frequently caused by antidepressants are interpreted as these medications protecting you from pre-existing mental illness, leading to more medications being given and catastrophic complications arising.
The symptoms of long haul Covid and Covid vaccine injuries have a significant overlap and respond to similar treatments. Notice how almost every symptom listed above within the diagnostic criteria for long haul covid directly overlaps with symptoms commonly reported for vaccination. To this point, the NIH was fully aware of this by early 2021, as they were using the same scale used to evaluate long haul Covid to evaluate potential vaccine injuries, which the NIH then recognized as vaccine injuries in their scientific publication on those patients.
Given the enormous political pressure to have a way to dismiss these injuries and continue incentivizing widespread vaccination, it is reasonable to assume this erroneous classification like the one employed to dismiss antidepressant injuries would be the default solution. The overlap in the symptoms between these two conditions makes it very easy to trick gullible people.
To that point, I and others have seen countless cases of individuals both online and in person reporting classic descriptions of vaccine injuries, admitting they have been repeatedly vaccinated, and citing their horrific experience with long-haul Covid as a reason why it is crucial for everyone to be vaccinated. Similarly, I have seen cases of doctors labeling vaccine injuries as “long haul covid following vaccination” in order to have a politically acceptable way to get recognition for their patient’s vaccine injuries.
It is also possible the vaccines have dramatically increased individual susceptibility to COVID, as discussed in this recent article, which shows this effect of mass vaccination was abundantly clear from the existing science on the mRNA vaccines before they entered the market. However, even if increasing long haul COVID is accounting for the rise in disability, that still means the increase in disability is ultimately due to the vaccines as they increased the likelihood of long haul Covid occurring within the population.
Disability versus receiving Disability Payments:
A common discussion that has come up with this dataset is whether it means millions will go into disability and receive SSI. Fundamentally, there is no way to know because there will likely be a 4 year lag between individuals entering the disability program following permanent disability from the COVID vaccines and it showing up in a publicly available dataset. and most people who pursue disability do not receive it despite spending years going through the process. I do believe a spike on individuals on disability is likely to occur (although it will be to a smaller degree than that within this dataset, as many continued working despite disability).
To illustrate why I believe many with vaccine injuries will eventually end up on disability, I will briefly share some (revised) thought from the previous article on this topic:
Early in my medical practice, I elected to work with individuals seeking disability.
While a few people I saw were suffering from self-created problems and some were either faking their condition or exaggerating their disability for money (which is the typical lens disability claimants are seen through by doctors), I found the majority had been through significant hardship that resulted in a life impairing disability (some of their experiences were pretty horrific). I took this as a sign a lot of vetting was done by the state before they were sent to me.
In many of these cases, I felt if the individual had been my patient, they would not have arrived at the place they needed to seek disability. Many of them either had iatrogenic complications from the poorer quality of medical care that individuals in state insurance programs like Medicaid have access to, and had problems that would be relatively fixable within a more integrative model of medical care if they had had access to one.
A frequent topic of discussion with my colleagues was whether granting someone disability was ultimately a harmful thing to do since it removes their motivation to address their illness. This is important because in almost all cases, being disabled and receiving disability is a far worse life than not being disabled and having employment. I always kept this in mind when I evaluated these claimants, and ultimately recommended disability for many of them.
I found the majority of claimants I saw did not want to be disabled (this has also been the experience of some of my readers), had tried over and over to get better, hated going through the process and were only doing this because they had no other choice left. Many will also often choose to commit suicide rather than live a life of disability (this is one reason these disabilities lead to death). It also made me particularly sad that many of them said I was one of the first doctors they met who treated them as a human being, something I once again view as a consequence of my working in a socioeconomically impoverished rural area where these patients only had access to the inferior quality of medical care afforded by state medical insurance.
From that job, I came to view the disability process as the last stop on the train for individuals who had been failed by the system. Due to the legal requirements of providing an impartial medical evaluation, I was not allowed to provide any type of medical advice to these individuals and I eventually quit because it just made me depressed and there was nothing I could do to help the people I saw.
As I thought it over while initially writing this article, I realized a sizable portion of the disability claimants I saw had conditions that had a significant overlap with the common permanent complications of COVID-19 vaccinations such as crippling autoimmune conditions, severe neurological disorders and heart failure, making them unable to perform basic tasks that would be required at a labor site.
I have read through reports in a variety of support groups for individuals with permanent injuries from the COVID vaccines and I believe many of them would qualify for disability if they were to pursue the case. Their conditions resemble a subset of the disability claimants I worked with, although in general their conditions are much more severe.
My general impression from working with a large number of patients with chronic illnesses (particularly iatrogenic illnesses) is that they typically file for disability at a much lower rate than individuals with other equally disabling conditions. These patients do not want disability and if they file for it, they only file for it as a last resort.
Unfortunately, it is for all intents and purposes impossible to get compensated for a COVID vaccine injury. To my knowledge, despite thousands of claims being filed and a promise at the start of the pandemic that vaccine injuries would be taken care of, there has not yet been a compensation claim for a COVID vaccine reaction awarded in the United States. As a result, disability status is often the only avenue these patients have.
Conclusion:
This data set is critically important because it will likely be one of the only ways to quantify the chronic complications of the Covid vaccinations on the American population. Likewise, I hope the case has been made that the Covid vaccines are the cause of this trend until proven otherwise.
One of the most concerning things about the trends seen here is that it they have not yet leveled off, which is somewhat congruent with chronic Covid vaccine injuries worsening over time and often following successive booster shots.
Over the last year and a half, a variety of very bad policy decisions have been made which have decimated the American economy in a manner most of us have never seen in our lifetimes. When I was younger, I repeatedly read of cases where the 1% allegedly crashed the economy so they could buy everything out for a cheap amount and steal the wealth from the 99%. I was ultimately not sure what to make of these ideas since they fell under the umbrella of "conspiracy theories."
Nonetheless, I fear that something very similar is happening right now. At this point in time, large portions of the economy are no longer working (for instance there are shortages throughout the supply chain), and one contributing factor for this has been a lack of available labor. Given that many of these individuals with newfound disability are still working, that suggests that many workers in the labor force cannot fully do their jobs, and as a result, despite being employed, that is making the economy partially grind to a halt. Consider for example the recent cancellation of thousands of flights over Memorial Day weekend due to a pilot shortage (pilots are particularly sensitive to vaccine injuries and I know multiple pilots who can no longer fly because of their vaccine injuries).
Once economies grind to a halt, it is very difficult to restart them. If you study the history of Russia and the ex-soviet republics’ economies after the Soviet Union collapsed, it took decades for them to recover from the severe consequences of having to rebuild an economy from scratch.
As this trend is continuing to worsen, based upon the financial slack within the economic system dissipating, the injuries from the vaccines progressively worsening, and the potential for a very bad Covid season this winter, I am genuinely concerned about what will happen with the American economy and that we are on the verge of entering an era of economic feudalism.
One of the major points that Ed Dowd made was that while the upper class does not care about the well-being of the American people, they do care about the well-being of the financial markets. For this reason, I believe focusing upon the economic consequences of the vaccination program is likely to be the most effective path for ending it.
I sincerely appreciate the work other authors in this community have done over the last few days to further delve into this data. At this point in time, I still feel we have only scratched the surface, and I once again humbly request anyone else able to further analyze these data sets to do so. Thank you for taking the time to read this and sharing it with others who can bring attention to this critical issue.
As a (now retired) attorney with some professional experience with the SSDI system, and some personal experience in applying for SSDI due to a medical condition (and winning a ‘closed period award’ for the length of time the condition prevented me from working) let me add a couple data points.
First, on historical average, only 22% of individuals who file an application ultimately get approved.
Second, on appeal after a claim is denied, about 13% of those who appeal ultimately get approved.
Third, on appeal (after the initial denial, and the 2nd denial) to an Administrative Law Judge about 60% of those who take it to that stage get approved. But, that represents only about 2% of those who made an initial claim. That is because most claims are abandoned before they get to the point where the case is heard by a judge. The process is miserable, demeaning, and the goal of the system is to deny the claim.
Fourth, for the vast majority of those who ultimately get approved, it can take years. From the date I filed my initial claim, until my hearing date, 4 years and 3 months elapsed. 3 more months of waiting for a decision and then after the Judge approved the award, another 5 months elapsed before SSA paid the award. So in total, it took 5 years from the time I filed until I received the award. In addition, I did not file my initial claim until 18 months after the disability occurred. So from the date I became disabled (under the legal definition and based on the court concurrence as to the date disability began), 6.5 years elapsed before I received the award (which was a single lump sum). By that time, my condition had been treated over a period of 3 years and I had been back to work for 2 years.
If you look at the statistics from 2009-17, the % of approvals was trending down. If my recollection is correct, during those years the % approved either stayed flat or declined every year. They rose slightly and/or stayed flat up until 2021 and are now on the rise, as pointed out in the article.
So the point to all of the above is threefold. First, more than 75% of applicants who file a claim are denied. Second, the process is miserable and takes 2 years or more to complete. Third, if indeed those who are attributing the rise to the jab are correct, we are only seeing the tip of the iceberg. My own personal experience and my legal experience allows me to say with certainty that a high percentage of valid claims are abandoned along the way…because the process itself, and the way lawyers are compensated is designed to deny claims and ultimately force people to give up.
Given the length of time it can take to go through the process, and the massive backlog that exists in nearly every jurisdiction for a hearing before an ALJ, we should expect to see a continued rise in both initial applications and approvals.
A thorough analysis would need to look at historical data for applications, approvals (at the various stages), and the medical conditions for which approvals were granted. The data is all public, although it would take a massive effort to find it, import it, and ultimately analyze it to determine if what we are seeing on the surface can be proven with the historical data.
AMD, if you would like someone to analyze the VAERS database for the stroke pokes, I can do that for you. The data is downloadable and importable into a queryable database which allows for extensive analysis of the horrific damage and death caused by the COVID vaccines.
Here is an example of a query I ran for someone last October - they wanted all the COVID entries for the keyword 'nightmare':
http://tritorch.com/degradation/VAERSNightmareEntries.htm
Let me know if this is something you are interested in.